hematology review in myeloid and lymphoid disease veteran general hospital 洪英中
TRANSCRIPT

Hematology Review in Myeloid and Lymphoid Disease
Veteran General Hospital
洪英中
Indication of Allo-HSCT in AML in 1st CR
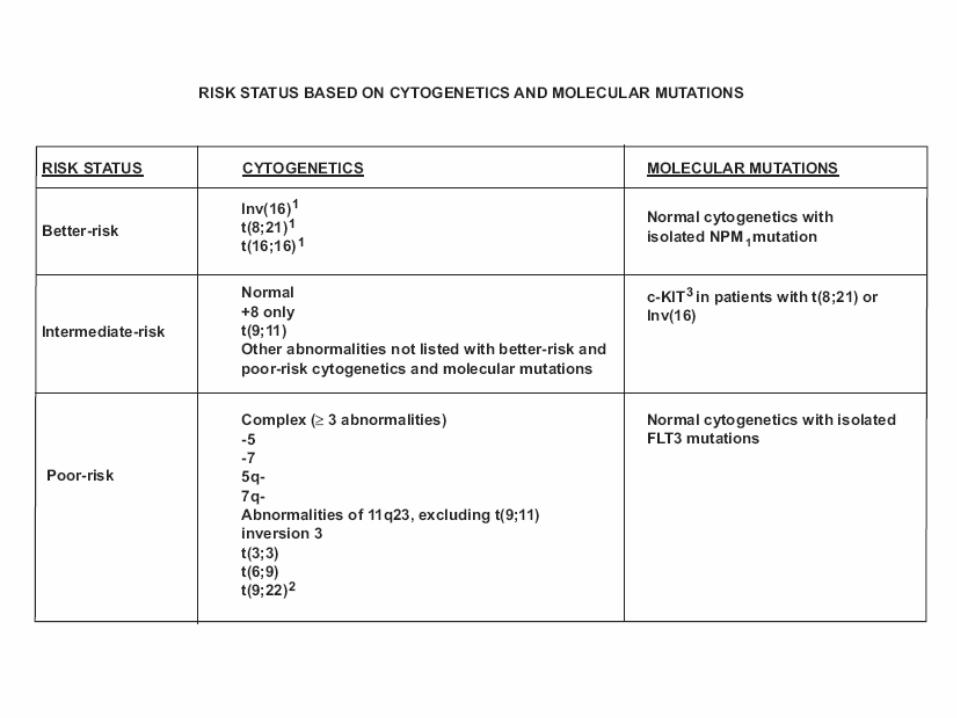
• Intermediate risk: If matching sibling donor available( normal karyotype with NPM1- or FLT3+, +8, +6, -Y )
• High risk( chromosome 5, 7or complex )
Appelbaum, ASCO 2008

Indication of AlloHSCT in ALL
• Matching sibling donor: all risk group adult ALL in 1st CR
• Matching unrelated donor: high risk group t( 4,11 ), complex. Ph+ in 1st CR and all disease beyond 1st CR
Appelbaum, ASCO 2008

Donor Lymphocyte Infusion
• Most promising in CML CP
• Myeloma, Low grade NHL and Hodgkin’s lymphoma: modest effect
• AML and high grade NHL: not satisfied
• ALL: disappointing
Mackinnon, ASCO 2008

Reduced Intensity HSCT
• Graft-versus leukemia/lymphoma
• Lower toxicity of conditioning regimen but higher relapse rate
• Extend to older age people
• Risk of GVHD: similar to conventional dose HSCT but pattern of onset is different
• Onset of aGVHD may be delayed by weeks to months
Antin 2007 Hematology
Reduced Intensity HSCT
• Not a very effective cytoreductive therapy• Performed in reasonable control of the disease• Immune mechanism “GVL”• Tumors could not provide co-stimulatory signals
may be poor targets• Proliferative rapidly may be difficult for the immu
ne system to control• Extensive disease more resistant than minimal d
isease Antin 2007 Hematology
Reduced-Intensity HSCT
• Less aggressive course and lower proliferative rates
• CML, CLL, low grade NHL: excellent rates of disease control
• High grade NHL and Hodgkin lymphoma: wait for further study
• AML/MDS: successful especially in CR status• ALL: much less amenable to GVL and best in
CR status• MM: Good candidate for immunologic control
Antin 2007 Hematology
Graft versus Host Disease
• Multifactorial pathogenesis• Conditioning regimen toxicity that exposes neoa
ntigens• Enhances cytokines release• Augments APC presentation of alloantigen to inc
oming donor T cells• Initiates immunologic storm• Donor T cells activated by alloantigen expand an
d migrate to lymphoid organs and expansion• Cytokine and cytolytic apoptotic injury
Weisdorf, Hematology 2007

