fereshteh ashtari md professor of neurology i sfahan university of medical sciences
TRANSCRIPT

Epilepsy
Fereshteh Ashtari MDProfessor of Neurology
Isfahan University of Medical Sciences
یا Seizureتشنج
در ناگهانی و پاروکسیسمال حاالت و عالئم بروز. مغز نرونهای زیاد و طبیعی غیر الکتریکی اثرفعالیت
اساس بر شود می ایجاد تشنج اثر در که عالئمی. است متفاوت دیسشارژ بروز محل
کوتاه بطور و شده ایجاد ناگهانی بطور عالئم اینیا و حرکتی اختالالت یا هوشیاری اختالل بروز باعث
. گردد می بیمار در حسی
بنام باشد داشته حرکتی جزء تشنج اگرConvulse . شود می خوانده

Epilepsy صرع یا
تشنج حمالت دچار فرد ان در که شرایطی. گردد می متناوب
خاصی شرایط در تشنج تکرار یا و تشنج بار یکنمی خوانده صرع است پیشگیری قابل که
شود.
Epilepsy: two or more unprovoked
seizure.
Incidence : 0.3-0.5%.
Prevalence: 0.5-1%

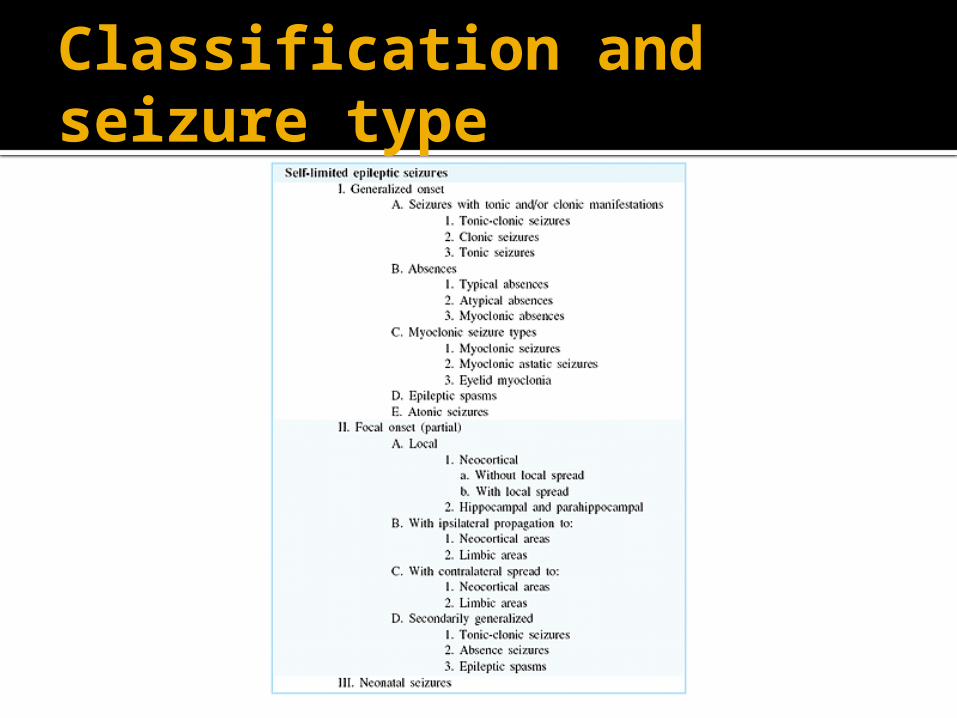
Classification and seizure type
What Causes a Seizure ?
in newborns and infants:
birth trauma congenital (present at birth)
problems fevermetabolic or chemical
imbalances in the body

children, adolescents, and adults:
alcohol or drugs head trauma infection unknown reasons

