sensorineural hearing loss in adults นพ. อัครรัตน์ ศาสตร์สูง...
TRANSCRIPT
SENSORINEURAL HEARING LOSS IN ADULTS
นพ.อั�ครร�ตน� ศาสตร�ส งเน�นอัาจารย์�ที่��ปร�กษา รศ.สมชาย์ ศร�ร�มโพธิ์��ที่อัง28 ธิ์�นวาคม 2549

28-Dec-2006 2
Sensorineural hearing loss
Introduction
Clinical evaluation• History• Physical examination• Auditory testing• Vestibular testing• Laboratory testing• Radiographic testing
28-Dec-2006 3
Sensorineural hearing loss
Etiology• Development &
Hereditary disorder• Infectious disorder• Pharmacologic
disorder• Trauma• Neurologic disorder• Vascular &
Hematologic disorder
• Immune disorder• Bone disorder• Neoplasms• Endocrine & Metabolic
disorder• Disorder of unknown
etiology
**Sudden Sensorineural hearing loss**

28-Dec-2006 4
Clinical evaluation
History• Unilateral / Bilateral• Chronicity• Tinnitus / Vertigo• Otalgia / Otorrhea• Headache• Eye symptoms
• Underlying disease• Ototoxic drugs• Hx of trauma• Noise exposure• Family Hx

28-Dec-2006 5
Clinical evaluation
Physical examination• Weber / Rinne test• Otoscopy• Cranial nerve• Stigmata of associated disease• Generally no abnormality**
28-Dec-2006 6
Clinical evaluation
Auditory testing• Conventional audiometry• Tympanometry• Acoustic reflex threshold• Auditory brainstem response• Electrocochleography• Otoacoustic emission
28-Dec-2006 7
Clinical evaluation
Laboratory testing• Fluorescent treponemal
antibody absorption test : FTA-ABS
• Microhemagglutination test for Treponema pallidum : MHA-TP
• Venereal disease research laboratory : VDRL
• Routine hematologic studies• Routine metabolic studies
Vestibular testing• Adjunct in selected patients
Radiographic testing• MRI with Gadolinium
Retrocochlear hearing loss?• Computed tomography
Labyrinthine abnormality?
28-Dec-2006 8
Etiology
• Development & Hereditary disorder• Infectious disorder• Pharmacologic disorder• Trauma• Neurologic disorder• Vascular & Hematologic disorder• Immune disorder• Bone disorder• Neoplasms• Disorder of unknown etiology
28-Dec-2006 9
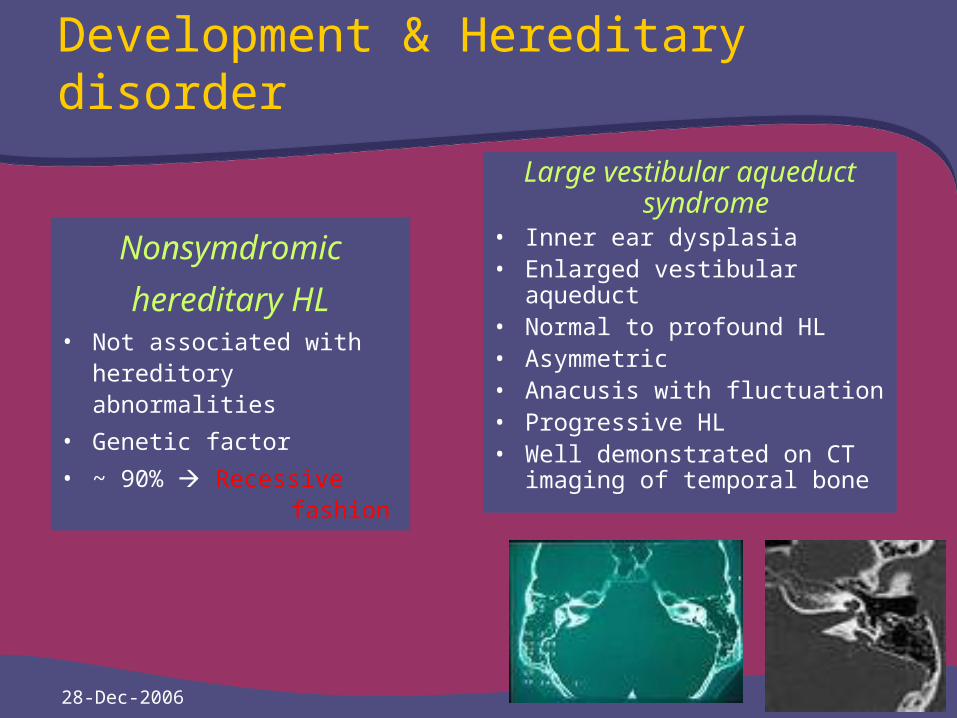
Development & Hereditary disorder
Nonsymdromic
hereditary HL• Not associated with
hereditory abnormalities
• Genetic factor
• ~ 90% Recessive fashion
Large vestibular aqueduct syndrome
• Inner ear dysplasia• Enlarged vestibular aqueduct • Normal to profound HL• Asymmetric• Anacusis with fluctuation• Progressive HL• Well demonstrated on CT
imaging of temporal bone