Graft versus Host Disease
• Skin, liver, and gut, probably lung• aGVHD 30-50% in sibling donor• Higher incidence in MUD• Dierct organ injury requiring immunosupre
ssive therapy• Secondary risks of infection• Hightened risks of cGVHD• Enhanced antitumor effect
Weisdorf, Hematology 2007
Graft versus Host Disease
• Cytotoxic T cells and inflammatory cytokines produce injury to GVHD target organs through direct cytolytic effect and induction of apoptosis
• Antibody-mediated B-cell responses may be involved in GVHD as well
Weisdorf, Hematology 2007
Presentation of Acute GVHD
• Erythematous skin rash progressing to bullae in most severe form
• Predilection for dorsal surfaces of extremities, malar regions, tops of the ear, back of neck and involvement of palms and soles
• GI tract involvement: nausea, anorexia, vomiting( UGI ); watery, protein-rich, secretory diarrhea that can progress to bloody diarrhea or ileus
• Hepatic involvement: targets the biliary epithelium with cholestasis and Alk-P elevation
• Few case with GI tract or liver involvement only without skin rashes
Weisdorf, Hematology 2007

Variant Presentation of GVHD
• Umbilical cord: less frequent or less severe
• RIC or nomyeloablative: later and slower in evolution of aGVHD but similar in cGVHD
Weisdorf, Hematology 2007

Infection Complication of GVHD
• Immunosuppressive and further immunosuppressive therapy produced lymphopenia
• Disrupted cutaneous and epithelium
• CMV reactivation, invasive fungal infection, PCP, VZV, bacterial infection ( pneumococcal and H. influenzae)
Weisdorf, Hematology 2007

Treatment of aGVHD
• Suppression of T-cell activation, cytokine release and re-establishment of donor-host immunotolerance
• Blunt T-cell activation and facilitate Treg cell expansion
• Initial therapy: 1-2 mg/kg/day prednisone, 30-50% response
• Limited-severity, upper-GI-only GVHD: oral budesonide or beclomethasone with hlow dose prednisone
Weisdorf, Hematology 2007

Treatment of aGVHD
• MMF• Etanercept( TNF-alpha receptor fusion protein )• Denileukin diftitox( Ontak, IL-2 diphtheria toxin )• Pentostatin• Daclizumab( IL-2R alpah receptor Ab )• Infliximab( anti-TNF alpha Ab )• ATG• Sirolimus, alemtzumab, mesenchymal stem cells
Weisdorf, Hematology 2007
Presentation of Chronic GVHD
• Similar with aGVHD: skin, GI and Liver
• Sicca syndrome
• Obstructive broncholitis
• Lichenoid or sclerotic skin change
• Esophageal dysmotility, fasciitis, arthropathy and autoimmune manifestation
Weisdorf, Hematology 2007
Treatment of cGVHD
• Extended duration of immunosuppressive therapy
• Corticosteroid and calcineurin inhibitors
• Newer agent: MMF, sirolimus, pentostatin, extracoporeal photophresis
• Rituximab and thalidomide ?
Weisdorf, Hematology 2007

GVHD
• Major risk factor for cGVHD: preceding aGVHD
• Most important cause of nonrelapse mortality and limiting quality of life
• Associated with protection against malignancy
• The extent and severity do not directly correlate with protection against relapse
Weisdorf, Hematology 2007
Chronic Lymphocytic Leukemia
• 80% CLL with cytogenetic lesions with FISH
• Del 13q: most common
• Trisomy 12
• Del 11q
• Del 17p: poor response to standard C/T, inferior prognosis, lack functional p53, response to Alemtuzumab
Kipps, ASCO 2008
Chronic Lymphocytic Leukemia
• Soluble CD23, thymidine kinase, beta2M, MMP9, IL-8, IL6, CD44: poorer survival or shorter PFS
• Not capable of identifying patients at diagnosis who are at increased risk for PD
Kipps, ASCO 2008