What are the Symptoms of a Seizure?
staring
jerking movements of the arms and legs
stiffening of the body
loss of consciousness
breathing problems or breathing stops
loss of bowel or bladder control
falling suddenly for no apparent reason
not responding to noise or words for brief periods
appearing confused or in a haze
sleepiness and irritable upon waking in the morning
periods of rapid eye blinking and staring
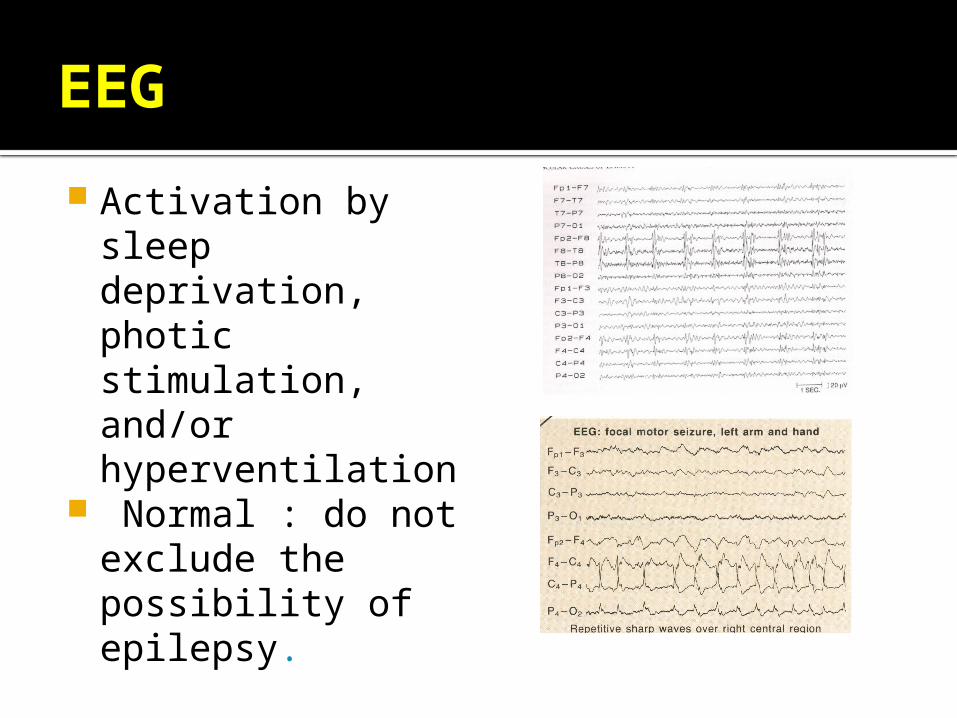
EEG
Activation by sleep deprivation, photic stimulation, and/or hyperventilation
Normal : do not exclude the possibility of epilepsy.
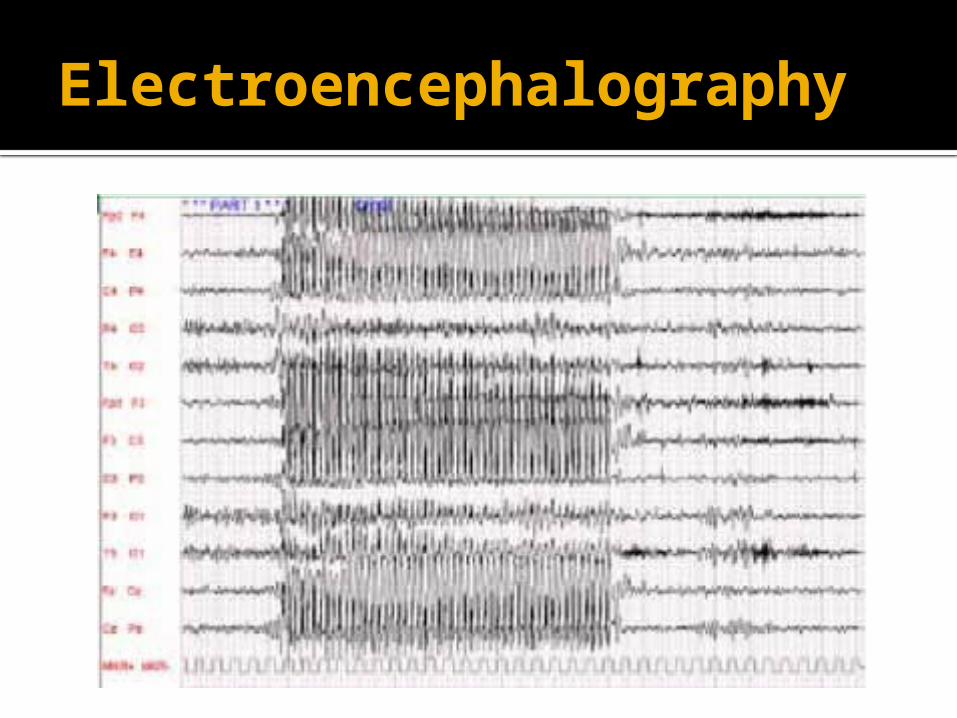
Electroencephalography



