ent in primary care - دانشگاه آزاد اسلامی...
TRANSCRIPT

ENT inPrimary Care
A Concise Guide
Edoardo CervoniKim Leech
123

ENT in Primary Care

Edoardo Cervoni • Kim Leech
ENT in Primary Care
A Concise Guide
ISBN 978-3-319-51986-9 ISBN 978-3-319-51987-6 (eBook)DOI 10.1007/978-3-319-51987-6
Library of Congress Control Number: 2017935364
© Springer International Publishing AG 2017This work is subject to copyright. All rights are reserved by the Publisher, whether the whole or part of the material is concerned, specifically the rights of translation, reprinting, reuse of illustrations, recitation, broadcasting, reproduction on microfilms or in any other physical way, and transmission or information storage and retrieval, electronic adaptation, computer software, or by similar or dissimilar methodology now known or hereafter developed.The use of general descriptive names, registered names, trademarks, service marks, etc. in this publication does not imply, even in the absence of a specific statement, that such names are exempt from the relevant protective laws and regulations and therefore free for general use.The publisher, the authors and the editors are safe to assume that the advice and information in this book are believed to be true and accurate at the date of publication. Neither the publisher nor the authors or the editors give a warranty, express or implied, with respect to the material contained herein or for any errors or omissions that may have been made. The publisher remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Printed on acid-free paper
This Springer imprint is published by Springer NatureThe registered company is Springer International Publishing AGThe registered company address is: Gewerbestrasse 11, 6330 Cham, Switzerland
Edoardo CervoniENT SpecialistCentral Park SurgeryLeylandLancashireUK
Kim LeechAdvanced Nurse PractitionerCentral Park SurgeryLeylandLancashireUK

v
Preface
ENT disease represents a significant percentage of the day-to-day cases seen in primary care – approximately 1 in 4 consultations. Research suggests this figure is between 23% (Cross and Rimmer 2007) and 25% (Lloyd et al. 2014) of all primary care presen-tations. Unfortunately, the educational curriculum of the medical schools and family doctor/GP training programs do not parallel the high prevalence of ENT disease. As a result, health care professionals such as GPs and nurse practitioners (NPs) may refer many patients to secondary care with ENT problems when they could handle them in primary care. It is legitimate to assume that a better understanding of the clinical his-tory, clinical examination and accurate management of ENT disease might lead to a better management of the ENT patient and a reduction in the number of specialist appointments requested in general practice. This book is not a complete compendium of otolaryngology. Instead, it is intended to be a practical guide for the primary care provider. The topics covered are common and the ENT disease management is the one you would expect to take place in a primary care setting. The use of ENT diagnostic instrumentation refers to what should be available in any GP surgery. We think this book is a useful addition to the library of medical students, GPs in training, board certi-fied family physicians and NPs. Its format is simple and the text is minimal. The topics are organized in such a way as to highlight when a patient should be sent to a specialist immediately and when they can be efficiently managed in general practice.
Leyland, Lancashire, UK Edoardo CervoniLeyland, Lancashire, UK Kim Leech
References
1. Cross S, Rimmer M (2007) Nurse practitioner manual of clinical skills, 2nd edn. Elsevier, London
2. Lloyd S, Tan ZE, Taube MA, Doshi J (2014) Development of an ENT undergraduate curricu-lum using a Delphi survey. Clin Otolaryngol 39:281–288

vii
Acknowledgements
We would wish to personally thank the following people for their contributions to our inspiration and knowledge and other help in creating this book.
Dr. Cervoni would like to thank the many people who have brought him this far. They are his relatives, teachers, and colleagues he had the pleasure to work with over the years, but especially his very much loved children, Oliver Alessandro and Francesca, with the infinite love that they give every day.
Mrs. Kim Leech would like to acknowledge her parents, Mark and Brenda Jagger, for her upbringing, their support and encouragement, her husband, Ashley, for his continued support and constant belief and her beautiful daughter, Maddison.
Finally, we would like to thank the patients for their trust and for having shared their experience of living with the most diverse ENT pathologies.
ix
Abbreviations
AIDS Acquired immune deficiency syndromeAOM Acute otitis mediaBD Twice a dayBPPV Benign paroxysmal positional vertigoCHL Conductive hearing lossCSF Cerebrospinal fluidEAC External auditory canalENT Ears, nose and throatHIV Human immunodeficiency virusNSAID Nonsteroidal anti-inflammatory drugRAST Radioallergosorbent testSNHL Sensorineural hearing lossTDS Three times a dayTIA Transient ischaemic attackTMJ Temporomandibular joint
xi
Contents
1 ENTAnamnesis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1The ENT Consultation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
ENT History . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1History of Presenting Complaint . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2Past Medical History . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2Drug History . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2Social History . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
2 Otology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5Organ Targeted History . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
The Ear . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5Ear Equipment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
Otoscope . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6Tuning Forks . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8Frenzel Goggles . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8Ear Syringe . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
Otological Examination . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10Otalgia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11Causes of Referred Otalgia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
Local Causes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12Otitis Externa . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12Acute Otitis Media . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
Consequences of Viral and Bacterial Otitis Media . . . . . . . . . . . . . . . . . 16Ear Secretions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
Otitis Externa . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19Middle Ear Pathology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19Trauma or Foreign Body . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
xii
Management of Ear Secretions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19Perforation of Tympanic Membrane . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20Cholesteatoma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22Child Deafness . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
With Otalgia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23Without Otalgia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
Adult Deafness . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25Hearing Tests . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
Rinne Test . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25Weber Test . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27Contraindications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29Precautions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29Evaluation of Auditory Function by GP . . . . . . . . . . . . . . . . . . . . . . . . . 30Services for Patients with Hearing Loss . . . . . . . . . . . . . . . . . . . . . . . . . 30
Vestibular System . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31Smooth Pursuit . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31Saccades . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31Head-Shaking Nystagmus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31Fukuda Stepping Test . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32Hallpike Test . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32
Tinnitus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33Subjective Tinnitus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33Objective Tinnitus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
Vertigo . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33Objective Vertigo . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36Subjective Vertigo . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37
Fistula Test . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37Benign Paroxysmal Positional Vertigo (BPPV) . . . . . . . . . . . . . . . . . . . 38
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 38
3 Rhinology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39The Nose . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39Nose Assessment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40
Dentist Mirror or a Cosmetic Mirror . . . . . . . . . . . . . . . . . . . . . . . . . . . 41Silver Nitrate Sticks . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41Nose Inspection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42
Epistaxis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42Epistaxis in the Child . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42Epistaxis in Adults . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44Nasal Obstruction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45Allergic Rhinitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45Vasomotor Rhinitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47Nasal Polyps . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 48Allergy Testing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50
Contents
xiii
Septal Deviation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50Inspiratory Nasal Valve Collapse . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50Nasopharyngeal Obstruction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50Sinusitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52
Recurring Rhinosinusitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54
4 Laryngology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 55The Throat . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 55Mouth and Throat Assessment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 56Sore Throat . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 57
Pharyngitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 57Other Causes of Pharyngitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 57Tonsillitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 58
Hoarseness . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 62Dysphagia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 63
Acute Dysphagia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 63Progressive Dysphagia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64Other Causes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64Globus Pharyngeus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64
Snoring . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 65Key Anamnestic Points . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 66
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 67
5 HeadandNeck . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 69The Oral Cavity and the Neck. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 69Neck Lump . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 69Salivary Gland Lump . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 70Facial Palsy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 70
Herpes Zoster . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 70Bell’s Palsy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 72Other Causes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 73References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 73
6 Post-operativeORL . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 75Adenoidectomy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 75Trans-tympanic Tubes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 75Nasal Surgery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 76Tonsillectomy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 76Oncology ORL . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 77
Neoplastic Suspect in ENT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 77
7 Pharmacology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 79Antibiotic Prescribing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 79
Common ENT Antibiotic Prescribing in Primary Care . . . . . . . . . . . . . 79
Contents

xiv
Common Prescriptions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 79Rhinitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 79Vertigo . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 80Otitis Externa . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 80Sore Throat/Mouth . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 80Glue Ear . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 82
Reference . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 82
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 83
Index . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 85
Contents
1© Springer International Publishing AG 2017 E. Cervoni, K. Leech, ENT in Primary Care, DOI 10.1007/978-3-319-51987-6_1
Chapter 1ENT Anamnesis
The ENT Consultation
There are many well-documented consultation models such as Helman’s Folk Model (1981), Pendleton et al. (1984), Neighbour (1987) and Calgary-Cambridge (1996) to name but a few. Many of which, designed in Primary Care. The use of consultation models helps to add structure to the consultation and ensure all relevant aspects are explored. It is not the intention of this book to specify a preferred model or whether a clinician devises their own model. However, there is a common factor in that all models which includes presenting complaint, past medical history, drug history, social history, examination, differential diagnosis, investigations and treatment.
�ENT�History
Undertaking an effective clinical history is an essential part of the ENT consultation, as it is with any aspect of medical practice. The content explored will vary from clinician to clinician and depend upon the patient’s past medical history, social history and drug history, as well as previous experiences. It is essential that the clinician has good com-munication skills, both verbal and non-verbal and may notice any cues given by the patient. Smith (2003) suggests that if the clinician listens to the patient, they will tell you the diagnosis. The information collected in the history will enable the clinician to target their questions to a certain line of enquiry and will guide the clinician to which investigations may be appropriate. During the history taking, the physician-patient relationship takes shape. It allows the clinician to get to know their patient, gain their confidence and trust and develop an understanding of any external influences that might affect their health. It also allows the clinician to explore the patient’s ideas, con-cerns and expectations. This is a crucial element of the clinical encounter for several reasons, including understanding of their condition and compliance to treatments.
2
�History�of�Presenting�Complaint
When a patient presents with an ENT complaint, it is important to ascertain factors such as onset, frequency and duration of symptoms, whether the patient has any other associated symptoms and what treatments, if any they have already tried. At this point, the physician should address questions specific to the system or systems. In relation to ENT, whether the patient has experienced any dizziness, congestion, decreased smell, hoarseness, odynophagia, swellings or lymphadenopathy, pain or discharge (to name a few ENT symptoms.) Corbridge (2011) suggests that, in gen-eral, unilateral symptoms should increase the clinician’s suspicion because most of the conditions that have serious consequences, such as tumours and cancers, are unilateral, at least initially.
�Past�Medical�History
The clinician should ascertain a patient’s past medical history. This may help the clinician determine if it is a recurring health problem. A history should include allergies. This is especially important in ENT presentations. Any history of asthma or respiratory conditions, neurology or rheumatology may also be significant. Undertaking a past medical history may affect a patient’s treatment plan or options for surgery and anaesthesia.
�Drug�History
Reviewing patient prescribed medications may alert a clinician to pre-existing ENT complaints or the presenting complaint may be because of a current medication. For example, a patient who presents with epistaxis who is prescribed apixaban or a patient presenting with hearing loss or tinnitus who is prescribed a macrolide or maybe quinine. A clinician should ascertain if the patient is taking any other medi-cations, prescribed, over-the-counter or otherwise obtained.
�Social�History
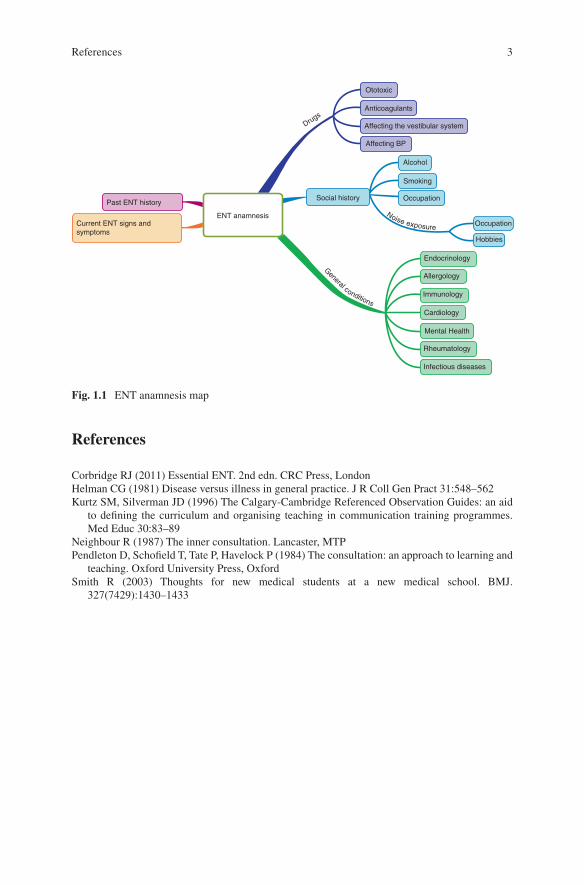
Many clinicians utilise physician-centred approaches to social history, which can be limiting to smoking, drinking alcohol and the use of drugs. However patient-centred approaches are often more in-depth and incorporate a wider range of social factors such as place of birth, qualifications/education, occupation, home environment, diet, exercise, sexual history, religion, tobacco, alcohol and drug use. In some cases, the details of the patient’s household may also be relevant (Fig. 1.1).
1 ENT Anamnesis
3
References
Corbridge RJ (2011) Essential ENT. 2nd edn. CRC Press, LondonHelman CG (1981) Disease versus illness in general practice. J R Coll Gen Pract 31:548–562Kurtz SM, Silverman JD (1996) The Calgary-Cambridge Referenced Observation Guides: an aid
to defining the curriculum and organising teaching in communication training programmes. Med Educ 30:83–89
Neighbour R (1987) The inner consultation. Lancaster, MTPPendleton D, Schofield T, Tate P, Havelock P (1984) The consultation: an approach to learning and
teaching. Oxford University Press, OxfordSmith R (2003) Thoughts for new medical students at a new medical school. BMJ.
327(7429):1430–1433
Past ENT history
Current ENT signs andsymptoms
ENT anamnesis
Social history
Ototoxic
Anticoagulants
Affecting the vestibular system
Affecting BP
Alcohol
Smoking
Occupation
Occupation
Hobbies
Endocrinology
Allergology
Drugs
General conditionsImmunology
Cardiology
Mental Health
Rheumatology
Infectious diseases
Noise exposure
Fig. 1.1 ENT anamnesis map
References