IgHV somatic hypermutation and ZAP-70 in CLL
• Aggressive clinical course in unmutated
• Indolent course in somatic hypermutated
• ZAP-70 express in unmutated
• ZAP-70 enhance the signaling capacity of the surface Ig expressed in CLL derive more stimulation from self and environmental antigens increased proliferation and/or resistance to apoptosis
Kipps, ASCO 2008
MicroRNAs in CLL
• Inhibit gene expression by causing either degradation or blocking the translation of target mRNA
• Regulate gene expression in development and disease
• miRNA gene in del 13q: miR15a and miR16-1• Abnormal, low-level expression of miR15a and
miR16-1 can lead to a disease of CD5-positive B cells in both mice and human
Kipps, ASCO 2008
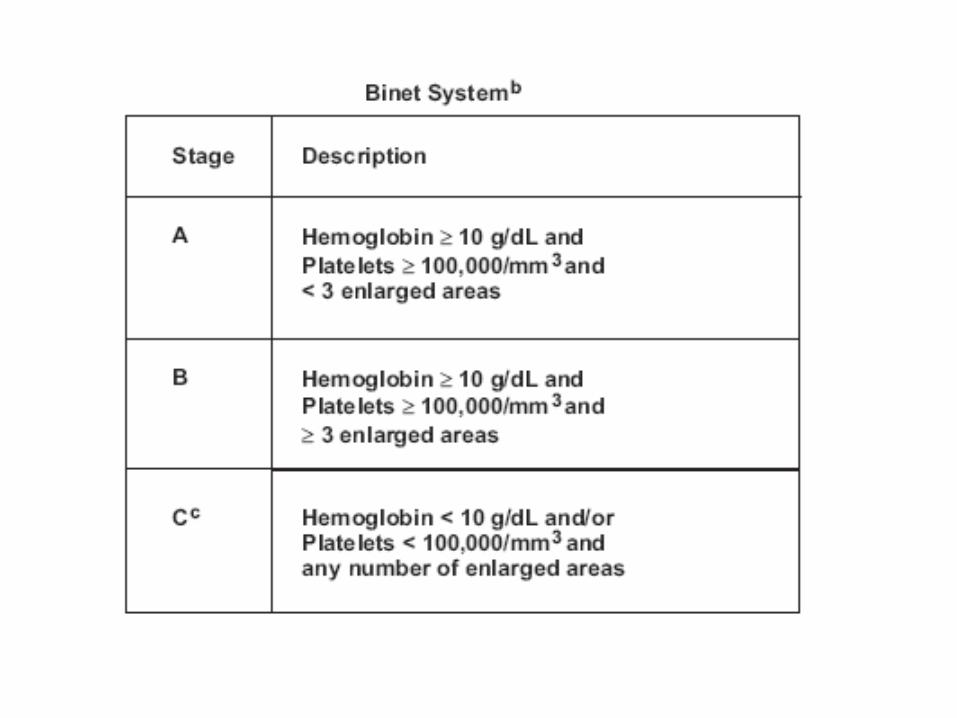
Time to Treatment of CLL
• NCI-working group criteria( revised 2008 )• Should not be treated solely on the basis of prognostic m
arkers except in clinic trial• Monitor without therapy in asymptomatic early stage dise
ase( Rai 0 to 1, Binet A ) unless PD• PD: progressive BM failure worsening anemia and/or thr
ombocytopenia, progressive lymphocytosis with an increase > 50% over 2 months, lymphocyte doubling time< 6 months, massive or progressive LAP, massive or progressive splenomegaly
• Intractable autoimmune anemia or thrombocytopenia
Kipps, ASCO 2008