28-Dec-2006 10
Development & Hereditary disorder
Waardenburg syndrome• Autosomal-dominant1) Dystopia canthrum (Lateral
displacement of the media canthi)
2) Broad nasal root3) Confluence of the
medialportions of the eyebrows
4) Partial or total heterochromia iridis
5) A white forelock6) Sensorinearal hearing loss• Vary hearing loss• Unilateral / Bilateral
28-Dec-2006 11
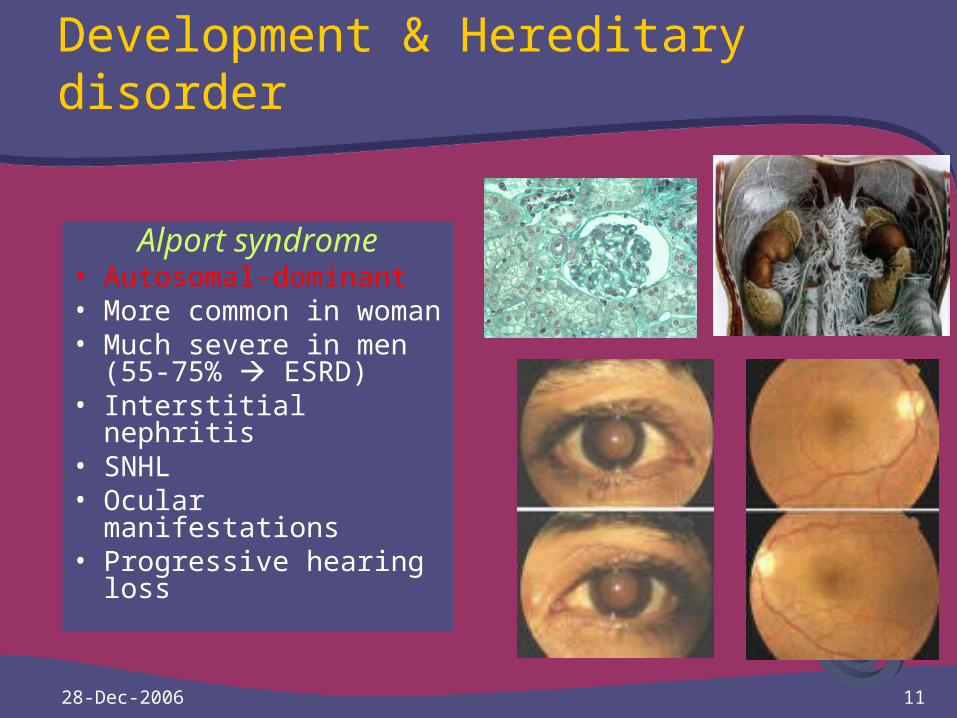
Development & Hereditary disorder
Alport syndrome• Autosomal-dominant• More common in
woman• Much severe in men
(55-75% ESRD)• Interstitial nephritis• SNHL• Ocular manifestations• Progressive hearing
loss

28-Dec-2006 12
Development & Hereditary disorder
Usher syndrome• Autosomal-recessive• Retinitis pigmentosa &
SNHL• Type I ~85% Profound HL Absent vestibular
response Retinitis pigmentosa
Stereocilia are arranged in three tiers atop a hair cell.Tip links connecting shorter stereocilia to their taller neighbors.
28-Dec-2006 13
Etiology
• Development & Hereditary disorder• Infectious disorder• Pharmacologic disorder• Trauma• Neurologic disorder• Vascular & Hematologic disorder• Immune disorder• Bone disorder• Neoplasms• Disorder of unknown etiology