5© Springer International Publishing AG 2017 E. Cervoni, K. Leech, ENT in Primary Care, DOI 10.1007/978-3-319-51987-6_2
Chapter 2Otology
Organ Targeted History
The Ear
Hearing loss is a very common presenting symptom of ear disease. It is estimated that ten million people in the UK suffer with this complaint. Hearing loss can occur in the external, middle or inner ear and can be conductive, sensorineural in nature or both. The clinician should ask the patient how long they have been experiencing the symptoms, was it a sudden loss or gradual and whether it is unilateral or bilateral. Unilateral loss could indicate important pathology. Family history of hearing loss can be relevant, and gaining an understanding of any professional or recreational noise the patient has been exposed to could be significant. In a child, it is important to enquire about previous infections, trauma at birth or anoxia, and other medical conditions. Ear problems can very often result in otalgia (ear pain).
Due to the distribution of cranial nerves and shared innervations such as of tem-poromandibular joint, mouth, teeth, salivary glands and throat; otalgia can quite often be because of referred pain. Therefore, the clinician needs to determine if the pain is from a direct or a referred cause. The clinician should explore whether the pain is acute or chronic and whether it has been a recurrent problem. The patient may describe the pain as sharp, dull, a discomfort, a deep penetrating pain or diffuse ante-rior pain. The clinician should ascertain what the exacerbating and alleviating factors are and whether there are any associated symptoms such as fever, congestion, nasal or ear discharge, sinus pain or headaches. As mentioned, otalgia can be because of referred pain for example tonsillitis. Fifty percent of ear pain is from a dental or TMJ causes, therefore a comprehensive history should assess ear, dental, sinus, jaw, neck, tongue, mouth and neurological disorders that can affect the head and neck.
Otorrhoea is a common presentation in primary care, especially in children. The clinician should ask the patient about onset, duration, amount and quality of otorrhoea. A purulent discharge could indicate infection, whilst a blood-stained
6
otorrhoea may indicate trauma. Likewise, patients with a mucous discharge may have a perforated tympanic membrane and patients with a clear fluid following a head or skull injury could have a CSF leak. A foul-smelling otorrhoea is character-istic of cholesteatoma. However, there are other infections leading to extremely malodorous ear secretion such as infection caused by Proteus. The history should investigate any childhood illness, trauma, foreign bodies, respiratory symptoms, any ENT surgery or excessive exposure to water e.g. swimmers. Associated symp-toms such as hearing loss, tinnitus, pain, vertigo and facial palsy should also be explored. Vertigo and facial palsy associated with otorrhoea require urgent referral.
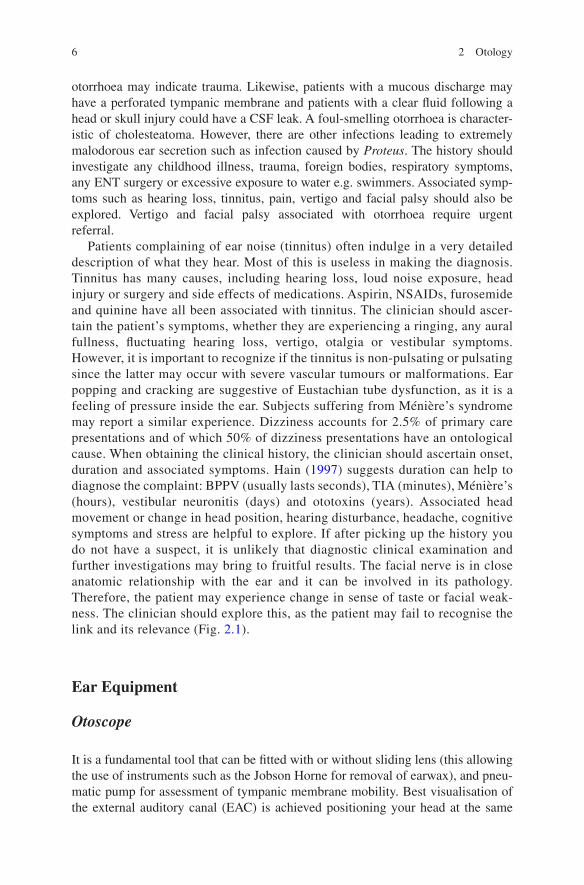
Patients complaining of ear noise (tinnitus) often indulge in a very detailed description of what they hear. Most of this is useless in making the diagnosis. Tinnitus has many causes, including hearing loss, loud noise exposure, head injury or surgery and side effects of medications. Aspirin, NSAIDs, furosemide and quinine have all been associated with tinnitus. The clinician should ascer-tain the patient’s symptoms, whether they are experiencing a ringing, any aural fullness, fluctuating hearing loss, vertigo, otalgia or vestibular symptoms. However, it is important to recognize if the tinnitus is non-pulsating or pulsating since the latter may occur with severe vascular tumours or malformations. Ear popping and cracking are suggestive of Eustachian tube dysfunction, as it is a feeling of pressure inside the ear. Subjects suffering from Ménière’s syndrome may report a similar experience. Dizziness accounts for 2.5% of primary care presentations and of which 50% of dizziness presentations have an ontological cause. When obtaining the clinical history, the clinician should ascertain onset, duration and associated symptoms. Hain (1997) suggests duration can help to diagnose the complaint: BPPV (usually lasts seconds), TIA (minutes), Ménière’s (hours), vestibular neuronitis (days) and ototoxins (years). Associated head movement or change in head position, hearing disturbance, headache, cognitive symptoms and stress are helpful to explore. If after picking up the history you do not have a suspect, it is unlikely that diagnostic clinical examination and further investigations may bring to fruitful results. The facial nerve is in close anatomic relationship with the ear and it can be involved in its pathology. Therefore, the patient may experience change in sense of taste or facial weak-ness. The clinician should explore this, as the patient may fail to recognise the link and its relevance (Fig. 2.1).
Ear Equipment
Otoscope
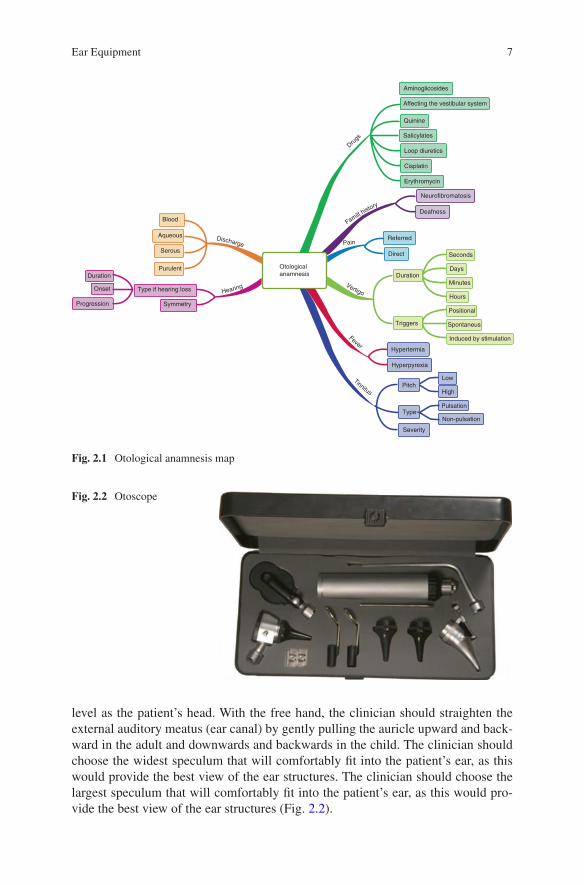
It is a fundamental tool that can be fitted with or without sliding lens (this allowing the use of instruments such as the Jobson Horne for removal of earwax), and pneu-matic pump for assessment of tympanic membrane mobility. Best visualisation of the external auditory canal (EAC) is achieved positioning your head at the same
2 Otology
7
level as the patient’s head. With the free hand, the clinician should straighten the external auditory meatus (ear canal) by gently pulling the auricle upward and back-ward in the adult and downwards and backwards in the child. The clinician should choose the widest speculum that will comfortably fit into the patient’s ear, as this would provide the best view of the ear structures. The clinician should choose the largest speculum that will comfortably fit into the patient’s ear, as this would pro-vide the best view of the ear structures (Fig. 2.2).
Aminoglicosides
Affecting the vestibular system
Quinine
Salicylates
Loop diuretics
Cisplatin
Erythromycin
Neurofibromatosis
Deafness
Referred
Otologicalanamnesis
Symmetry
Type if hearing loss
Blood
Aqueous
Serous
Purulent
Progression
Onset
Duration
Direct
Duration
Seconds
Days
Minutes
Hours
Positional
Spontaneus
Induced by stimulation
Triggers
Hypertermia
Hyperpyrexia
PitchLow
High
Pulsation
Non-pulsationType
Severity
Discharge Pain
Hearing Vertigo
Fever
Tinnitus
Familt history
Drugs
Fig. 2.1 Otological anamnesis map
Fig. 2.2 Otoscope
Ear Equipment

8
Tuning Forks
In ENT, tuning forks are used to assess hearing loss and ascertain whether the hearing loss is conductive or sensorineural in nature. Each tuning fork carries a number (128, 256, 512 and 1024 Hz.) This is the frequency at which the fork vibrates.
Diapason at 512 Hz
The 512 Hz tuning fork is the most effective in the range of clinical diapasons avail-able as the patient may not recognize a lower frequency (128, 256 Hz), and higher frequencies have a shorter duration making the Rinne test difficult to perform. The tuning fork may be made of steel or aluminium, the latter being a much cheaper material, but is suitable to clinical use (Fig. 2.3).
The easiest and most useful hearing tests to perform are the Rinne and the Weber test. The Rinne and Weber test are used to differentiate between conductive hearing loss (CHL) and sensorineural hearing loss (SNHL). Both should be carried out and the Rinne test should be done first. We shall address the details of both tests in a separate section of this book dedicated to hearing evaluation.
Frenzel Goggles
The Frenzel goggles are helpful to assess nystagmus, a condition of involuntary movement of the eyes, the assessment of which is often extremely helpful to diagnose pathologies affecting the vestibular system (Fig. 2.4).
Fig. 2.3 Tuning fork sets
2 Otology
9
Ear Syringe
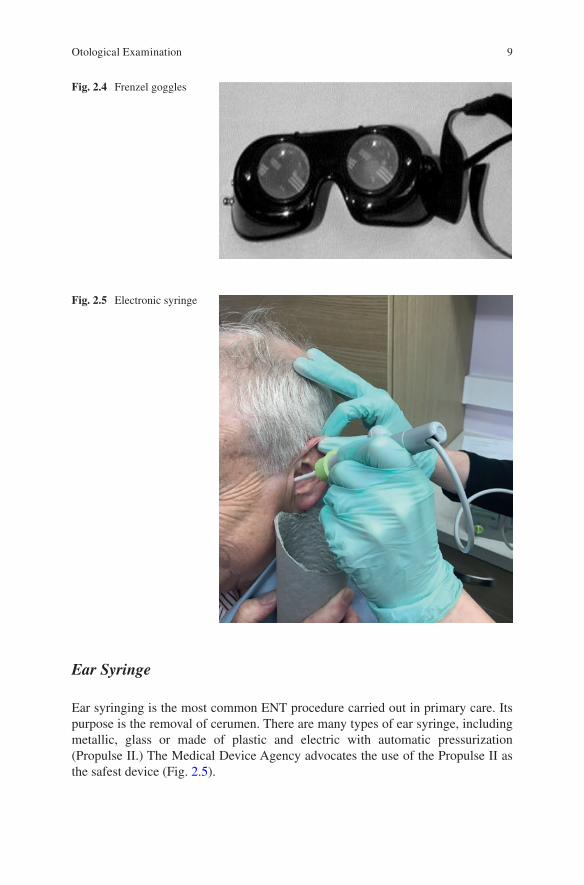
Ear syringing is the most common ENT procedure carried out in primary care. Its purpose is the removal of cerumen. There are many types of ear syringe, including metallic, glass or made of plastic and electric with automatic pressurization (Propulse II.) The Medical Device Agency advocates the use of the Propulse II as the safest device (Fig. 2.5).
Fig. 2.4 Frenzel goggles
Fig. 2.5 Electronic syringe
Otological Examination

10
Otological Examination
In addition to the clinical anamnesis we have described in the previous sections, the complete otological examination comprises a physical examination and testing which includes:
• Inspection• Otoscopy• Removal of cerumen if present• Use of tuning forks• Pneumatic otoscopy/“fistula test”• Vestibular system assessment• Cranial nerve exam• Head and neck exam
It is common practice to examine the unaffected or least affected ear first. This will set a baseline for the clinician to compare the other ear to. The clinician should start by assessing the pinna, reviewing the skin around, behind and adjacent to it.
Evaluate for the presence of scars, as this may be significant in framing the clini-cal scenario (Figs. 2.6 and 2.7).
The clinician should assess whether there is a deformity of the pinna, or any skin lesions.The clinician should then assess the appearance of EAC. The otoscope is funda-
mental to this providing magnification and illumination. The otoscope will be used in conjunction with a speculum of the largest size that can fit in the EAC of the patient without causing discomfort. Pulling the pinna upwards and backwards straightens the ear canal, and the clinician should assess:
• Normal findings such as hair, and cerumen• Abnormal findings such as dry flaky skin suggestive of eczema, inflamed or
swollen ear canal, discharge, impacted cerumen or foreign body• The appearance of tympanic membrane – this includes analysing the mobility of
the TM, any retraction pockets, the presence of keratinous accumulations, any erosion of the ossicular chain, any perforations or scars (Fig. 2.8)
Temporalfascia graftingsite
Graftingsite
Retroauricularapproach
Retroauricularapproach
Fig. 2.6 Surgical scars
2 Otology

11
Otalgia
Earache is a common presenting complaint in primary care. Often, but not always, it is indicative of an ear infection. When the otoscopic examination is normal, the ear pain is a referred pain. In addition, the healthcare professional has to be aware that catarrhal otitis can lead to chronic acute otitis media and vice versa. When con-sidering an ear infection, in conjunction with the clinical history, the diagnostic elements illustrated in the following paragraphs are of extreme relevance.
Causes of Referred Otalgia
There are several possible causes of otalgia. Among them are:
• Tonsillitis• Mononucleosis
Helix
Scaphoid fossa
Crura of antihelix
Concha cava
Antihelix
Antitragus
Lobule
Triangular fossa
Crus of helix
Tragus
Fig. 2.7 The ear
Fig. 2.8 Intact tympanic membrane
Causes of Referred Otalgia

12
• TMJ syndrome• Cervical spondylosis• Cancers of the throat, mouth and nasopharynx• Odontogenic
In the following sections we shall explore the local causes of otalgia, whilst some of the conditions causing referred otalgia will be discussed in other sections of the book instead.
Local Causes
The main local causes of otalgia are trauma, or pathology of the pinna, otitis externa, and otitis media.
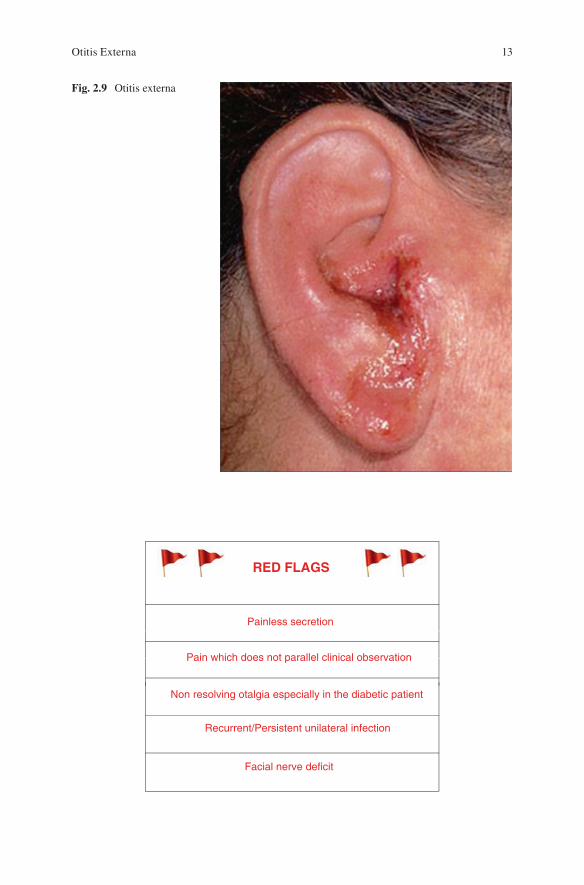
Otitis Externa (Fig. 2.9)
Clinical PresentationOtitis externa may be due to acute or chronic eczema, psoriasis, seborrhoeic derma-titis, skin infection of the EAC or pinna.
Examination• Itching and/or ear pain• Watery secretion• Some deafness, or blocked ear• Pain that radiates towards neck and adenopathy
Clinical Management• Antibiotic and topical steroid drops for 5 days• Cream and/or antibiotic drops with steroid and gauze• Ear swab for microbiological examination• Diabetic control if applicable• Consider shampooing• Acetic acid in drops or spray• Use of ear plugs to avoid water entering the ear canal
Key PointsRefer to a specialist if marked stenosis of the EAC, or in case of ear obstruction due to exostosis of the EAC, keratin debris, facial cellulitis, persistent symp-toms resistant to medical treatment, and infections interfering with the use of hearing devices. Other causes of otitis externa are boils, which are very painful especially to traction of the pinna; shingles; myringitis bullosa haemorrhagica; and perichondritis, which require hospitalization for appropriate therapy.
2 Otology
13
RED FLAGS
Painless secretion
Pain which does not parallel clinical observation
Non resolving otalgia especially in the diabetic patient
Recurrent/Persistent unilateral infection
Facial nerve deficit
Fig. 2.9 Otitis externa
Otitis Externa