Time to Treatment of CLL
• Symptomatic disease: unintentional BW loss > 10% in the past 6 months, significant fatigue( ECOG>=2, inability to work or perform usual activities ), fever > 100.5F or 38 C, for 2 weeks or longer without other evidence of infection, night sweats for 1 month or longer
• Absolute lymphocyte count should not be the sole indicator for treatment as hypogammaglobulinemia, monoclonal or olgioclonal paraproteinemia
Kipps, ASCO 2008

HSCT in CLL
• Incurable with standard treatment
• Autologous HSCT: low treatment-related mortality but high relapse
• Myeloablative allo-HSCT: high TRM with few late relapse
Gribben, ASCO 2008
Patient Selection for HSCT
• Young patients with high risk disease
• Unmutated IgHV, ZAP-70, del 17p, p53 abnormality
• Failed to achieve CR, progressed within 12 months after purine analog, relapse within 24 months after response with purine analog or auto-HSCT
Gribben, ASCO 2008

AutoHSCT in CLL
• Unclear role
• Not recommended unless in clinical trial
• Difficult collection of stem cell after purine analog
• Secondary MDS or AML
Gribben, ASCO 2008
AlloHSCT in CLL
• Significant morbidity and mortality from regimen-related toxicity, GVHD, and infection
• Long term disease control in survivors
• Induce durable remission even in refractory disease
Gribben, ASCO 2008

RIC AlloHSCT in CLL
• Potential GVL effect• Decreased relapse with cGVHD• Increased relapse with T cell depletion• DLI generated GVL effect• Reducing short-term morbidity and mortality of al
loHSCT• Allow transplantation in older patient• Alemtuzumab decreased GVHD but delayed pos
t-HSCT immune reconstitution, increased infection risk and impaired GVL
Gribben, ASCO 2008

Treatment of CLL
• Prognostic factors for time to treatment and survival : mutation status of IgHV, ZAP-70, CD38 expression, B2M, soluble CD23, del 17p, 11q by FISH
• Early treatment with chemotherapy for patients without indications or based solely on prognostic factor status should be administered only in the context of a clinical trial
• NCI-WG guideline revised 2008 ( Blood 2008 111: 5446-5456 )
Wierda, ASCO 2008

Treatment of CLL
• Alkylating agent based: chlorambucil, palliative, CR< 10%
• Purine analog based: higher CR and longer remission duration, No different OS
• Purine analog with alkylating agents: higher CR, OR, PFS with FC vs F; more myelosuppression in FC without increase of infection
• No trial confirmed survival advantage • IVIG for recurrent infection with hypogammablob
ulinemiaWierda, ASCO 2008, Kay, Hematology 2007

Treatment of CLL
• Alemtuzumab: single agent activity in Flu refractory disease, sc better tolerated than iv, better response but no survival difference with chlorambucil, only drug with response to p53 abnormality( del17p )
• Rituximab: low CD20 expression in CLL, limited activity
• FCR and PCR: waiting phase III result• No agent or combination have survival advan
tageWierda, ASCO 2008Wierda, ASCO 2008, Kay, Hematology 2007

Treatment of CLL
• 10-15% with autoimmune cytopenia
• Purine analogs may aggravate autoimmune cytopenia
• Immunotherapies and rituximab for AIHA, ITP
• If failed with immunotherapies, use nonpurine analog chemotherapy
• Richter transformation: DLBCL 1%/yearWierda, ASCO 2008, Kay, Hematology 2007
Mantle Cell Lymphoma
• 6% of newly diagnosed NHL
• Worst 5-year OS of any lymphoma subtype in The Non-Hodgkin’s Classification Project
• Median OS 3-4 years historically
• Generally incurable with conventional C/T
• Cyclin D1 overexpression
• T(11,14)(q13, q32)
Kahl, ASCO 2008

Mantle Cell Lymphoma
• CD5+CD23-, CD10-, CD20+• FISH: t(11, 14)• Higher proliferation rat( CDC-2, ASPM, tubulin-al
pha, CENP-F ), K-67: poor prognosis• Median diagnosis age: 63• M/F 4:1• Advanced stage • Extranodal with BM and GI tract involvement• 20-30% leukemic phase with poor outcome• Common splenomegaly
Kahl, ASCO 2008