28-Dec-2006 14
Infectious disorder
LabyrinthitisSerous labyrinthitis
• Abnormal process within the labyrinth
• Endolymphatic hydrops• Hearing loss and vestibular
dysfunction • Permanent or transient• Sudden onset of
sensorineural hearing loss and acute vertigo
• Viral labyrinthitis is common
Suppurative labyrinthitis • Bacterial invasion of the inner
ear• Profound hearing loss and
acute vertigo • Caused by a fistula between
the middle ear and the labyrinth
• Alternatively, the route of invasion can be meningogenic
• Most common etiology of deafness associated with meningitis
28-Dec-2006 15
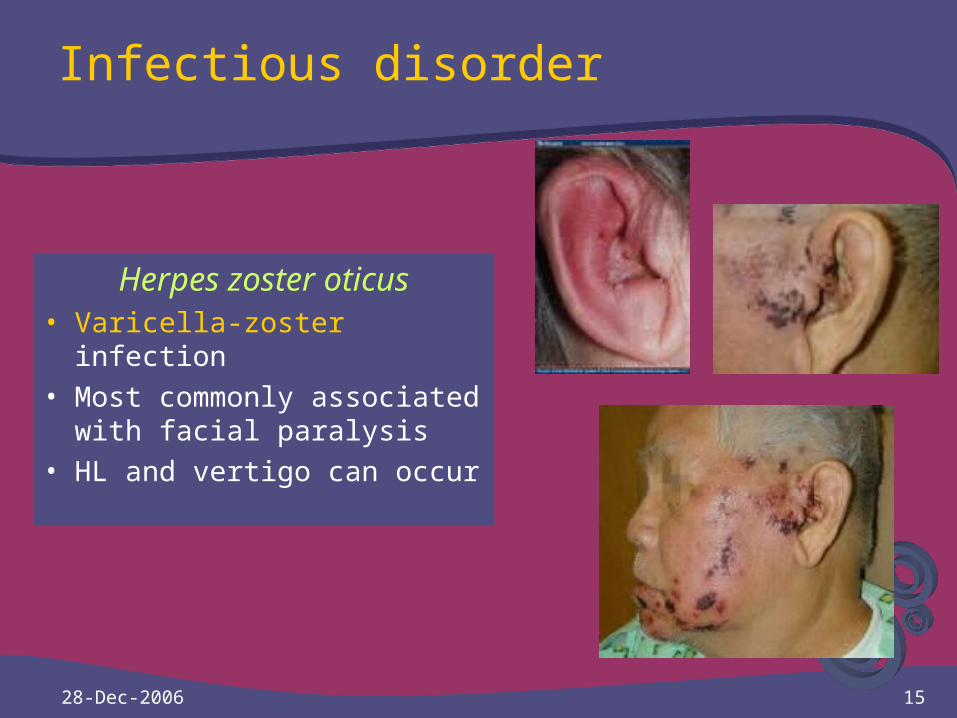
Infectious disorder
Herpes zoster oticus• Varicella-zoster infection• Most commonly associated
with facial paralysis • HL and vertigo can occur
28-Dec-2006 16
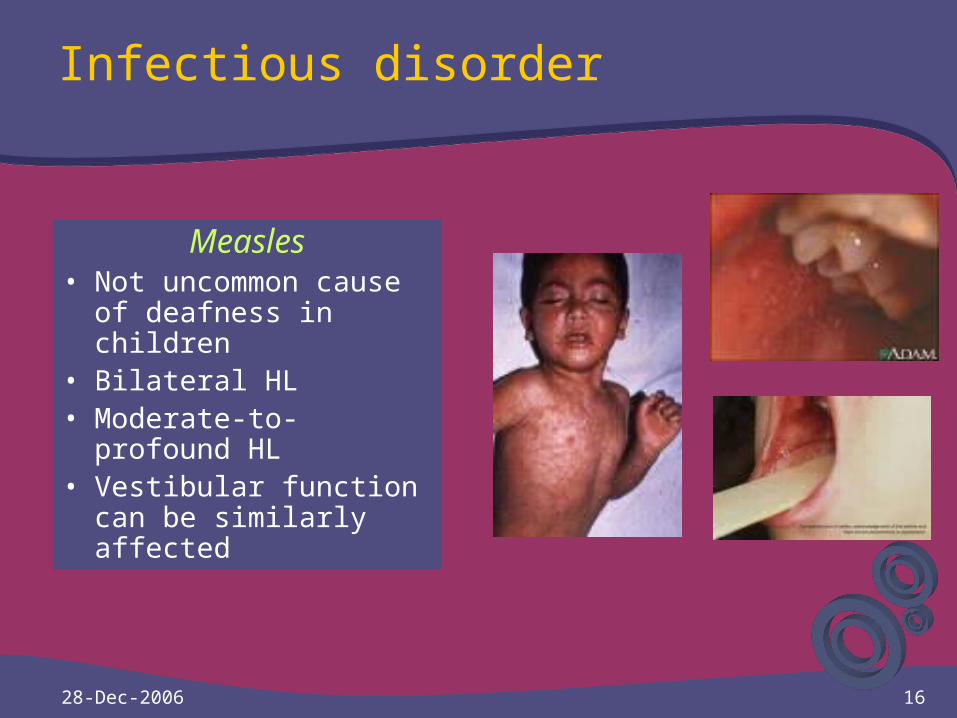
Infectious disorder
Measles• Not uncommon cause