14
Acute Otitis Media
The acute otitis media, or AOM, may be viral or bacterial.
Viral Otitis Media (Fig. 2.10)
Clinical PresentationViral otitis media may be secondary to upper respiratory tract infection, there may be the absence of fever, or mildly raised temperature and one of both ears may be affected. Children may present in combination with vomiting and diarrhoea.
Examination• Hyperaemia of the handle of the hammer• Bubbles and fluid behind a tympanic membrane flushed, but intact• The absence or decrease of luminous triangle• Hypervascularisation of the tympanic membrane
Clinical Management• Acetaminophen during the 24 h, when the pain is more accenuated.• NSAIDs, such as ibuprofen, may be particularly helpful at night.• If the ear pain persists for more than 24 h, review pain control and
consider antibiotic therapy, particularly if fever, age less than 3 years old, yellow tinged middle ear secretions, or perforation of the tympanic membrane.
• Check in 2 weeks to prevent relapse.
Fig. 2.10 Viral otitis media
2 Otology
15
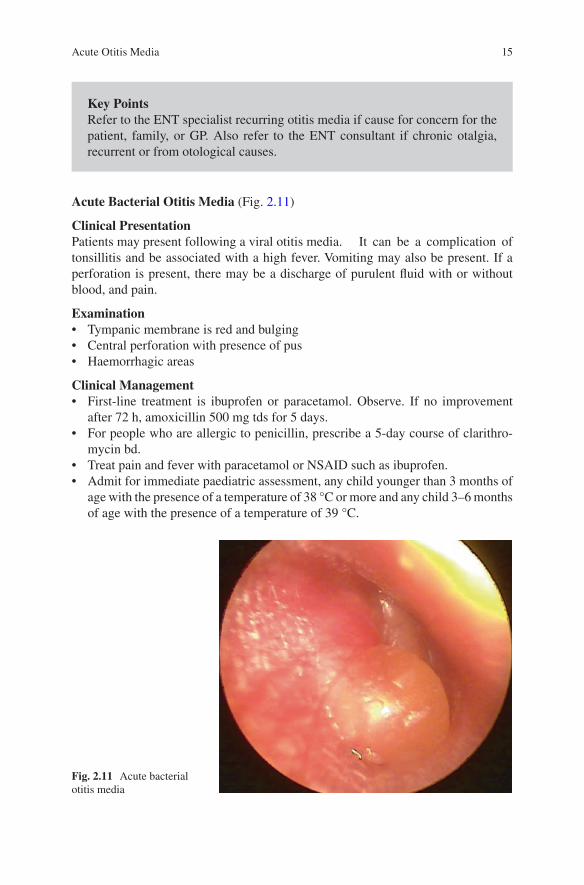
Acute Bacterial Otitis Media (Fig. 2.11)
Clinical PresentationPatients may present following a viral otitis media. It can be a complication of tonsillitis and be associated with a high fever. Vomiting may also be present. If a perforation is present, there may be a discharge of purulent fluid with or without blood, and pain.
Examination• Tympanic membrane is red and bulging• Central perforation with presence of pus• Haemorrhagic areas
Clinical Management• First-line treatment is ibuprofen or paracetamol. Observe. If no improvement
after 72 h, amoxicillin 500 mg tds for 5 days.• For people who are allergic to penicillin, prescribe a 5-day course of clarithro-
mycin bd.• Treat pain and fever with paracetamol or NSAID such as ibuprofen.• Admit for immediate paediatric assessment, any child younger than 3 months of
age with the presence of a temperature of 38 °C or more and any child 3–6 months of age with the presence of a temperature of 39 °C.
Key PointsRefer to the ENT specialist recurring otitis media if cause for concern for the patient, family, or GP. Also refer to the ENT consultant if chronic otalgia, recurrent or from otological causes.
Fig. 2.11 Acute bacterial otitis media
Acute Otitis Media
16
• Admit for immediate specialist assessment, adults and children with acute com-plications of acute otitis media such as meningitis, mastoiditis, or facial nerve paralysis.
• Consider admitting patients who are systemically unwell.• Consider admitting people with significant, persistent symptoms on high-dose
amoxicillin/clavulanic acid, or azithromycin.
Consequences of Viral and Bacterial Otitis Media
• Full resolution: no action to follow.• Persistent otalgia: refer to specialist.• Serous otitis media: if asymptomatic, observation; if painful or cause of deaf-
ness, refer to ENT.• If associated with acute tympanic membrane perforation, suggest avoiding the
entrance of water in the ear canal and review the patient in 1 month; refer to the specialist if the perforation has not closed.
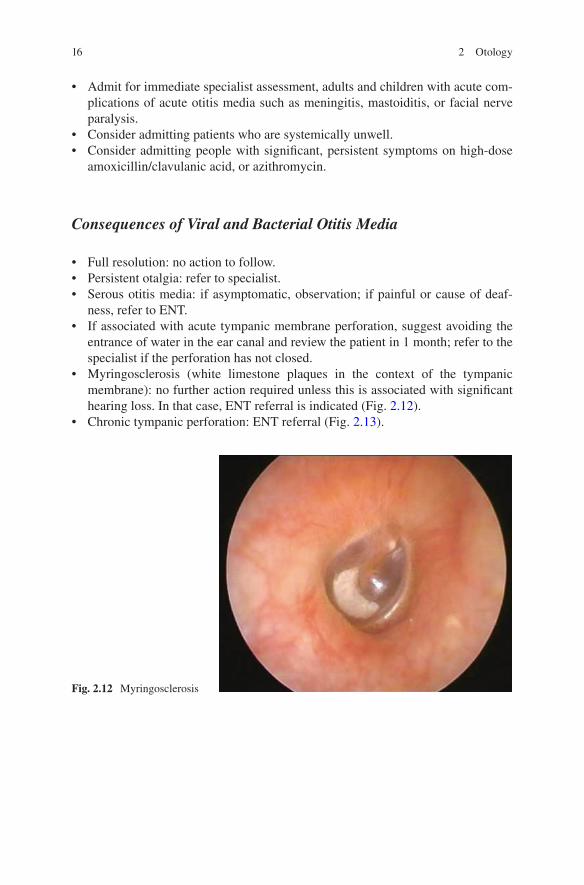
• Myringosclerosis (white limestone plaques in the context of the tympanic membrane): no further action required unless this is associated with significant hearing loss. In that case, ENT referral is indicated (Fig. 2.12).
• Chronic tympanic perforation: ENT referral (Fig. 2.13).
Fig. 2.12 Myringosclerosis
2 Otology

17
Key PointsAcute otitis media in adults is uncommon in those subjects that have not been already prone at a young age and as such it should be followed-up carefully. Refer to specialist in the absence of a speedy resolution, or in case of recurrence.Any child younger than 2 years old that is unwell needs otoscopic examination.The level of concern of relatives often goes in parallel with the severity of the ENT pathology.Treating otitis media with analgesia for 24 h does not harm the patient’s health.An exudative otitis media in an adult without previous history of ontological problems should trigger special attention.A mastoid abscess should not be diagnosed in the presence of normal tym-panic membrane, or almost normal.A mastoiditis requires hospital admission if evidence of complications.
Fig. 2.13 Chronic tympanic membrane perforation
Acute Otitis Media

18
RED FLAGS
Children < 3 monthes of age with a temperature > 38ºC
Children 3-6 months of age with a temperature > 39ºC
Swelling or pain to the mastoid process
Symptoms and signs suggestive of meningitis
Facial nerve deficit
Ear Secretions (Fig. 2.14)
The presence of ear discharge is a common finding in general practice. The presence of secretions in the EAC does challenge the clinician’s ability to visualize the tym-panic membrane without the help of a suctioning device. As such, the clinician should be particularly careful in their proposed management. In the presence of history of ear surgery, or surgical incision, the patient should be referred to the ENT specialist. Ear discharge, or otorrhoea, may be due to several causes, ranging from an otitis externa to pathology of the middle ear.
Fig. 2.14 Otorrhoea
2 Otology

19
Otitis Externa
We have already discussed otitis externa as being a cause of otalgia. In fact, earache is the prominent feature of otitis externa and the presence of discharge in the absence of pain should suggest the possibility of a perforated otitis media instead. Otitis externa can be due to a variety of causes, including a trauma, boils, pseudomonas, or rarely a neoplasm. The use of cotton buds is a common trigger of otitis externa. Otitis externa is often associated with pruritus, sensation of ear fullness because of the accumulations of keratin scales and exudate, and a slight hearing loss.
Middle Ear Pathology
It can lead to ear discharge only in the presence of tympanic membrane perforation. Pathologies of the middle ear that can cause discharge include the already discussed AOM, chronic otitis media, some fractures of the temporal bone and granulations of the tympanic membrane.
Trauma or Foreign Body
It is uncommon for a GP to see an ear trauma or a foreign object in the external auditory canal during surgery times. However, should this be the case, a referral to the local A&E Department is generally required. This may not be the case only if the GP can fully visualise the external and middle ear establishing the absence of lesions or foreign bodies. The presence of deafness, tinnitus, or vertigo should warrant further specialist assessment. A GP may also attempt removal of foreign objects by means of ear stringing, or using otoscope and Jobson Horn instrument.
Management of Ear Secretions
Clinical Management• Antibiotic and topical steroid drops for 5 days.• If the patient is diabetic, obtain an ear swab to exclude Pseudomonas aeruginosa
infection which, if present, would demand ENT referral.• Suggest avoiding shampoo, conditioner, swimming, and sauna.• Repeat otoscopic examination if the above measures do not bring benefit.• In the presence of tight and swollen ear canal, use gauze or other guide.• Analgesia.• Oral antibiotics if adenopathy present.• Anti-histamine if itching.• If abundant keratin debris, refer to ENT? cholesteatoma.
Management of Ear Secretions

20
RED FLAGS
Facial nerve injury or deficit of other cranial nerves
Vertigo suggestive of cholesteatoma
Foul-smelling secretion suggestive of cholesteatoma
Previous ontological surgery
Otorrhoea by cerebrospinal fluid leakage
Perforation of Tympanic Membrane (Fig. 2.15)
Tympanic membrane perforations can be handled in the large part by primary care. They occur when a hole or tear develops in the tympanic membrane.
These are divided into:
• Peripheral• Of the attic• Central
Fig. 2.15 Tympanic perforation
2 Otology

21
Each type has different management plans.
Clinical Presentation• Otalgia• Discharge from the ear• Temperature of 38 °C or above• Tinnitus
Examination• Undertake otoscopy to identify a perforation with or without granulation
tissue• Look for retraction pockets and keratinic debris, which may hint the presence of
cholesteamtoma• Be alerted by foul-smelling debris or discharge, which may suggest Pseudomonas
or other bacterial infection
Clinical Management of Central Perforations• Prescription drops if secretions obscure the tympanic membrane. Most antibiotic
ear drops contain aminoglycosides that are ototoxic. They are often still pre-scribed by the ENT consultant, but in primary care the use of non-ototoxic drugs such as ofloxacin drops with or without topical steroid could be preferable. When the perforation is dry, observe and advise patient to avoid getting water in the entrance of the ear canal using cotton with wax or Vaseline.
• Pain relief such as paracetamol or ibuprofen.• Review the patient after 6 weeks.• Very often central perforations resolve spontaneously.
Clinical Management of Peripheral Perforations and Perforation of the Attic• All peripheral perforations and perforations of the attic require ENT referral in
view of the higher risk of chronic middle ear disease and in particular cholesteatoma.
Key PointsConsider referring patient in case of:
• Recurring/persistent otorrhoea• Otalgia resulting from secondary otitis externa• Deafness• Vertigo• Persistent perforation
Perforation of Tympanic Membrane

22
RED FLAGS
Facial nerve deficit
Headache
High fever
Vertigo
Cholesteatoma (Fig. 2.16)
Cholesteatoma is a less common finding in general practice. It occurs when a col-lection of cells grow on the inside of the ear drum. Left untreated, it can damage the structures of the middle ear and lead to deafness, ear infections, vertigo, tinnitus and facial nerve damage.
Clinical PresentationThe presence of symptoms and conditions that should trigger the suspect of choles-teatoma are:
Fig. 2.16 Cholesteatoma
2 Otology

23
• Deafness• Smelly otorrhoea• Otalgia• Facial nerve deficit• Vertigo• Mastoid abscess• Meningitis
Examination• The presence of cholesteatoma is typically suggested by the presence of abun-
dant keratinic debris with or without smelly discharge and tympanic mem-brane perforation. The latter is most common, but it may not be present on occasions such as in the case or a retraction pocket or a congenital cholesteatoma.
Clinical Management• The presence or suspect of cholesteatoma dictates ENT referral for further
management.
Child Deafness
If a parent suspects that his child has difficulty hearing, the GP should consider a request for visiting an ENT specialist. In general, the perception of deafness in a child indicates the presence of bilateral hearing loss. The first question to consider is if deafness is associated with ear pain.
With Otalgia
Consider:
• Acute otitis media• Upper respiratory tract infection
Without Otalgia
Consider:
• Earwax• Bilateral exudative otitis media
Child Deafness

24
• History of pre-, peri-, post-natal complications or that might suggest the pres-ence of sensorineural hearing impairment
• History of meningitis, or severe rash• History of head trauma• Congenital malformations
Examination• Presence of earwax: sodium bicarbonate 5% drops for 48–72 h, eventually fol-
lowed by irrigation of the EAC. However, this would not be advisable in the young child.
• Glue ear which is very common and is determined by:
– Vascularisation of the tympanic membrane – Golden colour of tympanic membrane – Absence of bright reflex triangle – Almost blue reflex of tympanic membrane – Presence of fluid, or air-water levels/bubbles behind an intact tympanic
membrane – Horizontal handle of the hammer
Clinical Management of Deafness with Otalgia• Acetaminophen for 24 h in the presence of acute otitis media• Symptoms lasting longer than 24h, 5 days of antibiotic therapy• If the ear pain resolves but the deafness remains, treat as deafness without ear pain• Note: Nasal drops don’t help
Clinical Management of Deafness Without Otalgia• It is important to get a good clinical history from the relatives and clarify what,
when and how the suspect of deafness was established.• Evaluate speech and the ability to read; in the event of a delay request ENT and
Paediatric assessment.
In the clinical management of “glue ear”, or chronic otitis media exudative, consider:
• Otitis media and exudative otitis media can be linked to each other.• In the case of a speech delay, refer to a specialist.• In the absence of a delay in speech, observe for a couple of months before
referring.• Lack of improvement after 2 weeks, should lead to referral.• In the presence of auditory fluctuations, reviewing every 2 months.• In older children, spontaneous resolution is more likely.• Nasal drops, mucolytic and antibiotics should help.
Auditory assessment of a child can usually take place in a GP surgery using the Leeds Picture Discrimination Cards and whispered voice a metre away.
• 0–3 years: refer• 3–6 years: Leeds Picture Discrimination Cards• 6 years: whispered voice
2 Otology

25
If parents believe that a child has hearing problems, refer. Always refer a child with marked hearing loss even when this is possibly due to the presence of serous otitis media, or glue ear.
RED FLAGS
Speech delay
Marked hearing loss
Malformations
Chronic ear discharge
Adult Deafness
Usually, deafness in adulthood has a slow onset and evolution. It can be uni-/bilat-eral, affecting the understanding of speech, especially on the phone and in noisy environments.
Key anamnestic points
• Past medical history of ear surgery• Infantile exanthema• Head trauma• Severe systemic diseases that have required the use of ototoxic medications• History of occupational exposure to noise• Hobbies such as hunting, or music• Family history of deafness• Diabetes• Autoimmune disease
Hearing Tests
Rinne Test
The Rinne test is used to evaluate CHL. CHL occurs when there is a problem conducting the sound waves to the inner ear anywhere along the route through the outer ear, tympanic membrane, ossicular chain, up to the oval window (or fenstra vesibuli). CHL may occur in conjunction with SNHL or in isolation. The Rinne
Hearing Tests

26
test is performed by placing a 512 Hz diapason to the patient’s mastoid bone. A person with intact hearing should be able to hear the tuning fork by air after he can no longer hear the sound through the bone. If the person being examined is not able to hear the tuning fork when it is quickly repositioned near to the external acoustic meatus that means his bone conduction is greater than the air conduction. In turn, this indicates that there is some kind of problem that inhibits the move-ment of sound waves to the cochlea (i.e. there is a hearing loss). In the case of hearing loss of a sensorineural type, the ability to perceive the diapason via con-duction through bone is also diminished, therefore the conduction of sound through the air will still be more effective (Fig. 2.17).
+
–
>
<
–
<
False
Fig. 2.17 Rinne
2 Otology

27
Weber Test
The Weber test is used to detect either unilateral hearing loss of transmissive type or unilateral sensorineural hearing loss (SNHL). When undertaking the Weber test, the 512 Hz diapason is placed in the centre of the patient’s forehead. Patients with uni-lateral hearing loss (or predominantly unilateral) perceive the sound from the dis-eased side if suffering from conductive hearing loss, or from the healthy side – or less sick – if suffering from a perceptive hearing loss. In transmissive deafness, if deafness is bilateral and there is a difference in the threshold between the two ears, the sound will be lateralized in the worst ear; if deafness is symmetrical, to the cen-tre (Fig. 2.18).
Obstruction of the Auditory Canal
• Benign lesion/exostoses of the EAC• Earwax
Exostoses are common is scuba divers and swimmers in cold waters. Their man-agement requires ENT referral. Wax can be removed by means of ear drops, such as sodium bicarbonate 3%, 3–4 drops to be applied for 3–4 days and to be followed, if necessary, by ear syringing.
Ear Syringing
Ear Irrigation Procedure
It is important that a comprehensive history has been undertaken before performing ear irrigation to determine if there are any contraindications why it should not be performed.
SNHLCHLNeg
Fig. 2.18 Weber
Hearing Tests