Seizure types
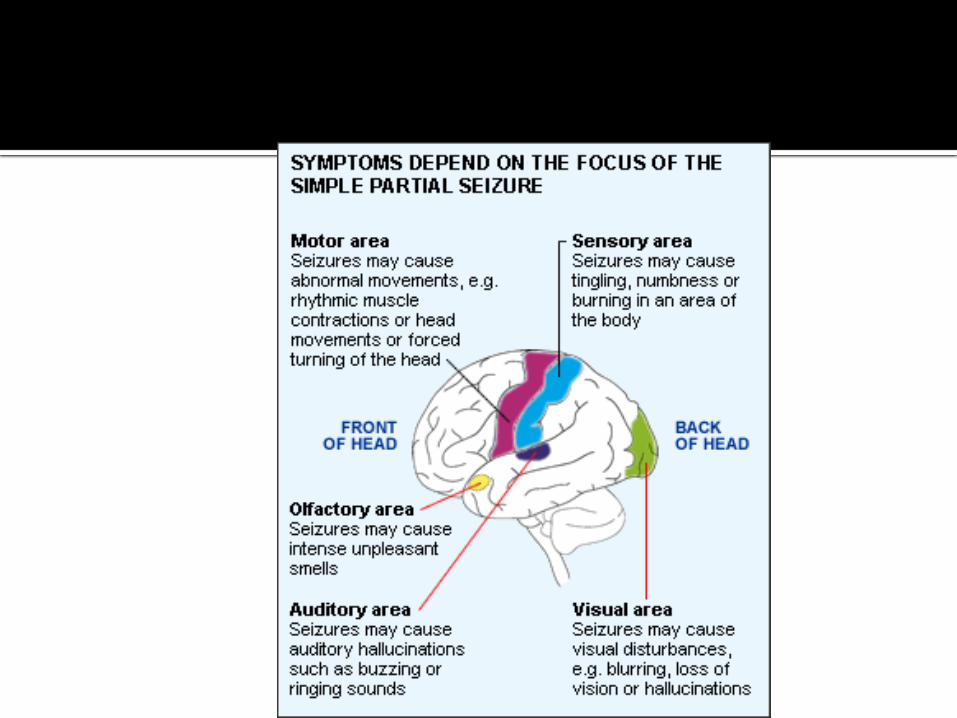
Partial (focal):the seizure activity is restricted to discrete areas of the cerebral cortex. usually associated with structural abnormalities of the brain.
Generalized : involve diffuse regions of the brain simultaneously.
Result from cellular biochemical or structural abnormalities that have a more widspread distribution.

Partial seizure: simple: consciousness is fully preserved
during the seizure. Complex: consciousness is impaired . the symptomatology is more complex
and the seizure is termed complex partial seizure.
Kinds of partial seizure
Simple partial seizure Complex partial seizure Secondary generalized seizure

Simple partial seizure: motor, sensory , autonomic or psychic symptoms without alteration
in consciousness.

Complex partial seizure: Frequently begin with an aura Ictal phase : often sudden behavioral
arrest or motionless stare whitch marks the onset of the period of amnesia.
Accompanied by automatisms( involuntary automatic behaviors that have a wide range manifestations such as chewing, lip smacking , swallowing, ...)
Secondary generalized seizure

Temporal lobe epilepsy
Aura Ictal : automatism , GMSPostictal15-30 y

Generalized seizure
Arise from both cerebral hemispheres simultaneously. Absence Primary tonic clonic seizure Myoclonic epilepsy
Absence seizure(petitmal):
Sudden, brief laps of consciousness without loss of postural control
seconds No postictal confusion Begin in childhood(4-8) May recurs hundreds times EEG is characterized