of deafness in children• Bilateral HL• Moderate-to-profound
HL• Vestibular function can
be similarly affected
28-Dec-2006 17
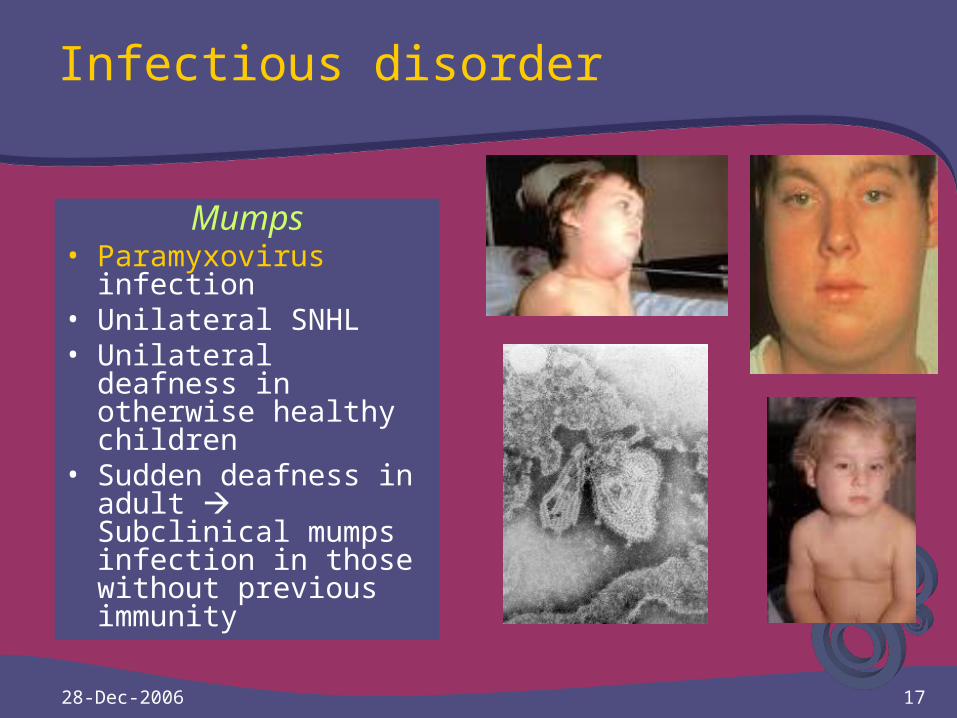
Infectious disorder
Mumps• Paramyxovirus
infection • Unilateral SNHL • Unilateral deafness in
otherwise healthy children
• Sudden deafness in adult Subclinical mumps infection in those without previous immunity
28-Dec-2006 18
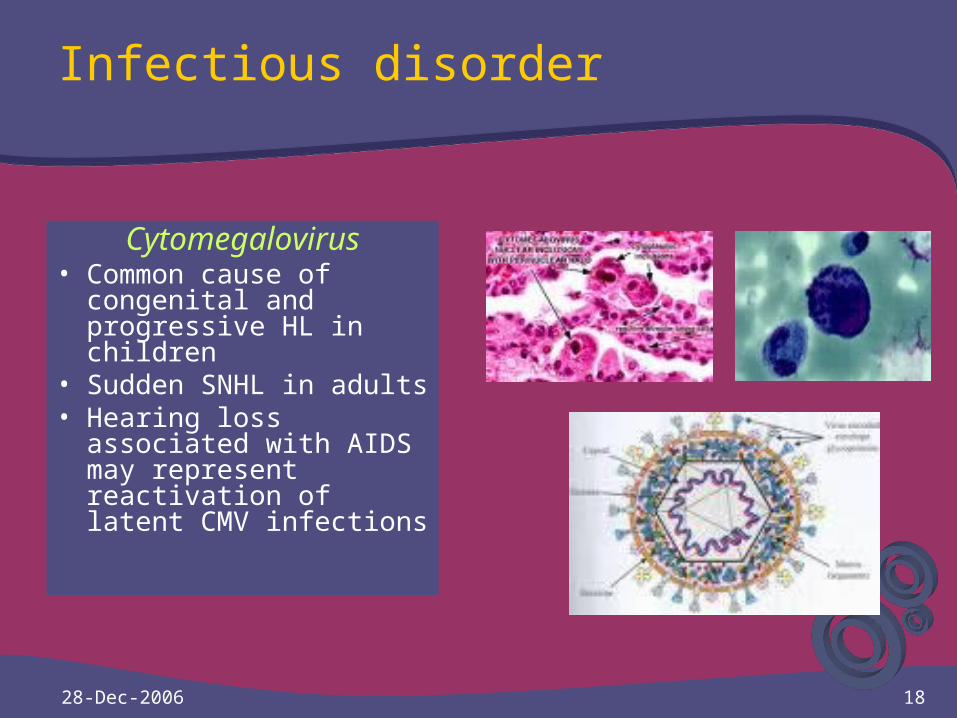
Infectious disorder
Cytomegalovirus• Common cause of
congenital and progressive HL in children
• Sudden SNHL in adults • Hearing loss
associated with AIDS may represent reactivation of latent CMV infections
28-Dec-2006 19
Infectious disorder
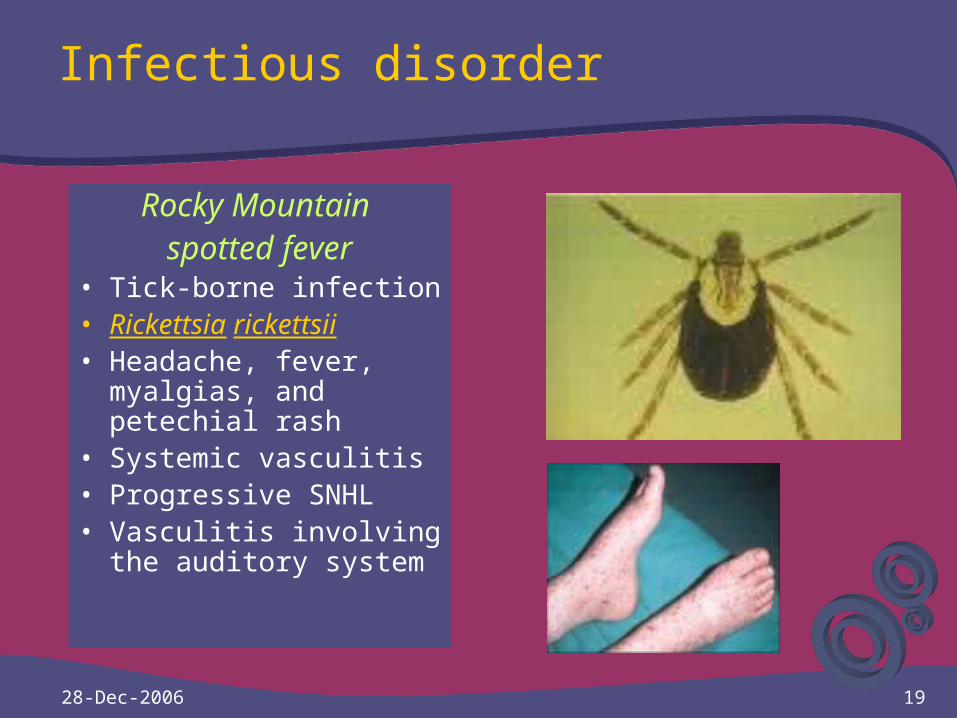
Rocky Mountain spotted fever
• Tick-borne infection • Rickettsia rickettsii• Headache, fever,
myalgias, and petechial rash
• Systemic vasculitis• Progressive SNHL• Vasculitis involving the
auditory system