28
Also an understanding of the basic anatomy of the ear is essential, so that the clinician examining the patient understands what constitutes normal and when there are devia-tions to this. Patients should be advised to use olive oil for at least 7 days, to soften the wax prior to irrigation. The procedure for ear irrigation should follow the NHS Modernisation Guidelines written by Harkin (2007) and is as follows.
• Explain the procedure to the patient, outlining risks associated with it such as dizziness, perforation, otitis externa. If the patient is happy to proceed, gain con-sent and document.
• Check whether the patient has had ear irrigation before.• Sit the patient in a chair appropriate for the procedure with the ear to be irrigated
facing you.• Inspect both ears with the otoscope.• Place the protective cape and disposable towel in position, and ask the patient to
hold the receiver under the ear. It is advisable the patient tilt their head slightly towards the affected side.
• Check your head light or mobile light is in place.• Check the temperature of the water using a thermometer to approximately 37 °C.• Remember any variation by more than a few degrees may cause the patient to
feel dizzy. If this occurs, stop irrigating, and ask the patient to fix his gaze on some object for a few minutes until the dizziness passes.
• You should be sitting at the same level as the patient when carrying out this procedure.
Use of an electronic syringe (Propulse II irrigator)
• Fill the reservoir of the Propulse II irrigator with warm water of 37 °C. Set the pressure to minimum.
• Connect disposable jet tip applicator to the tubing of machine with firm push/twist action. Push until click is felt.
• Direct the tip of the jet into the reservoir and switch on the machine for 10–20 s. This distributes the water through the system to expel any trapped air or cold water. This also enables the patient to accept the noise the machine makes.
• Gently pull the pinna upwards and outwards to straighten the meatus.• Place the tip of the nozzle into the external auditory meatus entrance. Nothing
should be inserted into the ear further than the part that can be seen from the outside. Inform the patient that you are about to begin and that they should make you aware of any symptoms of pain, dizziness or nausea. Switch the machine on (using either foot or hand control).
• Direct the stream of water onto the posterior wall of the canal (11 o’clock in the right ear and 1 o’clock in the left ear). Increase the pressure switch as determined by the aural condition. It is advisable that a maximum of two reservoirs of water be used in any one irrigation procedure.
2 Otology

29
• If the clinician has not managed to remove the wax within 5 min of irrigation, switch to the other ear if indicated; allow approximately 15 min before returning to first ear.
• Periodically inspect the meatus with the otoscope and inspect the solution run-ning into the receiver.
• After removal of the wax, ask the patient to dry mop the excess water from the meatus. Dry mop excess water from meatus under direct vision because stagna-tion of water and any abrasion of the skin during the procedure may predispose the otitis externa to infection.
• Examine ear, both meatus and tympanic membrane, and refer to ENT if there is severe inflammation or trauma. Record all findings and treatment in the patients’ notes.
NB: Irrigation should never cause pain. If the patient complains of pain – stop immediately.
Contraindications
Irrigation should not be carried out when the patient:
• Has a history of a perforation or there is a history of mucous discharge in the last year
• Has had a history of middle ear infection in the last 6 weeks• Has had an untoward experience following this procedure in the past• Has had previous ear surgery• Has a grommet in place• Has evidence of otitis externa• The patient has a cleft palate (repaired or not)• Has epilepsy
Precautions
• Tinnitus – people with troublesome tinnitus may notice that when the wax is removed and their hearing improves the tinnitus may increase in severity; dis-cuss the procedure with the patient in detail and document consent in patients’ records
• Healed perforation – discuss on an individual basis – consider referral for suction removal
• Dizziness
Hearing Tests

30
Evaluation of Auditory Function by GP
• Whispered voice at 1 metre with contra lateral masking• Conversation at 1 metre with contra lateral compression of tragus• General conversation with lip masking• Test with the diapason: Weber and Rinne with 512 Hz tuning fork• Pure tone audiometry if available
RED FLAGS
Unilateral hearing loss
Sudden hearing loss
Deficits of cranial nerves
Services for Patients with Hearing Loss
• ENT departments• Audiologists• Special schools• Adapted television and telephone
Key PointsConsider referral if:
• Removing the earwax doesn’t solve the deafness• Sudden onset of deafness in the absence of earwax• Unilateral symptoms• Other symptoms in addition to ear tinnitus• Tympanic membrane abnormalities
2 Otology

31
Vestibular System
The use of Frenzel goggles may be particularly helpful to look and assess for the presence of nystagmus. This may be spontaneous, gaze evoked, post-headshake, positional, triggered by the Dix-Hallpike manoeuvre, by pneumatic otoscopy, or by other techniques. Smooth pursuit, saccades, gait, and head-shaking nystagmus should be assessed. The Romberg test, the Fukuda step test and the hyperventilation test are also helpful.
Smooth Pursuit
Smooth pursuit is a movement of the eyes allowing us to follow a moving target. We can also shift the gaze voluntarily by means of saccadic eye movements. Pursuit is triggered by a moving visual signal and it would be very difficult, if possible, to be initiated in its absence. Smooth pursuit and saccades work together. If a target moves faster than 30°/s, the pursuit tends to require catch-up saccades. Smooth pursuit is asymmetric in so far that we are better at horizontal than vertical smooth pursuit, that is we can follow a moving target without making catch-up saccades horizontally rather than vertically. We are also better at downward rather than upward pursuit. Smooth pursuit may be affected by a variety of conditions as it requires the coordination of different brain areas also far away from each other.
Saccades
As briefly mentioned above, a saccade is quick, coordinated movement of both eyes between two positions of fixation in the same direction. Saccades are involved in fixation, rapid eye movement, and in the fast phase of optokinetic nystagmus.
Head-Shaking Nystagmus
Head-shaking nystagmus, or HSN, is a latent spontaneous vestibular nystagmus which can be provoked by rapid passive head shaking around a vertical axis. Typically HSN is triggered by means of horizontal sinusoidal head oscillations of 30° each side, for at least 20 cycles, and then abruptly interrupted. Ideally, the head of the subject should be 20° downward with respect to the vertical axis, so that the
Vestibular System

32
axis of rotation could be parallel to one of the semicircular lateral canals. HSN is absent in normal subjects; hence its identification with Frenzel’s glasses in a dark room or a video camera (videonystagmoscopy) can be helpful. In fact, passive head shaking is an effective way of triggering nystagmus in patients with peripheral and central vestibular lesions.
Fukuda Stepping Test
The Fukuda stepping test (FST) is another particularly useful test in the limited space of a consulting room. In the FST, also known as Unterberger’s stepping test, the patient is asked to walk in place with their eyes closed. There are two variants to the test, with 50 and 100 steps, the latter being somewhat more sensitive. Abnormal deviation towards the side of the lesion, that means >45° deviation, occurs in most cases, but in about 1/4 of the patients this could be towards the intact side, and in another 1/4 it can remain within the normal range. Hence, if the patient rotates to a particular side they may have a labyrinthine lesion on that side, but this test should not be used in isolation of other tests to diagnose lesions.
Hallpike Test
Also known as the Dix-Hallpike test, it is probably one of the most helpful test that can be performed in primary care to make diagnosis of BPPV. The British Society of Audiology (2014) suggests the clinician should begin by explaining the procedure to the patient and demonstrating if necessary. Make sure the patient is aware that he/she may experience vertigo with eventual nausea and/or vomiting, but that this is likely to be short-lived. Also, the clinician should be aware of the absolute contraindica-tions to the test; these are: recent cervical spine fracture, atlanto-axial subluxation, cervical discopathy, confirmed vertebro-basilar insufficiency and recent neck trauma that restricts torsional movements of the neck. The test is performed with the patient sitting upright on the examination table, or on their bed during a home visit, with the legs extended. The patient’s head is then rotated to one side by 45°. The examiner helps the patient to lie down backwards quickly with the head held in 20° extension. This extension may either be achieved by having the examiner supporting the head as it hangs off the table/bed, or by placing a pillow under their upper back. The patient must be reminded to keep the eyes open staring straight ahead, and endeav-ouring to suppress blinks, as their eyes are then observed for about 45 s. There is a characteristic 5–10 s period of latency prior to the onset of nystagmus. If rotational nystagmus occurs then the test is considered positive for benign positional vertigo. During a positive test, the fast phase of the rotatory nystagmus is towards the affected ear, which is the ear closer to the ground. The direction of the fast phase is defined by the rotation of the top of the eye, either clockwise or counter-clockwise.
2 Otology

33
Tinnitus
Tinnitus is the hearing of sound when no external sound is present. It can be described in various ways, but most often as a whistle or hum, in the head; in some cases, the noise is described as pulsating and synchronized with the heartbeat.
Subjective Tinnitus
It is more often associated with a sensory deficit. A disease of the middle ear that inhib-its masking ambient sounds, such as an otitis media, can exacerbate it. Many adults are extremely anxious about tinnitus. Often the patient fears a brain tumour causes tinnitus. A reduction of the anxiety levels may be surely beneficial. When this is present, the patient will probably be willing to have an MRI scan, but rather rarely this would bring any valuable information. Many patients are aware of a certain level of deafness.
• Refer to a specialist if deafness has a social impact• Refer if the tinnitus is unilateral• If mild, reassure the patient about the benign nature of tinnitus
Objective Tinnitus
Objective tinnitus occurs when the examiner can hear it as well. Objective tinnitus is rare and it demands further investigations via ENT referral.
Vertigo
The patient uses various terms to describe dizziness such as unsteadiness, light- headedness, giddiness or vertigo. It is up to the clinician to determine if it is an episode of true vertigo or not. Vertigo is a sensation of spinning and as such, to make a diagnosis of vertigo, the patient needs to have experienced a rotational movement
Key Points• Good lighting• Practice your technique• Correct equipment• Be methodical
Tinnitus
34
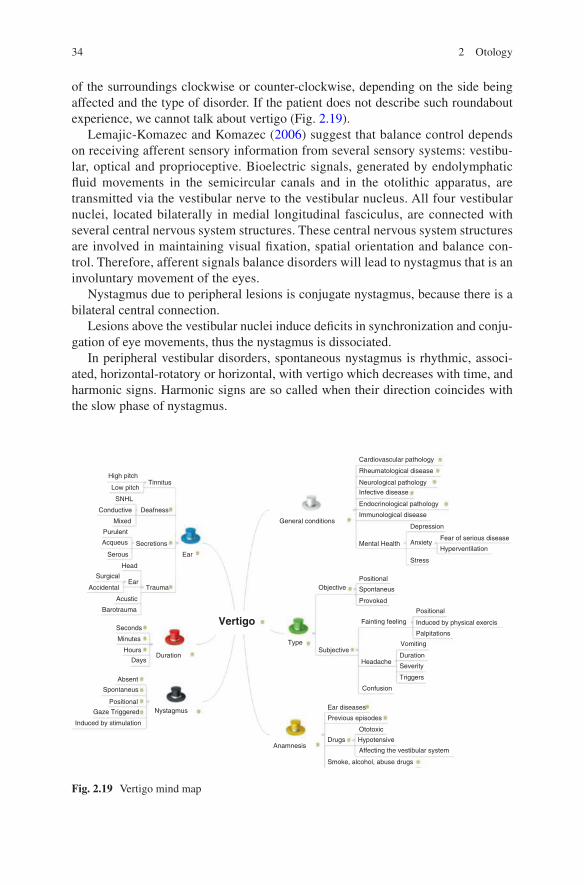
of the surroundings clockwise or counter-clockwise, depending on the side being affected and the type of disorder. If the patient does not describe such roundabout experience, we cannot talk about vertigo (Fig. 2.19).
Lemajic-Komazec and Komazec (2006) suggest that balance control depends on receiving afferent sensory information from several sensory systems: vestibu-lar, optical and proprioceptive. Bioelectric signals, generated by endolymphatic fluid movements in the semicircular canals and in the otolithic apparatus, are transmitted via the vestibular nerve to the vestibular nucleus. All four vestibular nuclei, located bilaterally in medial longitudinal fasciculus, are connected with several central nervous system structures. These central nervous system structures are involved in maintaining visual fixation, spatial orientation and balance con-trol. Therefore, afferent signals balance disorders will lead to nystagmus that is an involuntary movement of the eyes.
Nystagmus due to peripheral lesions is conjugate nystagmus, because there is a bilateral central connection.
Lesions above the vestibular nuclei induce deficits in synchronization and conju-gation of eye movements, thus the nystagmus is dissociated.
In peripheral vestibular disorders, spontaneous nystagmus is rhythmic, associ-ated, horizontal-rotatory or horizontal, with vertigo which decreases with time, and harmonic signs. Harmonic signs are so called when their direction coincides with the slow phase of nystagmus.
High pitchTinnitus
General conditions
Objective
Type
Positional
Spontaneus
Provoked
Fainting feeling
Headache
Confusion
Ear diseases
Previous episodes
Ototoxic
Drugs HypotensiveAnamnesis
Affecting the vestibular system
Smoke, alcohol, abuse drugs
Positional
Induced by physical exercis
Palpitations
Vomiting
Duration
Severity
Triggers
Subjective
Deafness
Secretions
Trauma
Ear
Low pitch
SNHL
Conductive
Mixed
Purulent
Acqueus
Serous
Head
SurgicalEar
Accidental
Acustic
Barotrauma
Seconds
Minutes
Hours
Days
Absent
Spontaneus
Positional
Gaze Triggered
Induced by stimulation
Nystagmus
Duration
Vertigo
Mental Health Anxiety
Stress
Depression
Hyperventilation
Fear of serious disease
Immunological disease
Endocrinological pathology
Infective disease
Neurological pathology
Cardiovascular pathology
Rheumatological disease
Fig. 2.19 Vertigo mind map
2 Otology

35
Spontaneous nystagmus in central vestibular lesions is severe, dissociated, hori-zontal, rotatory or vertical, without changes related to optical suppression; if ves-tibular symptoms are present, they are non-harmonic.
In central disorders, findings after peripheral, caloric stimulation – which can be carried out by a clinical audiologist – are either normal or pathological, with dysrhythmias and inhibition in pendular stimulation (Fig. 2.20).
Jerk nystagmusconvergence-retraction nystagmusrefers to the irregularjerking of the eyes backinto the orbit during up-ward gaze. It can indicatemidbrain tegmental dam-age.
Pendular nystagmusHorizontal, or pendu-lar, nystagmus refers to oscillations of equal ve-locity around a centerpoint. It can indicate con-gential loss of visual acu-ity or multiple sclerosis.
Downbeat nystagmusrefers to the irregulardownward jerking of theeyes during downwardgaze. It can signal lowermedullary damage.
Vestibular nystagmus,the horizontal or rotarymovement of the eyes,suggests vestibular dis-case or cochlear dysfunc-tion.
Vertical, or seesaw,nystagmus is the rapid,seesaw movement of theeyes; on eye appears torise while the other ap-pears to fall. It suggestsan optic chiasm lesion.
Fig. 2.20 Jerk vs. pendular nystagmus
Vertigo
36
Objective Vertigo
Ménière’s Syndrome
This is probably diagnosed more often than it should be. It is an idiopathic disease of the inner ear characterized by hearing loss, tinnitus and dizziness. Endolymphatic hydrops, that is an increase of the inner ear fluids pressure, mostly sharp, is believed to be responsible for the onset of the symptoms and signs.
Clinical Presentation• Vertigo and nausea• Hearing fluctuation with vertigo• Feeling of ear fullness, or pressure• Tinnitus• Cluster episodes, of variable duration ranging from several hours to days
Ménière’s syndrome must be referred to a specialist for an appropriate diagnostic and therapeutic management.
Clinical Management• Medical: diuretics, hypo-saline diet, sedatives, anti-vertiginous, antiemetic, any
correction of metabolic dysfunctions and vasculopathy.• Surgery: surgical therapy is indicated in those cases that do not benefit from
medical treatment. It can be divided into conservative and destructive: the latter should be reserved for the terminal stages of the disease and unilateral forms. The conservative treatment or functional treatment aims for the improvement of the vestibular symptoms with hearing preservation: sacculotomy and endolym-phatic shunt. The most radical intervention does not take into account the conse-quences for the hearing, in an attempt to achieve the highest success rate: it consists of the labyrinthectomy and in the section of the vestibular nerve.
Viral Labyrinthitis
It is characterized by the presence of:
• Recent viral upper respiratory tract infection• Accompanied by nausea and vomiting• Often lack of hearing impairment• Normal otoscopic examination• Beginning as vertigo then later changes into imbalance and resolves
Clinical Management• Reassure the patient that symptoms generally resolve within a few days, some-
times weeks, occasionally months• Use of vestibular suppressant if necessary• Vestibular physiotherapy• Refer to a specialist if symptoms persist for more than 6 weeks
2 Otology

37
Subjective Vertigo
Vertebrobasilar Insufficiency
The diagnosis is suggested by:
• Association with the neck extension and rotation• Normal tympanic membrane• Association with cervical pain from spondylosis• May be associated with other diseases due to atherosclerosis• Occasional episodes of cerebral ischemia
Clinical Management• Cervical collar – rarely proposed nowadays• Lifestyle changes• Treatment of osteoarthritis
Fistula Test
In the case of a cholesteatoma with or without otorrhoea, you might encounter an erosion of lateral semi-circular canal. In the case of cholesteatoma and vertigo, fis-tula test can sometimes confirm the diagnosis. To perform the fistula test, you are squeezing the tragus with the finger, and the patient, in case of a positive test, expe-riences the presence of objective vertigo with nystagmus directed towards the oppo-site side. Alternatively, you can use the pneumatic otoscope to achieve the same objective.
Key PointsRefer urgently to specialist in case of:
• Cholesteatoma• Otorrhoea• Deafness• Facial paralysis• Headaches and other neurological abnormalities• Previous otological surgery• Recent head injury
Vertigo