Petitmal
2-15 s 5-15 y After awaking Exacerbate by hyperventilation ,exersise Simple , complex

Generalized tonic clonic seizure:
Begin abruptly without warning No aura Initial phase is tonic contraction of
muscles ( ictal cry, contraction of jaw and tongue biting , apnea
Clonic phase Post ictal
GMS STAGES:
Perodormal Aura Tonic Clonic Clonic postictall

Atonic seizure: sudden loss of postural muscles lasting 1-2 sec
Consciousness briefly impaired but usually no post ictal confusion

Myoclonic seizure:
Sudden and brief muscle contraction One part of body or entire the body. Sudden jerking movement

Epilepsy syndromes
Disorders in which epilepsy is predominant features and there is sufficient evidences to suggest common underlying mechanisms'.
Juvenile myoclonic epilepsy Lennox-Gastaut syndrom Mesial temporal lobe epilepsy
syndrome
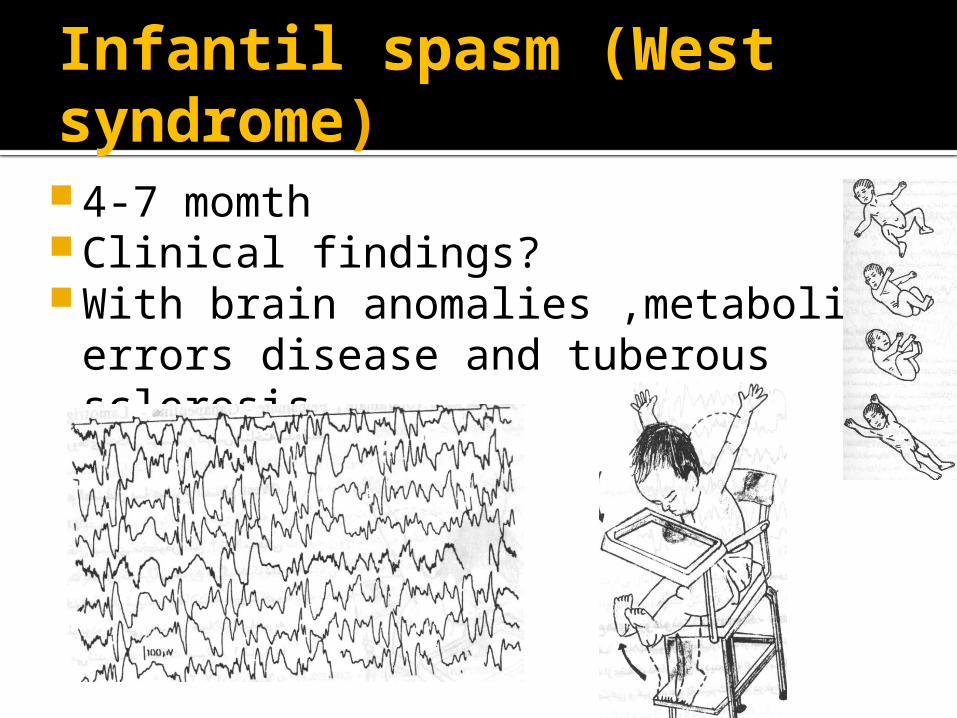
Infantil spasm (West syndrome) 4-7 momth Clinical findings? With brain anomalies ,metabolic
errors disease and tuberous sclerosis,

Juvenile myoclonus epilepsy
unknown cause early adolescence bilateral myoclonic jerks In the morning after
awakening and can be provoked by sleep deprivation.
. Many patients also experience generalized tonic-clonic seizures, and up to one-third have absence seizures.
The condition is otherwise benign, There is often a family history of epilepsy,
and genetic linkage studies suggest a polygenic cause.

Atonic
Drop attack 1s 6-7 years of old

Lenox – gastaut syndrome
Tonic, clonic, tonic clonic, absence, atonic
1-10 more in 3-5 yearls of old Primary Secondary Hemiplegia,
paraplegia,hydrocephalus, microcephalus in 20%


Status epilepsy