Treatment of MCL
• Induction therapy followed by some postremission therapy( consolidation or maintenance )
• R-CHOP + AutoHSCT• R-HyperCVAD• New postremission therapy: Y-90 ibritumomab ti
uxetan, maintenance rituximab, bortezomib• New agents for relapse/refractory disease: temsi
rolimus, everolimus, thalidomide, lenalidomide
Kahl, ASCO 2008
Hodgkin Lymphoma
• High cure rate• From extended field irridation and alkylating-bas
ed agents to anthracycline-based with involved filed irridation
• ABVD preserved most fertility of men and women but should care pulmonary toxicity
• PET a powerful functional imaging tool for restaging and response assessment
• Highly predictive at the conclusion of chemotherapy
Horning Hematology 2007

Hodgkin Lymphoma

Hodgkin Lymphoma

Hodgkin Lymphoma
• Second cancers are now the most common cause of mortality among long-term survivors of HL
• Cardiac disease is secondary
• Pulmonary disease
• Endocrine dysfunction
Travis Hematology 2007

Hodgkin Lymphoma
• Breast cancer: higher in R/T patients and decreases in received only alkylating agents( ovary ablation ? )
• Lung cancer: more in R/T
Travis Hematology 2007

Initial Therapy of Multiple Myeloma
• Eligible to transplantation
• All with phase III data
• Thalidomide + Dexamethasone
• Lenalidomide + Dexamethasone
• Bortezomib + Dexamethasone
• Bortezomib + Thalidomide + Dexamethasone
Rajkumar ASCO 2008

Initial Therapy of Multiple Myeloma
• Thalidomide + Dexamethasone• Most used induction regimen in U.S.• More DVT than dexamethasone alone• Lenalidomide + Dexamethasone• Lower stem cell yield with small proportion of pat
ient not collecting adequate amount• Bortezomib + Dexamethasone• Higher CR and VGPR than VAD• Bortezomib + Thalidomide + Dexamethasone• CR + VGPR > TD
Rajkumar ASCO 2008
Initial Therapy of Multiple Myeloma
• Thalidomide and lenalidomide: higher incidence of DVT
• Lenalidomide not suitable for renal failure• VTD most active regimen for renal failure who n
eed a rapid response• In newly diagnosed MM, dexamethasone in com
bination should be low( < 40 mg/week )• High dose dexamethasone is asociated with unf
avorable survival
Rajkumar ASCO 2008
Initial Therapy of Multiple Myeloma
• Not eligible for transplantation• Melphalan/prednosone/thalidomide (MPT)• Bortezomib/melphalan/prednisolone (VMP)• MPT and VMP demonstrate superior respo
nse rate and progression free even overall survival to MP
• VMP overcome adverse cytogenetics but more neurotoxicity
Rajkumar ASCO 2008

Dose of Concomitant Corticosteroid
• ECOG compared dexamethasone in low dose and high dose combined lenalidomide
• Low dose is better than high dose in DVT and infection rate; higher overall survival, lower toxic and disease related death
• Low dose steroid is safer and more effective in newly diagnosed MM
Rajkumar ASCO 2008
Goal of Therapy
• Not response rate or CR rate• Failed to show a consistent association with over
all survival in numerous trials• Most CR is temporary and inevitable relapse• IFM 99-06, Bologna 96, MAG trial, TT II all failed
to showed correlation of CR with overall survival in MM
• For non-transplant candidate, improve overall survival is the goal
• For transplant candidate, safest, least-toxic regimen for pretransplant induction therapy
Rajkumar ASCO 2008
Duration of Therapy
• Fixed duration as tolerated
• MPT < 18 months
• VMP < 12 months
• LD indefinite but stop steroid after 1 year
• VD, VTD, TD restrict to neurotoxicity
Rajkumar ASCO 2008

Role of SCT in MM
• Prolong survival in IFM, English and Italian study• Large U.S., MAG and Spanish study, no survival
benefit• Different design and duration of standard therap
y, age• IFM: benefit of HSCT only in < 60 y/o• Single HDT with SCT with Mel alone( without TB
I )should be considered a standard of care in young patient
Attal Hematology 2007, Fermand ASCO 2008