28-Dec-2006 20
Infectious disorder
Syphilis• Congenital or acquired syphilis • 80% Symptomatic neurosyphilis• HL in syphilis Meningolabyrinthitis • Syphilitic HL Indistinguishable from
Ménière’s disease• Hennebert’s sign (a positive fistula
test without middle ear disease) • Tullio’s phenomenon (vertigo or
nystagmus on exposure to high-intensity sound)

28-Dec-2006 21
Infectious disorder
Lyme disease • Tick-borne infection • Borrelia burgdorferi• Facial paralysis• Possible etiology of
SNHL in endemic areas

28-Dec-2006 22
Etiology
• Development & Hereditary disorder• Infectious disorder• Pharmacologic disorder• Trauma• Neurologic disorder• Vascular & Hematologic disorder• Immune disorder• Bone disorder• Neoplasms• Disorder of unknown etiology

28-Dec-2006 23
Pharmacologic disorder
Aminoglycosides Streptomycin, Kanamycin,
Neomycin, Amikacin, Gentamicin, Tobramycin, and Netilmycin
Death of the hair cell Different patterns of ototoxicity
with different aminoglycosides Unilateral or asymmetric Reversibility of the HL Risk factors
(1) presence of renal disease (2) longer duration of therapy (3) increased serum levels
(4) advanced age (5) concomitant administration of
other ototoxic drugs
Ototopical preparations Neomycin, Gentamicin, and
Tobramycin-containing Cochlear or vestibular
ototoxicity Avoid the use of
aminoglycoside-containing topical preparations in uninflamed ears with tympanic membrane perforations
Ingredients of ototopical preparations also have ototoxic potential
Polymyxin B, Propylene glycol, Acetic acid, Antifungal agents

28-Dec-2006 24
Pharmacologic disorder
Loop diuretics Effect by blocking sodium
and water reabsorption in the proximal loop of Henle
Reversible SNHL Bilateral and symmetric Sudden in onset Alteration of endolymphatic
ion concentration and endocochlear potential
Risk factors (1) Renal failure (2) Rapid infusion (3) Aminoglycoside
administration
Antimalarials Quinine Tinnitus, SNHL, &
Visual disturbances Chincinonism Tinnitus,
headache, nausea, and disturbed vision
Quinine appears to be primarily on hearing and usually is transient
Permanent hearing loss may occur with large doses or in sensitive patients
28-Dec-2006 25
Pharmacologic disorder
Salicylates Aspirin Tinnitus and
reversible SNHL HL Dose-dependent Moderate-to-severe range SNHL, loss of otoacoustic
emissions, reduced cochlear action potentials
Alteration of the “tips” of auditory nerve fiber tuning curves
Alteration in turgidity and motility of outer hair cells
Nonsteroidal antiinflammatory drugs
Naproxen, Ketoralac & Piroxicam
Ototoxicity resulting from use of NSAIDs is rare
Only reversible physiologic changes, without major morphologic changes

28-Dec-2006 26
Pharmacologic disorder
Vancomycin Almost received Vancomycin
& loop diuretics or aminoglycosides
Ototoxicity Intravenously Permanent or transient SNHL Excreted by the kidney Renal failure Vancomycin
half-life Increase ototoxicity Itself ototoxic Unclear
Erythromycin Uncommon Partially Intravenously Reversible on
discontinuation No reports
- Newer macrolide - Clarithromycin
- Azithromycin
28-Dec-2006 27
Pharmacologic disorder
Nitrogen mustards Antineoplastic agents Mechlorethamine has
Serious ototoxicity Limited use Severe toxic Shrinkage of the organ of
Corti Loss of inner and outer hair
cells
Cisplatinum Cell-cycle nonspecific
cancer chemotherapeutic agent
Dose-limiting SNHL Adults (25% to 86%) Children (84% to 100%) Bilateral / Irreversible Tinnitus or vertigo HL Dose-related Progressive outer hair
cell loss Inner hair cells, neural
structures and the stria vascularis are affected

28-Dec-2006 28
Pharmacologic disorder
Vincristine and vinblastine
The vinca alkaloids Potent neurotoxicity Peripheral neuropathy Cranial neuropathies,
ataxia, and hearing loss Loss of hair cells and
primary auditory neurons
Eflornithine Drug treatment of
trypanosomiasis Some Pneumocystis
carinii pneumonia, Cryptosporidiosis, Leishmaniasis, and Malaria
Cause major and dose-related SNHL

28-Dec-2006 29
Pharmacologic disorder
Deferoxamine Iron-chelating agent Auditory and visual
neurotoxicity Particularly with larger
doses in younger patients
The SNHL is reversible in some patients when the dosage is reduced
Lipid-lowering drugs Wallerian-like
degeneration High doses of HMG-CoA
reductase inhibitors Optic& vestibulocochlear
nerve degeneration No clinically significant
effect on vision or hearing
28-Dec-2006 30
Etiology
• Development & Hereditary disorder• Infectious disorder• Pharmacologic disorder• Trauma• Neurologic disorder• Vascular & Hematologic disorder• Immune disorder• Bone disorder• Neoplasms• Disorder of unknown etiology