38
Benign Paroxysmal Positional Vertigo (BPPV)
Patients suffering with BPPV experience short bursts of severe dizziness when they move their head in certain directions.
Clinical Presentation• Vertigo generally appears when the patient gets up from bed, or lies down; when
looking up to a shelf, or lacing shoes.• Typically one side is affected and the patient learns to avoid this position, most
notably the recumbent on one side when in bed.• Can be cured with appropriate clinical examination.• Otoscopy is normal.
Clinical Management• Reassure the patient• Vestibular exercises (Fig. 2.21)• Refer to a specialist if it does not resolve within 1 month
References
British Society of Audiology (2014) Recommended procedure for hallpike maneuver [online]. http://www.thebsa.org.uk/wp-content/uploads/2014/04/HM.pdf
Hain TC (1997) Approach to the Vertigo. In: Practical neurology. Lippincott-Raven, PhiladelphiaHarkin H (2007) Ear care guidance from the NHS Modernisation Agency. NHS Modernisation,
LondonLemajic-Komazec S, Komazec Z (2006) Initial evaluation of vertigo. Med Pregl 59(11–12):
585–590
2 1 43
Fig. 2.21 Vestibular exercises for BPPV
2 Otology

39© Springer International Publishing AG 2017 E. Cervoni, K. Leech, ENT in Primary Care, DOI 10.1007/978-3-319-51987-6_3
Chapter 3Rhinology
The Nose
Undertaking a history of the nose should include questions aiming to establish whether any of its functions – smelling, conditioning, warming, humidification of inhaled air and voice resonance – is impaired or not. Change of airway resistance and sense of smell are key indicators of nasal pathology. Also common presenta-tions seen in primary care are rhinorrhoea, epistaxis, facial pain or sense of pressure, and a nasal voice. Rhinorrhoea is perhaps the most frequent sign reported and observed by the clinician when dealing with nasal problems. Like otorrhoea, the clinician should ascertain whether the discharge is watery, purulent, mucousy or blood stained as this will help determine the cause. Rhinorrhoea can be chronic, acute or recurrent; so gaining an understanding of the duration may be pertinent. The patient should be asked if it is linked to any allergies or whether it is seasonal. Associated symptoms that the patient may describe include watering eyes, itchy eyes, sore throat and facial pain or pressure.
Many patients complain of nasal obstruction. This can be unilateral or bilateral. The clinician should determine the duration it has been occurring for, whether it is constant, intermittent or related to seasons or allergies. Any associated symptoms should also be explored including facial pain, sneezing, headache, post-nasal drip, sore throat, otalgia and asthma. If a patient presents with epistaxis, the clinician must prioritise significant bleeding over undertaking a history. However, once the bleeding is controlled, then the clinician should enquire as to whether the epistaxis was unilateral or bilateral, anterior or posterior. Foreign bodies can lead to epistaxis and should be ruled out, especially in children. It is important to ask the patient if the bleed was spontaneous or post trauma. The onset, duration and recurrence are also of significance.
Associated symptoms should be reviewed along with medications prescribed and past medical history. For example, the patient may be prescribed anti- coagulants or suffer from hypertension or renal disease. Symptoms that may direct the clinician to

40
suspect sinusitis include pressure or pain in the patient’s cheeks or forehead, nasal congestion, a sense of heaviness in the head heaviness and sometimes facial pain.
Determining the severity of the pain and the length of time a patient has experi-enced the symptoms will establish appropriate management. If the sinusitis has lasted up to 10 days it is likely to be viral. For symptoms lasting longer than 10 days it is more likely to be a bacterial sinusitis. Symptoms lasting for more than 12 weeks are suggestive of chronic sinusitis, and lasted >12 weeks is chronic sinusitis. Patients may describe fever, purulent discharge, nasal obstruction, post-nasal drip, chronic unproductive cough, malaise and facial pain.
Nasal voice may be distinguished in hyponasal and hypernasal speech, otherwise respectively known as rhinolalia clausa and rhinolalia aperta. The first is typical of nasal congestion, the latter of cleft palate and velopharyngeal insufficiency. The doc-tor should be informed about the presence of defects of smell, such as loss of smell (anosmia), its reduction (hyposmia), and unpleasant odours, particularly putrefactive odours (cacosmia). A thorough patient history is essential in determining any olfac-tory disorders such as sense of smell and sense of taste can often be confused by patients. Patients may also present with hyposmia, which is partial loss of smell. The clinician should ascertain the time the loss occurred and if there were any other con-tributing factors, such as trauma or illness. Intra-nasal obstruction, allergic rhinitis, head trauma and also type II diabetes and Alzheimer’s have been linked to anosmia. Drug and alcohol history should be taken as long term alcohol misuse can lead to anosmia. Certain medications such as metronidazole can also cause it (Fig. 3.1).
Nose Assessment
An otoscope can be used to make a rhinoscope with a wide speculum. The patient should be asked to breathe with his mouth during the examination to prevent the otoscope lens fogging during the procedure. The otoscope gives a good view of the anterior nasal cavity (Fig. 3.2).
Degree
Duration Fever
Pain
Nose
Hyposmia
Anosmia
Change of taste
Facial
Headache
Laterality
Unilateral
Bilateral
Serous
Aqueous
Purulent
Blood stained
Type
Triggers
Duration
Laterality
Nasal discharge
Olfaction changes
Nasal obstructionLaterality
Duration
Onset
Hyponasal
Hypernasal
Change of voiceresonance
Trauma
Epistaxis
Surgical
Accidental
Laterality
Amount
Duration
Drugs
Frequency
General conditions
NSAIDs
Triggers
Anticoagulants
Fig. 3.1 Rhinological anamnesis mind map
3 Rhinology
41
Dentist Mirror or a Cosmetic Mirror
Useful to evaluate the nasal flow, particularly in newborns.
Silver Nitrate Sticks
Silver nitrate sticks can be used for nasal cauterization to treat recurring nose bleeds. Frequent nose bleeds are likely to be a result of an exposed blood vessel in the nasal cavity; therefore cauterizing it may prevent further bleeding. Silver nitrate sticks look like large matches and are dipped in water before being applied to the lesion for a few seconds (Fig. 3.3).
Fig. 3.2 Otoscope being used to perform nasal examination
Fig. 3.3 Silver nitrate sticks
Nose Assessment
42
Nose Inspection
• Symmetry• Septal deviations• Deformity of the nasal pyramid• Patency of the nostrils• Little’s area (varices, crusting, bleeding) (Figs. 3.4 and 3.5).• Septal perforations• Nasal vestibule• Turbinates• Osteo-meatal complex• Injury or growths in the nasal cavity
Epistaxis
Patients do often experience recurring spontaneous nasal bleeding, from one or both nostrils. Sometimes, the GP is called to deal with epistaxis at the surgery, but much more frequently this pathology is handled in the Emergency Room.
Epistaxis in the Child
Children tend to bleed from the nose more easily than adults and from the front of the septum, otherwise known as Little or Valsalva area. Establishing the severity of bleeding should take precedence over the history taking.
Fig. 3.4 Little’s area, otherwise known as Valsalva area
3 Rhinology
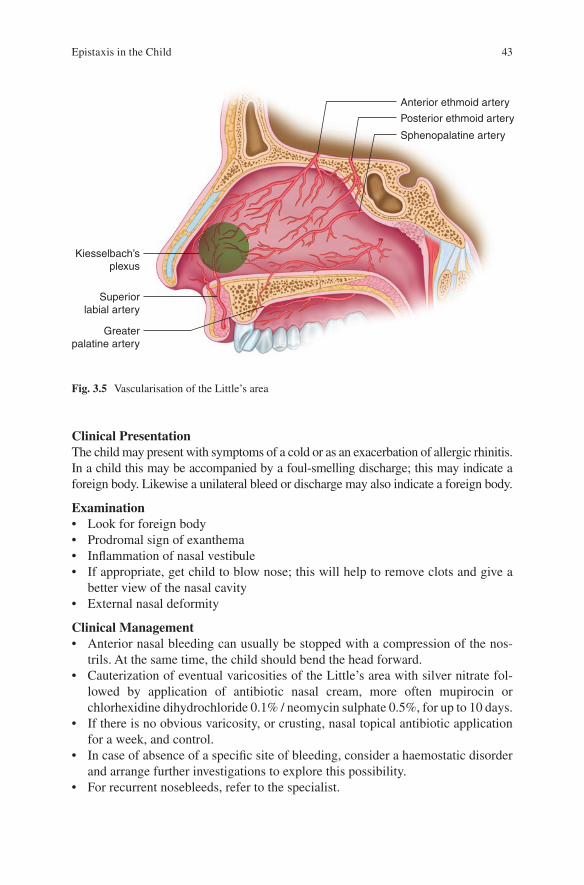
43
Clinical PresentationThe child may present with symptoms of a cold or as an exacerbation of allergic rhinitis. In a child this may be accompanied by a foul-smelling discharge; this may indicate a foreign body. Likewise a unilateral bleed or discharge may also indicate a foreign body.
Examination• Look for foreign body• Prodromal sign of exanthema• Inflammation of nasal vestibule• If appropriate, get child to blow nose; this will help to remove clots and give a
better view of the nasal cavity• External nasal deformity
Clinical Management• Anterior nasal bleeding can usually be stopped with a compression of the nos-
trils. At the same time, the child should bend the head forward.• Cauterization of eventual varicosities of the Little’s area with silver nitrate fol-
lowed by application of antibiotic nasal cream, more often mupirocin or chlorhexidine dihydrochloride 0.1% / neomycin sulphate 0.5%, for up to 10 days.
• If there is no obvious varicosity, or crusting, nasal topical antibiotic application for a week, and control.
• In case of absence of a specific site of bleeding, consider a haemostatic disorder and arrange further investigations to explore this possibility.
• For recurrent nosebleeds, refer to the specialist.
Anterior ethmoid artery
Kiesselbach’splexus
Superiorlabial artery
Greaterpalatine artery
Posterior ethmoid artery
Sphenopalatine artery
Fig. 3.5 Vascularisation of the Little’s area
Epistaxis in the Child

44
RED FLAGS
Bleeding non resolving with direct pressure
Recurrent idiopathic epistaxis
Signs of shock
Epistaxis in Adults
Clinical PresentationLike children, establishing the severity of the bleed should take precedence over the history taking. Once this has occurred it is important to establish whether the epi-staxis is unilateral or bilateral. A good history should enquire about previous epi-staxis, history of hypertension, other systemic diseases, family history or any bruising. In adults, a medication review may prove helpful looking for anti- coagulants, aspirin, NSAIDs and dipyridamole.
Examination• Consider anterior nasal bleeding as in children. Approximately 90% of bleeds
are anterior in nature.• Posterior nasal bleeding should be suspected when a specific point of bleeding is
not clearly identifiable, or stopped with the compression of the nostrils.
Posterior epistaxis is:
• More frequent in old age• More severe when associated with hypertension• May stop spontaneously, but is usually very copious• Should be handled within the scope of first aid emergency ENT
Clinical Management• Treat the anterior nasal bleeding as in children• In case of posterior nasal bleeding
– Check blood pressure – Refer to a specialist if recurring, or if associated with visible nasal lesion
Key PointsCheck if the patient takes anticoagulants.
Check haematocrit and coagulation.Consider angiofibroma in a young man with nasal obstruction. In this case,
refer to the specialist.
3 Rhinology
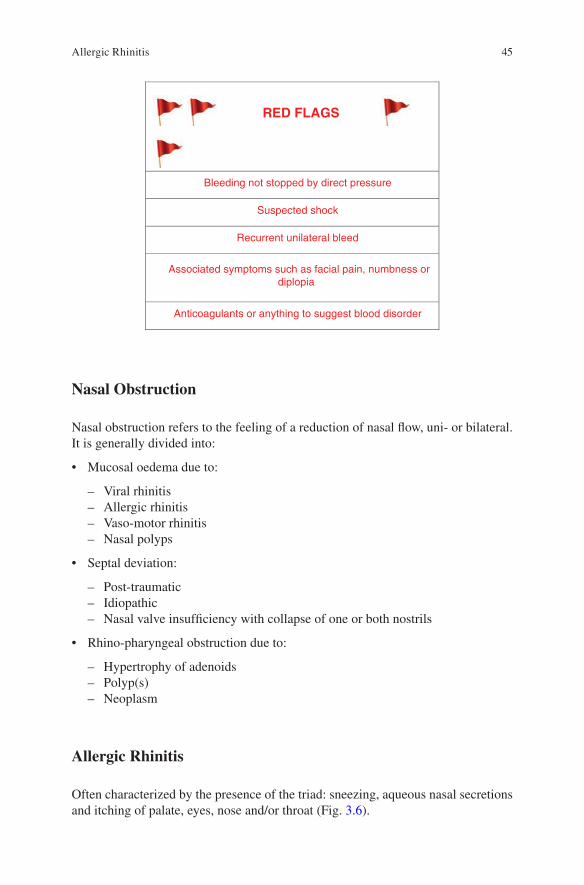
45
RED FLAGS
Bleeding not stopped by direct pressure
Suspected shock
Recurrent unilateral bleed
Associated symptoms such as facial pain, numbness ordiplopia
Anticoagulants or anything to suggest blood disorder
Nasal Obstruction
Nasal obstruction refers to the feeling of a reduction of nasal flow, uni- or bilateral. It is generally divided into:
• Mucosal oedema due to:
– Viral rhinitis – Allergic rhinitis – Vaso-motor rhinitis – Nasal polyps
• Septal deviation:
– Post-traumatic – Idiopathic – Nasal valve insufficiency with collapse of one or both nostrils
• Rhino-pharyngeal obstruction due to:
– Hypertrophy of adenoids – Polyp(s) – Neoplasm
Allergic Rhinitis
Often characterized by the presence of the triad: sneezing, aqueous nasal secretions and itching of palate, eyes, nose and/or throat (Fig. 3.6).
Allergic Rhinitis

46
Clinical PresentationWhen taking the medical history, you should also look for data that can identify the potential allergen(s) such as:
• Dust• Pollens• Feathers• Mould• Spore• Animal dander
ExaminationTypical findings at the clinical examination are:
• Oedema of the inferior turbinate• Pale colour of the nasal mucosa• Wet nasal mucosa• Choanal space reduction• Allergic dermatitis
Clinical Management• Medicinal products for topical use.• Steroids for nasal use. They are also available in aqueous forms that cause less
easily nasal bleeding.• Allergen(s) avoidance.• Anticholinergics for topical use if the rhinorrhoea is predominantly watery.• In the case of cacosmia and facial pain, a study of the paranasal sinuses is essen-
tial before starting the steroid use.
Fig. 3.6 Swollen inferior turbinate in allergic rhinitis
3 Rhinology
47
• Oral therapy supports topical treatment. In case of nasal symptoms or persistence of non-nasal symptoms, their use is particularly recommended and relies on:
– Anti-histamine – Pseudo-ephedrine – Anti-histamine and sympathomimetics
• Inhalation therapy. Perhaps not as popular in the UK as it may be in the rest of Europe, it is based on the use of:
– Menthol – Steam – Eucalyptol
– Inhalations reduce pain in sinuses and reduce nasal obstruction most often, up to 2 h.
• Immunotherapy – This is still not widely available. Fujisawa (2015) suggests that to make the therapy more effective, it is preferable to start it as early as possible, hopefully in infancy. But it is still difficult at present because of relatively fre-quent adverse events and invasive manner of administering allergen extracts for young children. It would need a referral to an allergologist.
• Surgery – Surgical interventions aim to reduce the volume of the turbinate which is recommended when:
– Nasal obstruction is severe. – Medical treatment does not give good results. – Turbinate reduction improves airflow and the distribution of medicines for
topical use.
Vasomotor Rhinitis (Fig. 3.7)
Clinical PresentationVasomotor rhinitis in many ways resembles allergic rhinitis, but it is not triggered by an allergen and its cause is currently unknown. It can be exacerbated by:
• Perfumes• Spray• Air temperature changes• Tobacco smoke or other irritants
In addition:
• There is not usually an associated itch• The obstructed side is generally alternating• Can co-exist with an allergic form• Sometimes it is associated with puberty and hormonal changes• Its onset may be associated with anxiety and frustration• Watery nasal discharge is typical
Vasomotor Rhinitis