Role of SCT in MM
• Asymptomatic( smoldering ) MM should not be treated until signs of progression
• Stem cell should be harvested within 3-6 months after therapy initiation
• Timing of autotransplantation has no effect on overall survival
• MAG 90, similar overall survival in patients who received SCT as first line or rescue in parimary resistance to standard Tx or at relapse in responder
Attal Hematology 2007, Fermand ASCO 2008
Role of SCT in MM
• Average time without Sx, Tx, and Tx toxicity favor upfront SCT
• Present recommendation for early SCT is mainly based on quality of life
• Single vs double trials did not provide evidence for a benefit sufficient enough to overcome the risks and constraints of using tandem transplantation
• Double transplantation proposed to patients failing to achieve a VGPR after first SCT, ideally as part of clinical trial
Attal Hematology 2007, Fermand ASCO 2008
Role of SCT in MM
• Thalidomide, bortezomib or lenalidomide including regimens may be preferred to VAD-like regimen as induction therapy
Attal Hematology 2007, Fermand ASCO 2008

Allogeneic SCT in MM
• High TRM with myeloablative regimen
• Reduced transplantation-related toxicity with GVM in reduced intensity conditioning
• Heavily pretreated patients and progressive disease( advanced MM ) do not appear benefit with RIC
• Tandem auto-RIC allogeneic SCT, encouraging in prospective clinical trials
Attal Hematology 2007, Fermand ASCO 2008

Risk-adapted Approach to MM
• Genetic high risk: t(4,14), t(14,16), t(14,20), del 17p by FISH
• Del 13, hypodiploidy by conventional metaphase cytogenetics
• LDH > 2x UNL, B2M> 5.5 mg/L: high risk
Fonseca Hematology 2007, Stewart ASCO 2008
MM Genetics Initiation
• Translocation and ectopic expression of cyclin D genes, MAF family, FGFR3 to IgH switch region on 14q32( 40-50% )
• Tirsomies by odd-numbered chromosomes( hyperdiploidy ) 50-60%
• Up-regulation of cyclin D1, D2 or D3
Stewart ASCO 2008Fonseca Hematology 2007, Stewart ASCO 2008
MM Genetics
• Karyotypic instability induces del 17p13, gene amplification of chromosome 1, monosomy/deletions of 13q14
• A novel progression event of nuclear factor-kappa B pathway in up to 45% of patients
• The primary determinant of patient outcome is the underlying genetics of the tumor
• Therapy should be individualized based on these findings
Stewart ASCO 2008Fonseca Hematology 2007, Stewart ASCO 2008

Clinical Implication for t(11,14)
• Improved or neutral survival for SCT
• Oligosecretory or light chain only myeloma
• CD20 expression
• Lymphoplasmacytic morphology
Stewart ASCO 2008Fonseca Hematology 2007, Stewart ASCO 2008
T(4, 14)
• 15% of MM• Translocation of receptor tyrosine kinase FGFR3• Higher relapse rate and shorter event-free and o
verall survival after SCT• Poor prognosis• High B2M and anemia• Secondary events related to proliferation• Del 13 secondary event of 80% t(4, 14)• Bortezomib at least in part modulate the poor pr
ognosis
Stewart ASCO 2008Fonseca Hematology 2007, Stewart ASCO 2008

T(14,16)
• 5% MM
• Transcription factor c-maf and subsequent cyclin D2 are transcriptionally upregulated
• Associated with shorter survival with SCT or conventional C/T
Stewart ASCO 2008Fonseca Hematology 2007, Stewart ASCO 2008

Hyperdiploidy
• Generally consider favorable
• Live for extend periods after SCT
• Superior PFS and OS
Stewart ASCO 2008Fonseca Hematology 2007, Stewart ASCO 2008

Secondary Genetic Events of Prognostic Relevance
• Del 17p13• Poor prognosis• Generally considered a progression event but
10% at diagnosis• Plasma cell leukemia• CNS involvement• Shorter survival after both conventional C/T and
SCT• Seldom overlap with t(4,14)
Stewart ASCO 2008Fonseca Hematology 2007, Stewart ASCO 2008