28-Dec-2006 31
Trauma
Head injury Blunt head injury alone
Concussive injury of the labyrinth
Labyrinthine injury SNHL Temporal bone fracture
Labyrinthine concussion Longitudinal fractures
Similar to acoustic trauma
Limited to the high F
Worse at 4 kilohertz
Transverse fractures
Complete loss of auditory & vestibular function
Penetrating injuries
Subluxation ofthe stapes into the vestibule
Profound SNHL
28-Dec-2006 32
Trauma
Noise-induced HL & Acoustic trauma
First published in the 1930s Common occupationally-
induced disabilities Common in industry Caused by excessive noise
exposure Temporary SNHL that
recovers over the next 24 to 48 hours
High intensity & repeated Permanent
Outer hair cell Most effect
More damage in - High-frequency sound - Continuous sound - Pure tones
Symmetric & Bilateral HL Limited to 3 kHz, 4 kHz,
and 6 kHz Greatest loss 4 kHz Progress rapidly in first 10
to 15 years of exposure
28-Dec-2006 33
Trauma
Noise-induced HL & Acoustic trauma
Common patterns Flat & downsloping losses
Acoustic trauma Unilateral or asymmetric
OSHA does not allow unprotected exposures greater than 90 dBA based on an 8 hour/day time weighted average (TWA)
Variability Age, gender, race, and coexisting vascular disease
No known way to predict susceptibility to NIHL
Protection Earplugs or earmuffs
Many hazardous noise exposures are not occupational in origin
28-Dec-2006 34
Trauma
Barotrauma Unequalized pressure
differentials between the middle and external ears
Occurs during flying or underwater diving
Pain, hyperemia and possible perforation of the tympanic membrane
Edema and ecchymosis of the middle ear mucosa
Conductive HL may result
Perilymphatic fistula Pathologic communication
between the perilymphatic space of the inner ear and the middle ear
Congenital or acquired Occur at either the round or
oval windows
28-Dec-2006 35
Perilymphatic fistula
Congenital Occur in the stapes
footplate with labyrinthine anomalies
Such as Mondini dysplasia Communicate with the
subarachnoid space and result in cerebrospinal fluid leak and possible meningitis
Profound hearing loss
Acquired Result of
- Barotrauma
- Direct trauma of temporal
- Indirect trauma of temporal
- Complication of stapedectomy Sudden SNHL and vertigo after a
head injury, barotrauma, or heavy lifting or straining
May be spontaneously Diagnosis
Middle ear exploration
28-Dec-2006 36
Trauma
Irradiation Conventional
fractionated irradiation of the temporal bone
Fractionated irradiation Limited extent to treat vestibular schwannoma
Difficult to determine because of the limited data available
Stereotactic irradiation (“radiosurgery”) for vestibular schwannoma
This modality Risk of SNHL High as with microsurgical removal
28-Dec-2006 37
Etiology
• Development & Hereditary disorder• Infectious disorder• Pharmacologic disorder• Trauma• Neurologic disorder• Vascular & Hematologic disorder• Immune disorder• Bone disorder• Neoplasms• Disorder of unknown etiology