48
Examination• Vasomotor rhinitis can be sub-classed as ‘runners’ that exhibit wet rhinorrhea• Dry vasomotor rhinitis – with airflow resistance and nasal obstruction with lim-
ited rhinorrhea
Clinical ManagementClinical management mirrors that of allergic rhinitis. The distinction between aller-gic rhinitis and vasomotor rhinitis may be clinically challenging and it is most often dictated by history data rather than by the appearance of the nasal mucosa.
Nasal Polyps (Fig. 3.8)
Clinical PresentationSymptoms develop in a gradual, progressive way and are very often in the context of an allergic rhinitis or vasomotor rhinitis. In addition, there is often a history of:
• Previous nasal polypectomy• Decreased sense of smell• Recurrent sinusitis
Examination• Alterations in facial appearance• Assess inferior turbinate, anterior septum and middle meatus• Assess posterior wall for polyposis• Undertake otoscopy – extensive polyposis can lead to Eustachian tube dysfunc-
tion and cause otitis media
Clinical Management• In the case of mild symptoms, intra-nasal drops such as Beclomethasone should
be applied twice daily with the head in extended position.
Fig. 3.7 Vasomotor rhinitis with watery discharge
3 Rhinology

49
• Alternatively, you can use a steroid spray.• An x-ray of the sinuses may be useful to detect possible hydro-air levels, but it is
nowadays rarely requested as CT and MRI scan are easily available and do offer significant diagnostic advantages.
• An oedema or thickening of the mucosa of the paranasal sinuses is acceptable, if minimal.
• We recommend smoking cessation.• ENT specialist advice should be sought when:
– Drug therapy does not produce acceptable results – Severe nasal obstruction – A neoplastic pathology is suspected due to the presence of unilateral polyp,
with or without nasal bleeding
0 1 3 42
MT MT MTMT MT
IT IT ITIT IT
Fig. 3.8 Nasal polyposis and its grading (Lund and Mackay 1993)
Key PointsIn the case of nasal polyps, one must always keep in mind that this is a recur-rent disease, so the topical steroid therapy should be maintained.
RED FLAGS
Bloody discharge
Unilateral growth
Facial swelling
Polyps in children could mean cystic fibrosis
Nasal Polyps

50
Allergy Testing
The allergy testing can be made via cutaneous stimulation, the patch and the prick test, or via blood collection using the RAST test. The latter can be directly arranged by GPs. The skin tests require the support of a Resuscitation Department and the patient should stay in observation for a couple of hours. A referral should be arranged, but the purpose of skin tests is limited and often impractical. Even from a commercial point of view, the advantages are much reduced, and because of this it is not easy to find the necessary kit. The RAST test (radio absorbent sensitivity test) is easily obtainable, although expensive; it can be carried out on a sample of venous blood.
Septal Deviation
Examination• May be associated with deformity of the nasal pyramid.• There may be a history of trauma of the nasal pyramid.• Unilateral nasal obstruction is often present.• There are often coexisting changes of the nasal mucosa, such as compensatory
hypertrophy of the turbinates.
Clinical Management• Refer to a specialist if nasal obstruction is only due to septal deviation.• In case of co-existence of rhinitis, treat the rhinitis first, and if that’s not enough,
refer to a specialist.
Inspiratory Nasal Valve Collapse
A certain degree of movement of the nostrils during inhalation is normal. However, a collapse of the nostril(s) is pathological and leading to nasal obstruction. In this case, the patient should be referred to an ENT specialist (Fig. 3.9).
Nasopharyngeal Obstruction
The causes of nasopharyngeal obstruction include:
• Hypertrophic adenoids in children (Fig. 3.10)• Antro-coanal polyps• Craniosynostosis
3 Rhinology

51
• Post-surgical scarring• Tumours
Examination• Look for dysmorphic features• Perform anterior rhinoscopy• Assess oropharynx• Both in adults and in children look for possible ear pathology• Cervical lymph nodes: palpate for any inflammatory or neoplastic pathology
Clinical Management• This highly depends on the cause of the obstruction. Referral to the ENT special-
ist is required and if the adenoids are deemed to be responsible for the obstruc-tion, they may require adenoidectomy.
Fig. 3.9 Collapse of the nasal valve
Fig. 3.10 Adenoids hypertrophy
Sinusitis

52
Sinusitis
Sinusitis it is common presentation in primary care (Fig. 3.11).
Clinical PresentationThe following symptoms suggest the possibility of sinusitis:
• Cacosmia• Facial pain and tenderness of the maxillary and frontal sinuses• Nasal obstruction• Mucopurulent rhinorrhoea• Fever associated with symptoms listed above, peri-orbital oedema or swelling of
face (or Pott’s oedema) can occur as a complication of sinusitis but it is unusual with proper medical treatment
• Sensation of congestion of upper respiratory tract, head, and ears• Dizziness• Hyposmia
Examination• Rhinoscopy to ascertain the presence of nasal discharge• Assess for fever• Facial tenderness
Clinical Management• In the event of Pott’s oedema, refer immediately to the ENT specialist• Antibiotic therapy may be indicated if sinusitis does not respond to home reme-
dies or symptoms are severe• Analgesia
Fig. 3.11 Purulent sinusitis
3 Rhinology

53
• Menthol/inhalations• Refer to the specialist in case of non-resolution of symptoms
Recurring Rhinosinusitis
Examination• A minimum mucosal thickening without hydro-air levels is common and not
necessarily pathological, and a diagnosis of rhinitis, rather than of sinusitis, should be taken into account.
• Bone erosions are suggestive of neoplastic disease and require urgent specialist clinical evaluation.
• Small cystic lesions of maxillary sinuses are common and do not require treatment.
Clinical Management• Imaging may help to assess the presence of chronic disease. GP may request
x-rays with chin-occipital view to evaluate the maxillary, frontal and ethmoid sinuses.
• An acute exacerbation of a recurring form requires the use of metronidazole and penicillin, or macrolide.
• Analgesia.• Menthol/inhalations.• In an allergic rhinitis, nasal steroid are useful.• Nasal polyposis can respond to the nasal steroid spray or drops.• Referring to a specialist is required in case of:• Frequent recurrences• Large nasal polyps• Large septal deviation• Suspect of neoplastic pathology
In the absence of radiographic abnormalities, diagnosis of sinusitis is highly unlikely. The clinician should consider other possible causes of facial pain and in particular the contact between nasal concha and septum.
Key PointsRhinitis medicamentosa is a disease that results from prolonged use of decon-gestants. If a patient presents with nasal obstruction and nasal mucosa oedema after a period of prolonged use of decongestants, refer to a specialist as may require surgical correction.
Unilateral nasal secretion in a child is believed to be due to the presence of a foreign body until proven otherwise and it requires an urgent ENT referral.
Children are not prone to nasal polyps and their presence should trigger the suspect of cystic fibrosis.
Sinusitis

54
References
Fujisawa T (2015) Allergen immunotherapy in children. Arerugi 64:787–794Lund VJ, Mackay IS (1993) Staging in rhinosinusitus. Rhinology. 31:183–184
Patients from tropical regions, or sub-tropical, may take a couple of years before showing signs of dust allergy.
Nasal polyps should always trigger an ENT referral if unilateral.Steroid drops should be avoided in the long term in favour of spray.Remember nasal valve incompetence as a cause of nasal obstruction.Posterior nasal drainage is a nonspecific symptom.Facial oedema is always indicative of complications and the patient should
be referred to a specialist.Unilateral nasal bleeding with obstruction, or facial pain, should be sent to
a specialist with a suspect of neoplastic pathology.
3 Rhinology

55© Springer International Publishing AG 2017 E. Cervoni, K. Leech, ENT in Primary Care, DOI 10.1007/978-3-319-51987-6_4
Chapter 4Laryngology
The Throat
Voice problems and sore throat are two of the most common complaints associated with the throat, larynx and hypopharynx regions. Voice disorders should be distin-guished in problems with the articulation of the voice, or dysarthria, and hoarseness, or dysphonia, when there is a change in the quality of the voice instead.
Hoarseness is the most frequent among the two. It is important to determine if hoarseness has been of a gradual onset or sudden onset. Gradual onset may be as a result of smoking or drinking alcohol, whilst sudden onset may be as a result of an infection or vocal abuse. Smoking and alcohol should be documented in all cases. A patient’s occupation may provide vital information to the history, especially if they use their voice in a professional way such as a singer. In these cases it is worth ask-ing the patient if they have experienced a change in their pitch or abnormal pitch range. The clinician should determine if their hoarseness is constant, or whether it changes throughout the day. Any exposure to chemicals or corrosive substances may also be important. Previous trauma, surgery or endotracheal intubation should be ascertained. Patients may describe their voice disturbances as breathy, hoarse, low-pitched, strained, and trembling or a feeling of vocal fatigue. Clinicians should be aware that specific voice disturbances could help the focus on a differential diag-nosis. For example, breathy complaints could indicate functional dysphonia, vocal cord paralysis or abductor spasmodic dysphonia.
Dysarthria results from a neurological injury of the phonation system. As such, the causes may be several, including multiple sclerosis, Parkinson’s disease, Parkinson plus syndromes, stroke, motor neuron disease and others. A sore throat itself is actually a symptom. Other common presenting symptoms include a feeling of a lump in throat, mucus in the throat and general discomfort. Sore throat is usu-ally caused by viral infection; however, the most common bacterial infection affect-ing the throat is Group A beta-haemolytic streptococcus. The clinician should ascertain the duration and severity of the symptoms, any dysphagia, rash or stridor,

56
whether the patient feels systemically unwell and whether there is the presence of trismus. Associated symptoms may include malaise, headache, rhinitis, cough and hoarseness. These symptoms are often benign in nature. However, can also be symptoms of malignancy. Patients with acid reflux may present with throat prob-lems. If this is linked with symptoms of dyspepsia or gastro-oesophageal reflux it should be investigated (Fig. 4.1).
Mouth and Throat Assessment
Tongue depressors, (Fig. 4.2) typically a disposable wooden spatula, are used to depress the tongue to allow the clinician to inspect the patient’s mouth and throat structures. Again an otoscope can be used as a torch to improve visualisation of the mouth and throat. A clinician should always wear gloves when performing an oral examination.
Oral mucosa
Pain Mouth Saliva
Taste
Ageusia
Parageusia
Dysgeusia
Hypogeusia
Reduced
Increased
General conditions andmedications
Ulcerations
Blisters
Bullae
Referred
Local tenderness
Odynophagia
Fig. 4.1 Mouth anamnesis map
Fig. 4.2 Tongue depressor
4 Laryngology

57
Mouth, throat and neck examination
• Scars and nodularity• Symmetry of the face and lips• Speech quality• Teeth• Soft and hard palate• The oral mucosa and the retro-molar trigon• Palpation of the floor of the mouth, neck, and salivary glands
Sore Throat
It is a frequent symptom and often associated with viral upper respiratory tract infection.
Pharyngitis
Clinical Presentation• Sore throat or dryness of the throat• Worse in the morning• Absence of systemic impairment• The patient may have sense of nasal obstruction especially at night• Cold symptoms
– Acutes – Chronic (Fig. 4.3)
Examination• Check the nasal passages• Check the sinuses• Check oropharynx, mouth, and tonsils• Assess cervical lymph nodes
Clinical Management• Invite to stop smoking• Advise to stop or reduce to recommended limits alcohol intake• Refer to a specialist in case of failure to respond to previous approaches
Other Causes of Pharyngitis
• Iatrogenic, from prolonged use of antibiotics or topical steroid• Anti-inflammatory causing agranulocytosis• Dental caries
Sore Throat

58
• Tobacco• GORD• Alcohol• Occupational irritants• Vocal abuse• Venereal diseases
RED FLAGS
Presence of traces of blood
Smoker/ Age greater than 40 years
Unilaterality
Tonsillitis (Fig. 4.4)
Clinical Presentation• Major general prostration• Fever• Cervical adenopathy• Otalgia• Halitosis
Fig. 4.3 Chronic pharyngitis
4 Laryngology

59
ExaminationThe Centor criteria are particularly useful to corroborate the diagnostic suspect giv-ing an indication of the likelihood of a sore throat being due to bacterial infection. The criteria are:
• Tonsillar exudate• Tender anterior cervical adenopathy• Fever over 38 °C (100.5 °F) by history• Absence of cough
If 3 or 4 of Centor criteria are met, the positive predictive value is 40–60%. The absence of 3 or 4 of the Centor criteria has a fairly high negative predictive value of 80%. Also of good clinical value is the streptococcal score card. This gives an indication of the likelihood of a sore throat being due to infection with group A beta- haemolytic streptococci (GABHS). The criteria are (Centor et al. 1981):
• Age 5–15 years• Season (late autumn, winter, early spring)• Fever (≥38.3 °C [≥101 °F])• Cervical lymphadenopathy• Pharyngeal erythema, oedema, or exudate• No symptoms of a viral upper respiratory infection (conjunctivitis, rhinorrhoea,
or cough)
If 5 of the criteria are met, a positive culture for GABHS is predicted in 59% of children; if 6 of the criteria are met, a positive culture is predicted in 75% of children.
Fig. 4.4 Bacterial tonsillitis
Sore Throat

60
Peri-tonsillar Cellulitis
• Peri-tonsillar redness and oedema• Lock of the jaw, but not marked
Peri-tonsillar Abscess
• Evolution of peri-tonsillar cellulitis• Symptoms and signs of peri-tonsillar cellulitis• Lockjaw
ExaminationThe appearance of the tonsils between episodes of acute tonsillitis does not help much the diagnosis. At times, the tonsils are hypertrophic, sometimes to the point to cause snoring, or airway obstruction. In other cases, they may be cryptic. Some caseous material may be found in the cryptae of the tonsils, hinting chronic inflam-mation with dysfunctional tonsils. During periods of acute sore throat, in case of viral infection, you may observe:
• Redness and oropharyngeal mucosa and oedema with or without ulcerations
• In the case of unilateral ulceration of the pharynx, consider herpetic infection
• Petechiae of the palate• Oedema of the uvula• Cold sores of the nostril
In case of tonsillitis, you can demonstrate:
• Limited redness, swelling of the tonsils and of the tonsillar pillars• Pus in the tonsillar crypts• Halitosis• “Hot potato voice”• Redness of the face• Fever• Painful cervical adenopathy• General malaise
In the case of mononucleosis:
• Halitosis• “Hot potato voice”• Petechiae on the palate• Tonsils swollen with whitish patina• Fever• Adenopathy• Liver and spleen may be enlarged• Jaundice may be present• General malaise
4 Laryngology