Secondary Genetic Events of Prognostic Relevance
• Del 13• Associated with poor prognosis• Detected by FISH:40% of MM, 10-20% by
conventional cytogenetics• Shorter survival and decreased response t
o treatment but much stronger when karyotype used
• Highly associated with other high risk genetic features
Stewart ASCO 2008Fonseca Hematology 2007, Stewart ASCO 2008
Secondary Genetic Events of Prognostic Relevance
• Increased proliferation• Unfavorable• LDH• B2M, marker of plasma cell number, alone
should not be used to define high risk disease in the absence of other poor prognostic factors or presence of renal failure
• Plama cell labeling index
Stewart ASCO 2008Fonseca Hematology 2007, Stewart ASCO 2008

High Risk MM
• T(4,14), t(14,16), del 17p13 by FISH
• Hypodiploidy or del 13 by karyotype
• Plasma cell labeling index >3%
• Above comprise total 25% of MM
• Standard risk with better prognosis, possibly median survival 10 years
Stewart ASCO 2008Fonseca Hematology 2007, Stewart ASCO 2008

Treatment Paradigms Derived From Baseline Genetics
• T(4,14), t(14,16), del 17p very short median event-free survival after conventional induction therapy and SCT
• SCT is no longer of significant value in the high risk MM
• Poor risk features of t(4, 14) and del 13 are partly abrogated by Bortezomib
Stewart ASCO 2008Fonseca Hematology 2007, Stewart ASCO 2008
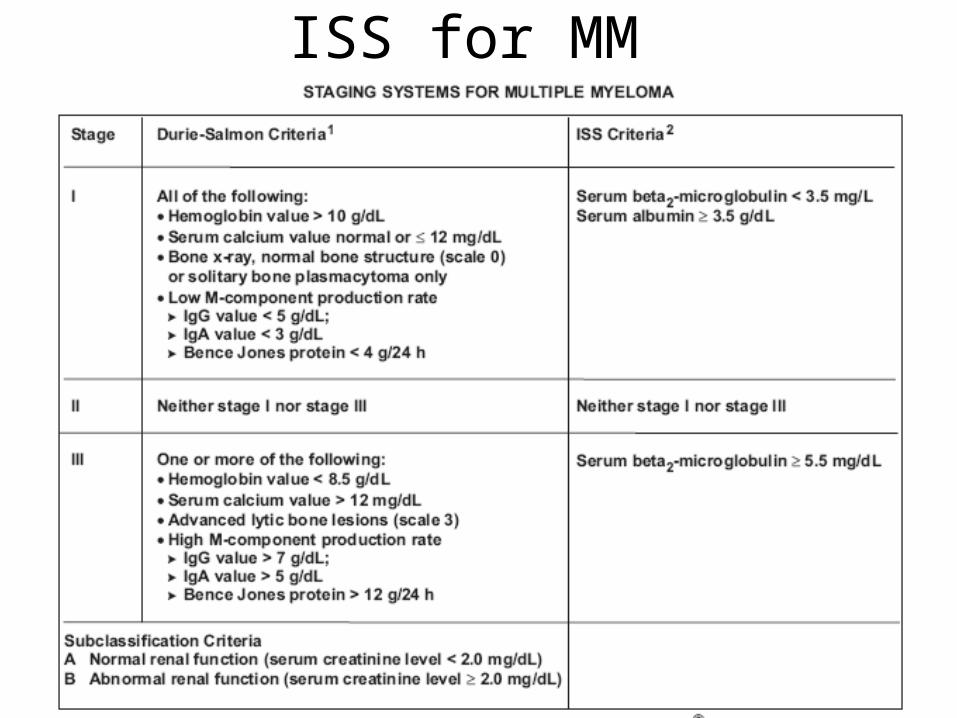
ISS for MM

Myeloma
• Elderly patient may have more indolent disease with low risk features: t(11,14), IgGk, hyperdilopidity, less del 13
• Younger patients more likely have high risk feature: multiple IgH translocation, IgAL, renal failure, more extramedullary MM
Fonseca Hematology 2007