28-Dec-2006 38
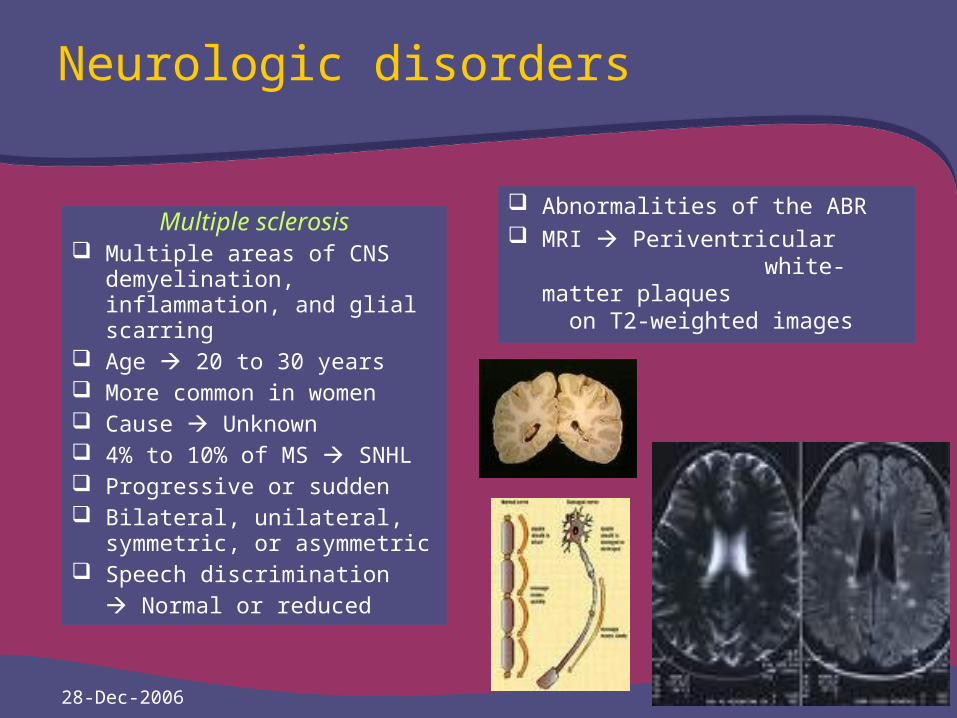
Neurologic disorders
Multiple sclerosis Multiple areas of CNS
demyelination, inflammation, and glial scarring
Age 20 to 30 years More common in women Cause Unknown 4% to 10% of MS SNHL Progressive or sudden Bilateral, unilateral, symmetric,
or asymmetric Speech discrimination
Normal or reduced
Abnormalities of the ABR MRI Periventricular
white-matter plaques on T2-weighted images
28-Dec-2006 39
Neurologic disorders
Benign intracranial hypertension
Pseudotumor cerebri Increased intracranial pressure Without evidence of mass
lesion, obstructive hydrocephalus, intracranial infection, or hypertensive encephalopathy
Headache and visual blurring Pulsatile tinnitus SNHL and vertigo More in young, obese women
SNHL Fluctuating, low-F Unilateral or bilateral Vertigo and aural fullness Diagnosis
Papilledema CSF pressure > 200 mmH2O ABR abnormalities
Management - Weight loss- Acetazolamide- Furosemide- Lumbar-peritoneal shunting
28-Dec-2006 40
Etiology
• Development & Hereditary disorder• Infectious disorder• Pharmacologic disorder• Trauma• Neurologic disorder• Vascular & Hematologic disorder• Immune disorder• Bone disorder• Neoplasms• Disorder of unknown etiology
28-Dec-2006 41
Vascular and hematologic disorders
Migraine• Headache and visual aura• Basilar migraine
Vertigo, SNHL Tinnitus, aural fullness Distortion & recruitment
• 46% Bilateral, low-F-SNHL• Fluctuated HL • Similarity, between basilar
migraine and Ménière’s Dz.• Drugs in basilar migraine
No systematic study
Vertebrobasilar arterial occlusion
• Brainstem syndromes• Anterior inferior cerebellar
artery (AICA) • Occlusion of AICA SNHL• Thrombosis or embolism • Area infarcted Inferior pons• Acute AICA infarction• Acute vertigo with N/V• Facial paralysis, SNHL• Tinnitus, gaze paralysis• Loss of pain and temperature
sensation on the face• Ipsilateral Horner’s syndrome
28-Dec-2006 42
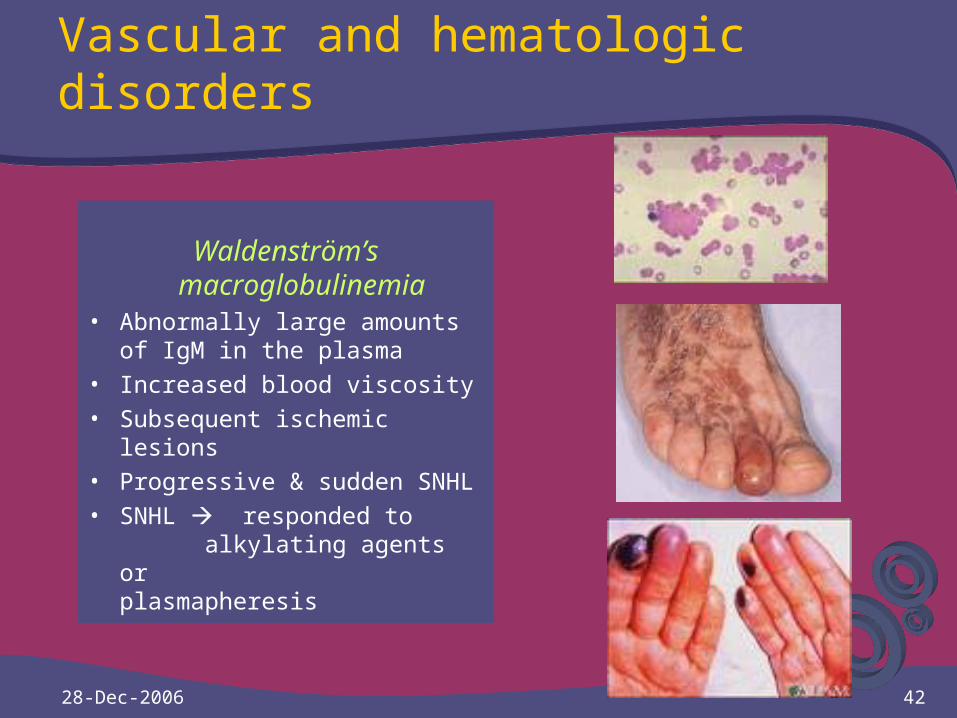
Vascular and hematologic disorders
Waldenström’s macroglobulinemia
• Abnormally large amounts of IgM in the plasma
• Increased blood viscosity • Subsequent ischemic lesions• Progressive & sudden SNHL• SNHL responded to
alkylating agents or plasmapheresis
28-Dec-2006 43
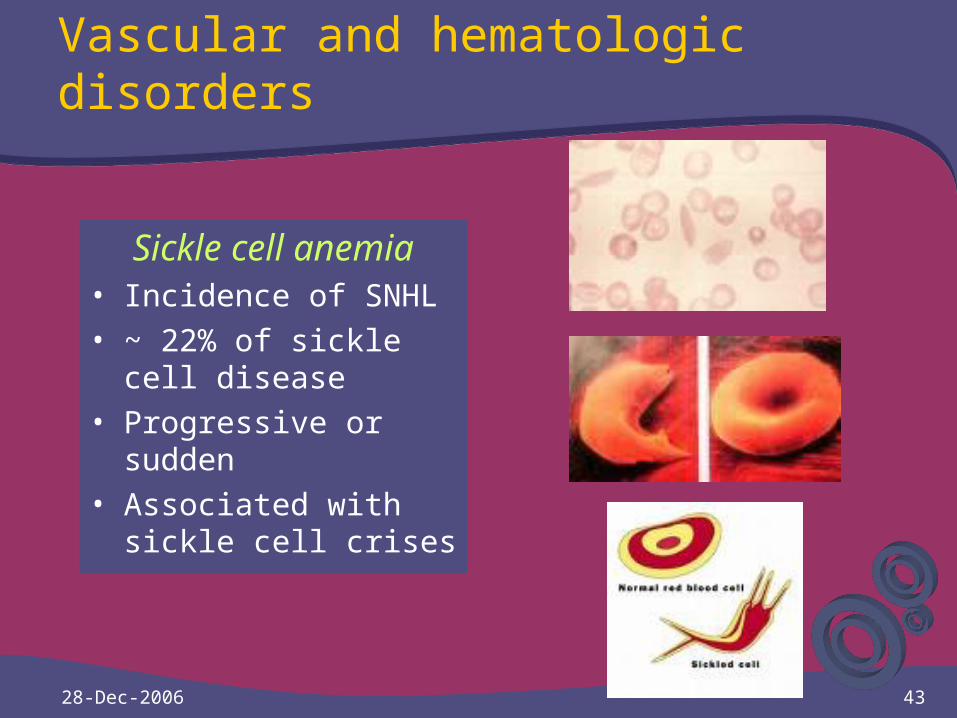
Vascular and hematologic disorders
Sickle cell anemia• Incidence of SNHL• ~ 22% of sickle cell
disease• Progressive or sudden• Associated with sickle
cell crises
28-Dec-2006 44
Vascular and hematologic disorders
Leukemias & Lymphomas• SNHL
Leukemic infiltrates
Inner ear hemorrhage
Vascular occlusion
Labyrinthine ischemia
28-Dec-2006 45
Etiology
• Development & Hereditary disorder• Infectious disorder• Pharmacologic disorder• Trauma• Neurologic disorder• Vascular & Hematologic disorder• Immune disorder• Bone disorder• Neoplasms• Disorder of unknown etiology