61
Clinical Management of Tonsillitis• In sore throats without lockjaw, or other complications, soluble aspirin is a good
option in the adult only. In children, paracetamol and ibuprofen should be preferred.• The majority of patients with sore throat may have already tried to manage their
disease for at least a day with analgesia before presenting to the family physician.• At this point, having made a diagnosis of tonsillitis, antibiotic therapy, preferably
with penicillin V, erythromycin, or clarithromycin, for 10 days rather than 5 or 7 days, is an option (Little et al. 1997).
• Refer to the specialist in case of recurrent tonsillitis requiring antibiotic therapy in line with local referring policy.
Clinical Management of Infectious Mononucleosis• Do not advise antibiotic therapy as this would not help.• It may require a prolonged period of rest.• Liver disease may occur, but often it is not clinically significant (Fig. 4.5).
• The Monospot test or blood smear on a slide helps to confirm the diagnostic suspect
• Supra-infection may require specific treatment
RED FLAGS
Trismus (reduced mouth opening)
Hot potato voice
Patients unable to swallow their own saliva or smallamounts of fluid
Quinsy/abscess
Meningism
Fig. 4.5 Glandular fever
Sore Throat
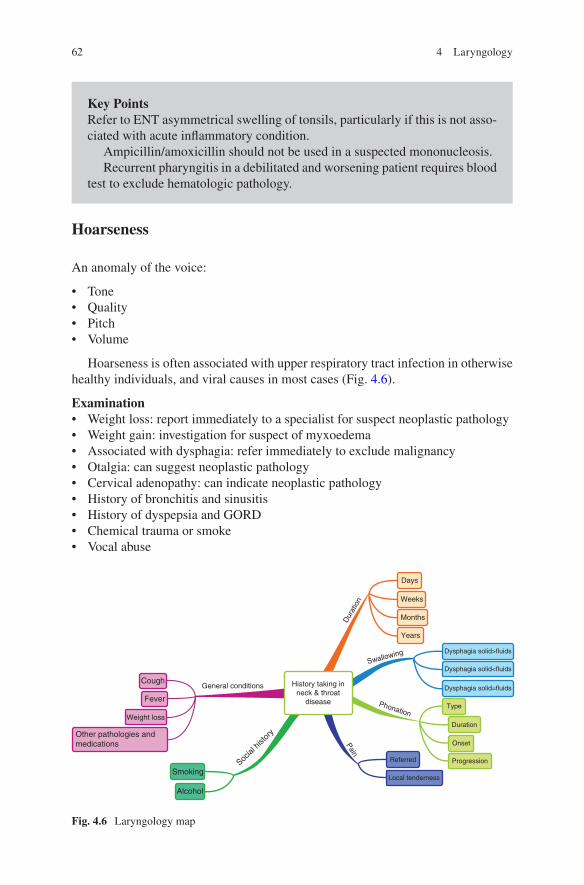
62
Hoarseness
An anomaly of the voice:
• Tone• Quality• Pitch• Volume
Hoarseness is often associated with upper respiratory tract infection in otherwise healthy individuals, and viral causes in most cases (Fig. 4.6).
Examination• Weight loss: report immediately to a specialist for suspect neoplastic pathology• Weight gain: investigation for suspect of myxoedema• Associated with dysphagia: refer immediately to exclude malignancy• Otalgia: can suggest neoplastic pathology• Cervical adenopathy: can indicate neoplastic pathology• History of bronchitis and sinusitis• History of dyspepsia and GORD• Chemical trauma or smoke• Vocal abuse
Key PointsRefer to ENT asymmetrical swelling of tonsils, particularly if this is not asso-ciated with acute inflammatory condition.
Ampicillin/amoxicillin should not be used in a suspected mononucleosis.Recurrent pharyngitis in a debilitated and worsening patient requires blood
test to exclude hematologic pathology.
Social
hist
ory
General conditions History taking inneck & throat
disease
Dur
atio
n
Phonation
Pain
Swallowing
Years
Months
Weeks
Days
Dysphagia solid>fluids
Dysphagia solid<fluids
Dysphagia solid=fluids
Type
Duration
Onset
ProgressionReferred
Local tenderness
Cough
Fever
Other pathologies andmedications
Weight loss
Smoking
Alcohol
Fig. 4.6 Laryngology map
4 Laryngology
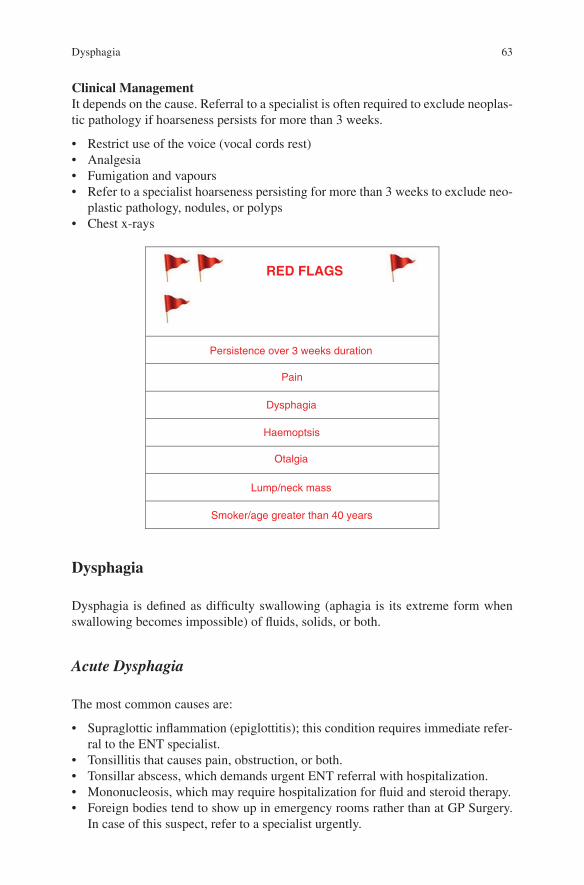
63
Clinical ManagementIt depends on the cause. Referral to a specialist is often required to exclude neoplas-tic pathology if hoarseness persists for more than 3 weeks.
• Restrict use of the voice (vocal cords rest)• Analgesia• Fumigation and vapours• Refer to a specialist hoarseness persisting for more than 3 weeks to exclude neo-
plastic pathology, nodules, or polyps• Chest x-rays
RED FLAGS
Persistence over 3 weeks duration
Pain
Dysphagia
Haemoptsis
Otalgia
Lump/neck mass
Smoker/age greater than 40 years
Dysphagia
Dysphagia is defined as difficulty swallowing (aphagia is its extreme form when swallowing becomes impossible) of fluids, solids, or both.
Acute Dysphagia
The most common causes are:
• Supraglottic inflammation (epiglottitis); this condition requires immediate refer-ral to the ENT specialist.
• Tonsillitis that causes pain, obstruction, or both.• Tonsillar abscess, which demands urgent ENT referral with hospitalization.• Mononucleosis, which may require hospitalization for fluid and steroid therapy.• Foreign bodies tend to show up in emergency rooms rather than at GP Surgery.
In case of this suspect, refer to a specialist urgently.
Dysphagia
64
Progressive Dysphagia
This should always trigger the suspect of oesophageal or pharyngeal neoplastic pathology in particular when associated to:
• History of weight loss and fatigue• First to solids and then to both fluids and solids• Hoarseness
Cough when drinking may suggest the possibility of aspiration. Anamnestic data suggesting a benign cause of progressive dysphagia are:
• Regurgitation: a barium swallow allows you to confirm a pharyngeal or oesopha-geal diverticulum. Refer to the specialist.
• A history of GORD suggests the possibility of a stricture due to oesophageal mucosal ulceration. Even in this case, refer to the specialist.
Other Causes
• Neurogenic dysphagia• Connective tissue disorders such as systemic sclerosis
Globus Pharyngeus
The sense of obstruction in the throat is a functional problem and it is otherwise known as globus pharyngeus, or hystericus. The term ‘pseudo-dysphagia’ also describes adequately the problematic.
• The knot in the throat improves swallowing, but returns immediately after.• It is variable.• There are no signs of obstruction.• There is often anxiety.
The patient should be referred to the specialist for endoscopic evaluation.
ExaminationGeneral examination should be looking for abnormal findings such as:
• Pallor• Weight loss• Abdominal masses• Abnormal chest examination• Cranial nerve abnormalities
4 Laryngology
65
Local/district examination:
• Angular cheilitis• Glossitis• Neck masses• Masses of the oral cavity• Movements of the tongue, palate and pharynx• Sensory examination of mouth and pharynx
Clinical ManagementThe investigations should include:
• X-ray of the neck with side view• Chest x-ray• Barium• Basic blood tests
In case of a suspect neurological disorder, refer immediately to a specialist.
RED FLAGS
Ear Pain
Sore Throat
Symptoms of lateralization
Persistent hoarseness
Snoring
Snoring is the snorting or rattling noise some people may do when breathing during sleep. The noise comes from the vibration of the soft palate due to a turbulent air flow. Also the vibration for the mouth tissues, nose and throat can contribute signifi-cantly to its generation. Some people snore infrequently and the sound they make are not particularly loud, while others may snore every night loudly enough to disturb other people. From an anatomical point of view snoring is due to loss of tone of the muscles of the soft palate, including those of the uvula, but there are many contribut-ing factors to it, all of them contributing to the speed and turbulence of the air flow, or the capacity of vibrating of the soft tissues of the upper aero-digestive tract.
Snoring

66
Key Anamnestic Points
Apnoea: snoring may be associated with apnoeic episodes. Few, short episodes of apnoea may occur also in normal individuals, but apnoeic episodes that last more than 10 s and ending with a loud snoring, or heave with awakening, often temporary and partial, are suggestive of obstructive sleep apnoea syndrome (OSAS).
Epworth Sleeping Score: reference scale that makes possible to evaluate the severity of daytime sleepiness. With a score 10 < ESS the OSAS is unlikely. Sometimes children with OSAS may be hyperactive during the day (Fig. 4.7).
ExaminationGeneral examination
• Obesity• Arterial hypertension
Localized/district examination
• Nasal obstruction• Soft palate ptosis• Short, large neck• Mandibular retrognathism• Hypertrophy of tonsils• Hypertrophy of adenoids• Hypertrophy of lingual tonsil
Clinical Management• Weight loss.• Smoking cessation.• Avoid alcoholic drinks for 4 h before bedtime.
Fig. 4.7 OSAS and sites of obstructions of the upper airways
4 Laryngology

67
• Do not use hypnotics, or muscle relaxers at night.• Trial of mandibular snore ban type pusher. Optionally, refer the patient for poly-
somographic studies. A respiratory physician may advise continuous positive airway pressure (CPAP).
CPAP is a small machine that delivers a constant and steady air pressure through a hose to a mask or nose piece. Remember to tell the patient it is its obligation to inform the Driving Vehicles Licensing Authority.
RED FLAGS
Daytime sleepiness
Sleep apnoea observed by another person
References
Little P, Gould C, Williamson I, et al. (1997) Reattendance and complications in a randomised trial of prescribing strategies for sore throat: the medicalising effect of prescribing antibiotics. BMJ 315:350–352
Centor RM, Witherspoon JM, Dalton HP, Brody CE, Link K (1981) The diagnosis of strep throat in adults in the emergency room. Med Decis Making. 1(3):239–246
References

69© Springer International Publishing AG 2017 E. Cervoni, K. Leech, ENT in Primary Care, DOI 10.1007/978-3-319-51987-6_5
Chapter 5Head and Neck
The Oral Cavity and the Neck
Any of the structures of the mouth may be involved in local disease or may be part of wider systemic pathology. Therefore a thorough history is needed to determine between the two. Certain symptoms such as xerostomia (dry mouth) should not be considered in isolation. This may be as a result of drugs, gland dysfunction or diabe-tes. Ulcerations of the oral mucosa could be as a result of local disease such as poor dental hygiene, gingivitis or systemic illnesses including anaemia, AIDS or HIV. Any ulceration that is red, white or pigmented lasting for longer than 3 weeks should be investigated. Angular stomatitis and tongue/mouth soreness could be from a haema-tological cause or iron deficiency. Any intraoral swellings that increase in size or pain associated with eating are usually as a result of salivary gland pathology. Patients who present with any lumps in the neck should be referred to an ENT specialist, so that they can be appropriately investigated to determine if they are secondary lymph nodes and the likely primary source. In patients presenting with a neck lump, it is worth investigating any symptoms of the tongue, mouth, nose or throat as these may identify the primary site. Enlarged lymph nodes may be a result of a previous infec-tion, so the clinician should determine if the patient has had any recent illnesses or infections. Symptoms associated with under-active or over-active thyroid should be determined. Associated symptoms such as weight loss, night sweats and malaise are suggestive of systemic diseases such as AIDS or lymphoma.
Neck Lump
All patients with an unexplained lump in neck that recently appeared, or a lump that was not diagnosed before and has changed during a period from 3 to 6 weeks, should be referred urgently to an ENT specialist.

70
Salivary Gland Lump
Patients with persistent unexplained swelling of a parotid, sublingual, or subman-dibular gland should be referred urgently to ENT.
Facial Palsy
The facial nerve controls the muscles of the facial expression and stapedius, the lac-rimal and submandibular glands, and the sensory function of the anterior 2/3 of the tongue. Hence, as well as facial droop, patients may present with drooling, hyperacu-sis, altered taste, speech issues, earache, dry eye and reduced corneal reflex. Facial palsy can be classified in central or peripheral. The two forms are differentiated clini-cal examination since the facial motors nuclei are two, one top and one bottom bilat-erally innervated that receives only a contra-lateral innervations. It follows that:
• Central facial palsy is incomplete, affecting only the lower half of the contra- lateral face.
• Peripheral facial paralysis is complete and ipsilateral and its severity can be clas-sified according to House and Brackmann (1985) (Fig. 5.1).
Herpes Zoster
Herpes affects the ear, mouth, pharynx and facial nerve. Even the acoustic nerve may be affected and is otherwise known by the name of Ramsay-Hunt.
Clinical Presentation• Ramsay-Hunt syndrome presents with severe otalgia Hunt JR (1907).• Burning pain several hours before onset of typical herpetic blistering.• Blistering rash will appear around the ear, face and sometimes in the oral
cavity.• The syndrome generally causes more severe symptoms and has a worse progno-
sis than Bell’s palsy has. Even if the latter, of which the exact reasons remain unclear, maybe likewise ascribed to herpetic infection.
• Accompanying vestibular symptoms such as vertigo, nausea and vomiting may be present.
5 Head and Neck

71
• Hearing can be reduced, with or without tinnitus.• The eye and mouth may be affected; the latter with alteration to taste, known as
disgeusia.
Examination• Examination will demonstrate a vesicular rash• Examination of facial nerves• Assessment of taste• Otoscope and hearing assessment• Pain and/or paraesthesia• If the vestibular system is affected, vestibular testing would show a deficit on the
same side of the lesion.• Middle ear pathology – The involvement of the facial nucleus lower motor neu-
ron is associated with ipsilateral otorrhoea and/or cholesteatoma.• Post-traumatic causes – Most often occur in the emergency room while occa-
sionally patients seek advice from part of GP. In this case, the patient should be reported immediately to the specialist. They may be: a temporal bone fracture, post-surgical, sharp/blunt facial trauma, or a birth canal trauma
Clinical Management• Analgesics• Acyclovir (topical or oral) if onset of symptoms is within 48 h• Protection of the cornea• EMG evaluation
Fig. 5.1 Peripheral facial paralysis
Facial Palsy

72
RED FLAGS
Suspect of stroke
Suspect of mastoiditis
Head trauma
Severe otitis externa
Bell’s Palsy
Bell’s palsy is a diagnosis of exclusion.
Clinical Presentation Complete• Can be preceded by otalgia.• Often the patient is believed to have had a stroke.
Examination Complete• The sense of taste in the front 2/3 of the tongue is affected, and the patient may
have watery eye and reduced corneal reflex. However, their recovery is often faster than the recovery of the motor function.
Clinical Management• In 75% of the cases, it resolves within 3 weeks from the onset and the lack of a
resolution within that span of time should suggest a request for specialist visits.• ACTH and corticosteroids have not been confirmed as effective. However, it is
believed that steroid tablets such as prednisolone help to reduce inflammation and are normally taken for 10 days.
• The eye should be protected and artificial drops prescribed.• In the case of a suspicion of damage to the cornea, refer to ophthalmologist.• In the case of a slow recovery, suggest physiotherapy with transcutaneous elec-
trical stimulation.• Consider alternative diagnoses in case of multiple neuropathies.
RED FLAGS
Otitis media
Cholesteatoma
Parotid tumour
Malignant otitis externa
Bilateral onset
5 Head and Neck

73
Other Causes
Other causes may be an acoustic neuroma, a parotid gland malignancy, a malignant otitis externa or Lyme disease.
References
House JW, Brackmann DE (1985) Facial nerve grading system. Otorlaryngol Head Neck Surg 93(2):146–147
Hunt JR (1907) On herpetiform inflammation of the geniculate ganglion: a new syndrome and its complications. Nerve Ment Dis 34:73
References

75© Springer International Publishing AG 2017 E. Cervoni, K. Leech, ENT in Primary Care, DOI 10.1007/978-3-319-51987-6_6
Chapter 6Post-operative ORL
Adenoidectomy
After adenoidectomy, the patient may experience post-operative bleeding and pain.
Post-operative BleedingBleeding after adenoidectomy surgery requires immediate hospitalization, with posterior nasal tamponade, if necessary.
Post-operative PainIt is in general minimal. If otalgia, perform otoscopy to exclude ear infection.
Trans-tympanic Tubes
It is not uncommon for a GP to be consulted by parents alarmed by the appearance of ear discharge from the very same ear where a drainage tube, this being a grommet or a T-tube, had been positioned by the ENT specialist some weeks or months before. The discharge may follow an upper respiratory tract infection or a bath with subsequent infection due to contaminated water, for example, penetrated in the mid-dle ear. It is reasonable to suggest topical antibiotic therapy as eardrops, or an oral antibiotic. The GP should be mindful of the ototoxicity of the aminoglycosides usu-ally present in the eardrops. Eye drops with ofloxacin or ciprofloxacin may be very helpful in similar circumstances. There is no conclusive evidence that swimming is risky for the child with trans-tympanic drainage. It is preferable to avoid shampoo and conditioner in your ear (Fig. 6.1).
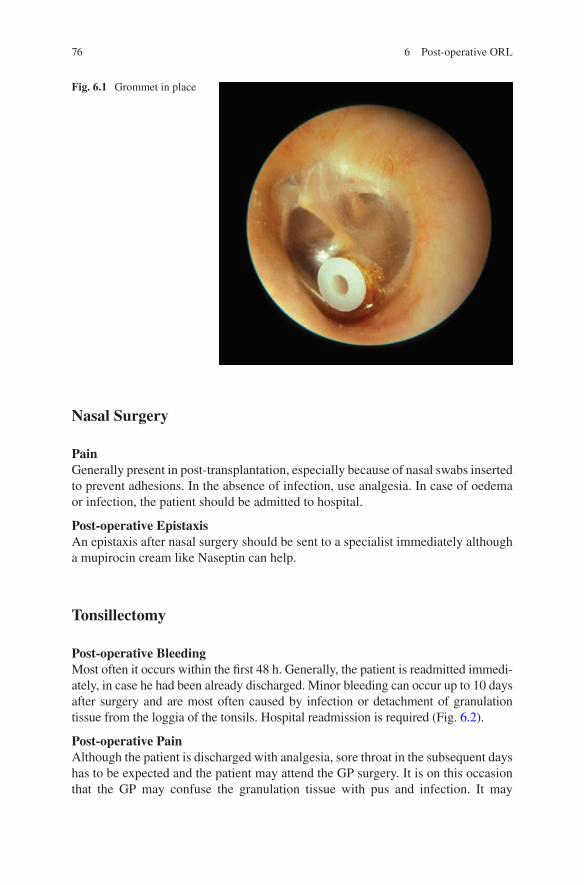
76
Nasal Surgery
PainGenerally present in post-transplantation, especially because of nasal swabs inserted to prevent adhesions. In the absence of infection, use analgesia. In case of oedema or infection, the patient should be admitted to hospital.
Post-operative EpistaxisAn epistaxis after nasal surgery should be sent to a specialist immediately although a mupirocin cream like Naseptin can help.
Tonsillectomy
Post-operative BleedingMost often it occurs within the first 48 h. Generally, the patient is readmitted immedi-ately, in case he had been already discharged. Minor bleeding can occur up to 10 days after surgery and are most often caused by infection or detachment of granulation tissue from the loggia of the tonsils. Hospital readmission is required (Fig. 6.2).
Post-operative PainAlthough the patient is discharged with analgesia, sore throat in the subsequent days has to be expected and the patient may attend the GP surgery. It is on this occasion that the GP may confuse the granulation tissue with pus and infection. It may
Fig. 6.1 Grommet in place
6 Post-operative ORL

77
happen that the GP replaces an antibiotic that the ENT department initiated, assum-ing that this was not working. In addition, we must be cautious in the use of soluble aspirin for the risk of bleeding associated with NSAIDs. Paracetamol, codeine and ibuprofen are all valuable alternatives.
It is helpful to assure patients and their relatives that within a couple of weeks the situation will be resolved. As for the food, hard foods like nuts and chips should be avoided in favour of a liquid or soft diet. Eating little and often can be beneficial. Avoid a two-large-meals diet.
Oncology ORL
Neoplastic Suspect in ENT
The request for an urgent ENT appointment is recommended whenever you suspect a malignancy. Several signs and symptoms may be the trigger and they shall be illustrated in the following paragraphs.
Hoarseness
If hoarseness persists for more than 3 weeks, particularly in smokers over 50 years old and heavy drinkers, we recommend an urgent CXR. Patients with positive results must be sent urgently to a team specialized in the management of lung can-cer. Patients with a negative result must be sent urgently to a team that specializes in cancer of the head and neck.
Fig. 6.2 Tonsillectomy
Oncology ORL
78
Sore Throat
In patients with sore throat unexplained and persistent, it is recommended that a request for an urgent ENT assessment should be arranged.
Otalgia with Sore Throat or Neck
In patients with unilateral unexplained pain in the area of the head and neck for more than 4 weeks, associated with ear pain (otalgia), but with normal otoscopy, you should formulate a request for urgent ENT assessment.
6 Post-operative ORL
79© Springer International Publishing AG 2017 E. Cervoni, K. Leech, ENT in Primary Care, DOI 10.1007/978-3-319-51987-6_7
Chapter 7Pharmacology
Antibiotic Prescribing
When prescribing, or considering prescribing antibiotics, it is advisable to:
• Document the indication/rationale for antimicrobial therapy, including clinical criteria relevant to this.
• Review and document the patient’s allergy status.• Ensure the choice of antibiotic complies with the antibiotic guidelines whenever
possible and to keep a record of any clinical criteria relevant to the choice of agent.• Document a management plan including duration of the treatment or review
date.• Where relevant, consider drainage of pus or surgical debridement/removal of
foreign material. To this aim, immediate ENT referral may be required.
Common ENT Antibiotic Prescribing in Primary Care (Fig. 7.1)
Common Prescriptions
Rhinitis
Beclometasone nasal sprayBudesonide nasal spray (Rhinocort Aqua)Betamethasone nose drops (Betnesol, Vistamethasone)Ipratropium bromide 21 μg/metered spray (Rinatec)Xylometazoline hydrochloride 0.1% (Otrivine)Fluticasone propionate 50 μgAzelastine hydrochloride 137 μg/metered spray (Dymista)
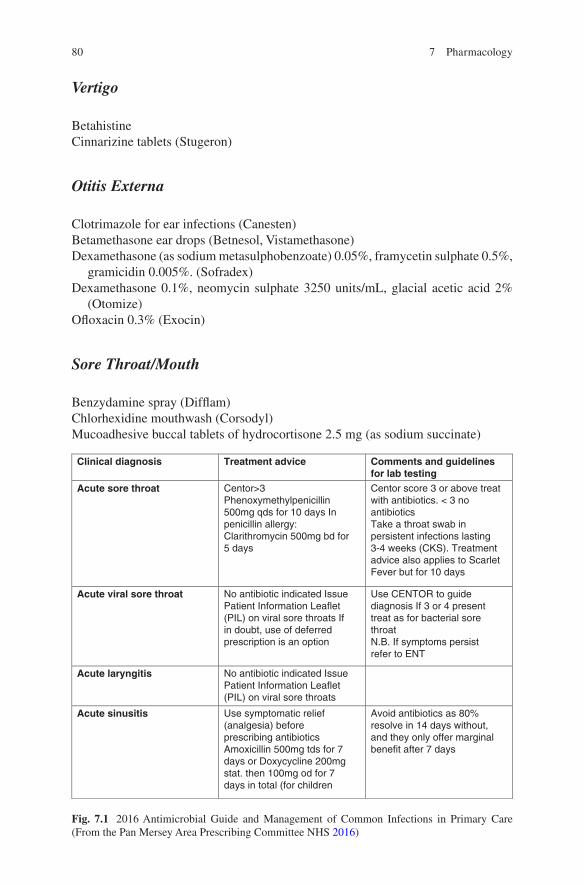
80
Fig. 7.1 2016 Antimicrobial Guide and Management of Common Infections in Primary Care (From the Pan Mersey Area Prescribing Committee NHS 2016)
Clinical diagnosis Treatment advice Comments and guidelinesfor lab testing
Acute sore throat Centor>3Phenoxymethylpenicillin500mg qds for 10 days Inpenicillin allergy:Clarithromycin 500mg bd for5 days
Centor score 3 or above treatwith antibiotics. < 3 noantibioticsTake a throat swab inpersistent infections lasting3-4 weeks (CKS). Treatmentadvice also applies to ScarletFever but for 10 days
Acute viral sore throat No antibiotic indicated IssuePatient Information Leaflet(PIL) on viral sore throats Ifin doubt, use of deferredprescription is an option
Use CENTOR to guidediagnosis If 3 or 4 presenttreat as for bacterial sorethroatN.B. If symptoms persistrefer to ENT
Acute laryngitis No antibiotic indicated IssuePatient Information Leaflet(PIL) on viral sore throats
Acute sinusitis Use symptomatic relief(analgesia) beforeprescribing antibioticsAmoxicillin 500mg tds for 7days or Doxycycline 200mgstat. then 100mg od for 7days in total (for children
Avoid antibiotics as 80%resolve in 14 days without,and they only offer marginalbenefit after 7 days
Vertigo
BetahistineCinnarizine tablets (Stugeron)
Otitis Externa
Clotrimazole for ear infections (Canesten)Betamethasone ear drops (Betnesol, Vistamethasone)Dexamethasone (as sodium metasulphobenzoate) 0.05%, framycetin sulphate 0.5%,
gramicidin 0.005%. (Sofradex)Dexamethasone 0.1%, neomycin sulphate 3250 units/mL, glacial acetic acid 2%
(Otomize)Ofloxacin 0.3% (Exocin)
Sore Throat/Mouth
Benzydamine spray (Difflam)Chlorhexidine mouthwash (Corsodyl)Mucoadhesive buccal tablets of hydrocortisone 2.5 mg (as sodium succinate)
7 Pharmacology
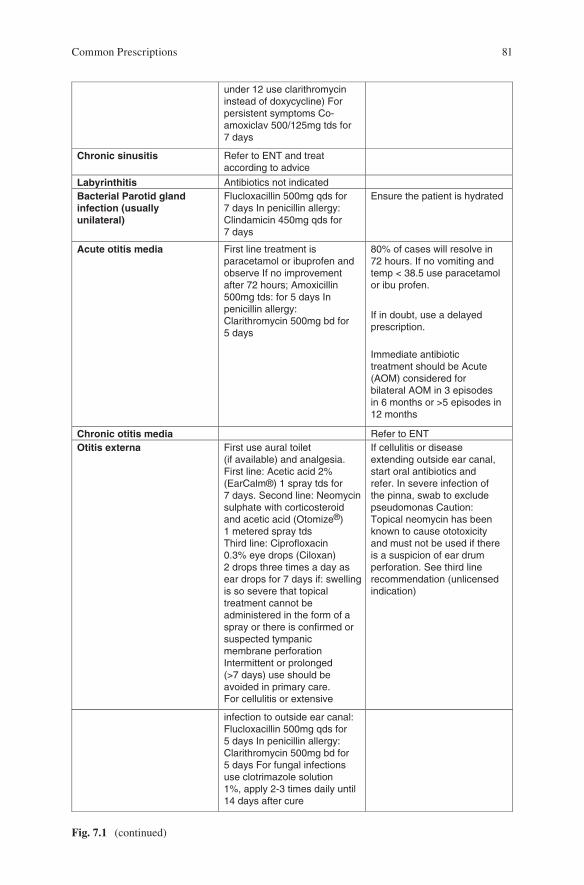
81
under 12 use clarithromycininstead of doxycycline) Forpersistent symptoms Co-amoxiclav 500/125mg tds for7 days
Chronic sinusitis Refer to ENT and treataccording to advice
Labyrinthitis Antibiotics not indicated Bacterial Parotid glandinfection (usuallyunilateral)
Flucloxacillin 500mg qds for7 days In penicillin allergy:Clindamicin 450mg qds for7 days
Ensure the patient is hydrated
Acute otitis media First line treatment isparacetamol or ibuprofen andobserve If no improvementafter 72 hours; Amoxicillin500mg tds: for 5 days Inpenicillin allergy:Clarithromycin 500mg bd for5 days
80% of cases will resolve in72 hours. If no vomiting andtemp < 38.5 use paracetamolor ibu profen.
If in doubt, use a delayedprescription.
Immediate antibiotictreatment should be Acute(AOM) considered forbilateral AOM in 3 episodesin 6 months or >5 episodes in12 months
Chronic otitis media Refer to ENT Otitis externa First use aural toilet
(if available) and analgesia.First line: Acetic acid 2%(EarCalm®) 1 spray tds for7 days. Second line: Neomycinsulphate with corticosteroidand acetic acid (Otomize®)1 metered spray tdsThird line: Ciprofloxacin0.3% eye drops (Ciloxan)2 drops three times a day asear drops for 7 days if: swellingis so severe that topicaltreatment cannot beadministered in the form of aspray or there is confirmed orsuspected tympanicmembrane perforationIntermittent or prolonged(>7 days) use should beavoided in primary care.For cellulitis or extensive
If cellulitis or diseaseextending outside ear canal,start oral antibiotics andrefer. In severe infection ofthe pinna, swab to excludepseudomonas Caution:Topical neomycin has beenknown to cause ototoxicityand must not be used if thereis a suspicion of ear drumperforation. See third linerecommendation (unlicensedindication)
infection to outside ear canal:Flucloxacillin 500mg qds for5 days In penicillin allergy:Clarithromycin 500mg bd for5 days For fungal infectionsuse clotrimazole solution1%, apply 2-3 times daily until14 days after cure
Fig. 7.1 (continued)
Common Prescriptions

82
Glue Ear
Autoinflation nasal balloon (Otovent)
Reference
Pan Mersey Area Prescribing Committee NHS (2016) Antimicrobial guide and management of common infections in primary care 11–14
7 Pharmacology

83© Springer International Publishing AG 2017 E. Cervoni, K. Leech, ENT in Primary Care, DOI 10.1007/978-3-319-51987-6
References
BMJ Best Practice (2016) Tonsilitis [online]. http://bestpractice.bmj.com/best-practice/mono-graph/598/diagnosis/criteria.html
British Society of Audiology (2014) Recommended procedure for Hallpike maneuver [online]. http://www.thebsa.org.uk/wp-content/uploads/2014/04/HM.pdf
Centor RM, Witherspoon JM, Dalton HP, Brody CE, Link K (1981) The diagnosis of strep throat in adults in the emergency room. Med Decis Making 1(3):239–246
Corbridge RJ (2011) Essential ENT. 2nd edn. CRC Press, LondonCross S, Rimmer M (2007) Nurse practitioner manual of clinical skills, 2nd edn. Elsevier, LondonFujisawa T (2015) Allergen immunotherapy in children. Arerugi 64:787–794Hain TC (1997) Approach to the Vertigo. In: Practical neurology. Lippincott-Raven, PhilidelphiaHarkin H (2007) Ear care guidance from the NHS Modernisation Agency. NHS Modernisation,
LondonHelman CG (1981) Disease versus illness in general practice. J R Coll Gen Pract 31:548–562House JW, Brackmann DE (1985) Facial nerve grading system. Otorlaryngol Head Neck Surg
93(2):146–147Hunt JR (1907) On herpetiform inflammation of the geniculate ganglion: a new syndrome and its
complications. Nerve Ment Dis 34:73Kurtz SM, Silverman JD (1996) The Calgary-Cambridge Referenced Observation Guides: an aid
to defining the curriculum and organising teaching in communication training programmes. Med Educ 30:83–89
Lemajic-Komazec S, Komazec Z (2006) Initial evaluation of vertigo. Med Pregl 59(11–12):585–590Lloyd S, Tan ZE, Taube MA, Doshi J (2014) Development of an ENT undergraduate curriculum
using a Delphi survey. Clin Otolaryngol 39:281–288Neighbour R (1987) The inner consultation. Lancaster, MTPPan Mersey Area Prescribing Committee NHS (2016) Antimicrobial guide and management of
common infections in primary care 11–14Pendleton D, Schofield T, Tate P, Havelock P (1984) The consultation: an approach to learning and
teaching. Oxford University Press, OxfordSmith R (2003) Thoughts for new medical students at a new medical school. BMJ.
327(7429):1430–1433
85© Springer International Publishing AG 2017 E. Cervoni, K. Leech, ENT in Primary Care, DOI 10.1007/978-3-319-51987-6
AAdenoidectomy, 51, 75Adult deafness, 25Allergic rhinitis, 40, 43, 45–48, 53
BBell’s palsy, 70, 72
CChild deafness, 23
DDysphagia, 55, 62–64
EEar syringe, 9Epistaxis, 2, 39, 42–44, 76
FFacial palsy, 6, 70–71Fistula test, 10, 37–38Frenzel goggles, 8, 9, 31Fukuda stepping test (FST), 32
GGlobus pharyngeus, 64–65Glue ear, 24, 25, 82
HHalitosis, 58, 60Hallpike test, 32–33Head-shaking nystagmus, 31, 32Hearing tests, 8, 25–30Herpes zoster, 70–72Hoarseness, 2, 55, 56, 62–65, 77–78
NNasal obstruction, 39, 40, 44, 45, 47–50, 52,
53, 57, 66Nasal polyps, 45, 48–50, 53, 54
OOtalgia, 5, 6, 11–12, 15, 16, 19, 21, 23–25,
39, 58, 62, 70, 75, 78Otitis externa, 12–13, 18, 19, 28, 29, 73, 80,
81Otoscope, 6, 7, 10, 19, 28, 29, 37, 40, 41, 56,
71
PPharyngitis, 57–58, 62
RRecurring rhinosinusitis, 53–54Rhinitis, 45, 53, 56, 79Rhinosinusitis, 53–54Rinne, 8, 25–27, 30
Index
86
SSaccades, 31Septal deviation, 42, 45, 50, 53Sinusitis, 40, 48, 52–54, 62, 80, 81Smooth pursuit, 31Snoring, 60, 65–66Sore throat, 39, 55–62, 76, 78, 80–81
TTinnitus, 2, 6, 19, 21, 22, 29–36, 70Tonsillectomy, 76–77
Tonsillitis, 5, 11, 15, 58–63Trans-tympanic tubes, 75–76Tuning forks, 8, 9, 26, 30
VVasomotor rhinitis, 47–48Vertigo, 6, 19, 21, 22, 33–38, 70, 80
WWeber, 8, 27–30
Index