28-Dec-2006 46
Immune disorders
Cogan’s syndromeo Attacks of acute non-
syphilitic interstitial keratitis o Auditory and vestibular
dysfunctiono Unilateral or bilateral SNHLo Severe vertigo, nausea,
vomiting, and tinnituso Progresses to a profound
loss over monthso Ophthalmologic findings o If treated SNHL is
responsiveo Aggressive treatment with
steroids
28-Dec-2006 47
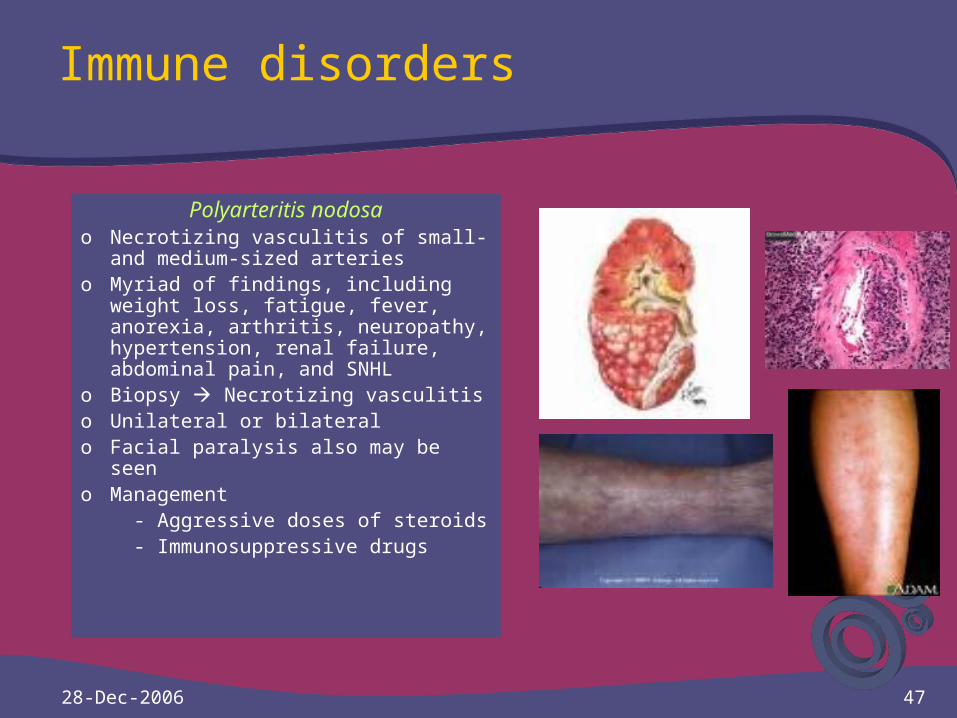
Immune disorders
Polyarteritis nodosao Necrotizing vasculitis of small- and
medium-sized arterieso Myriad of findings, including weight
loss, fatigue, fever, anorexia, arthritis, neuropathy, hypertension, renal failure, abdominal pain, and SNHL
o Biopsy Necrotizing vasculitiso Unilateral or bilateral o Facial paralysis also may be seeno Management
- Aggressive doses of steroids - Immunosuppressive drugs
28-Dec-2006 48
Immune disorders
Relapsing polychondritiso An inflammatory reaction in
multiple cartilageso The auricles 1st affectedo Arthritis and eye findings o HL Conductive
Sensorineural
Mixed HL
o SNHL Sudden or progressive
o May be associated with vestibular disturbances
o Rx
Steroids
Immunosuppresive
Dapsone
28-Dec-2006 49
Immune disorders
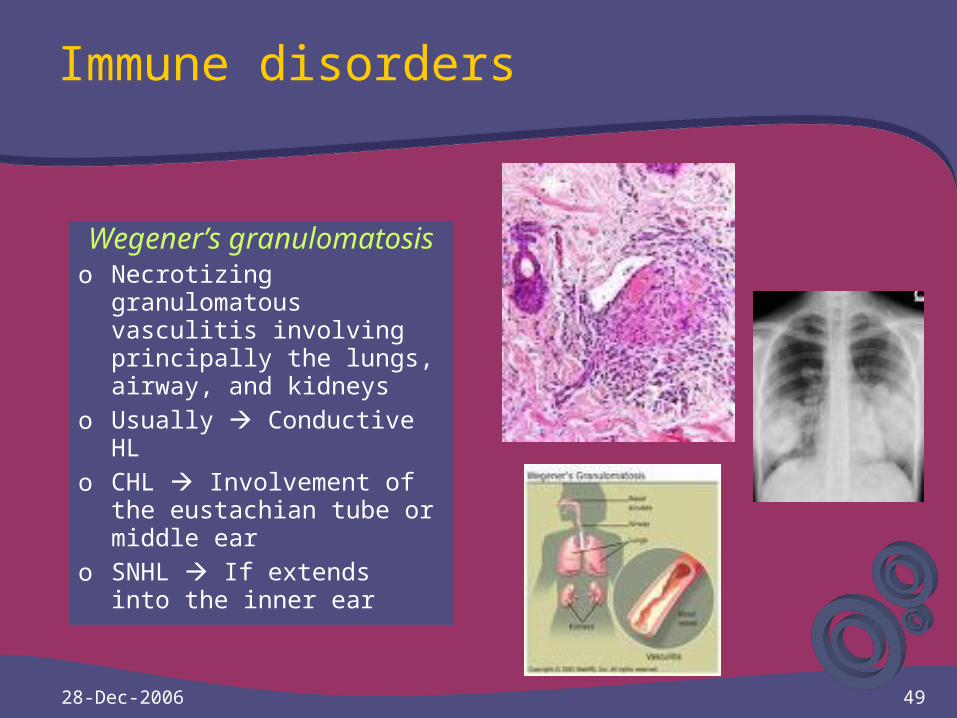
Wegener’s granulomatosis
o Necrotizing granulomatous vasculitis involving principally the lungs, airway, and kidneys
o Usually Conductive HLo CHL Involvement of the
eustachian tube or middle ear
o SNHL If extends into the inner ear
28-Dec-2006 50
Immune disorders
Primary autoimmune inner ear disease
o McCabe Bilateral SNHL responsive to immunosuppressive drugs
o Sudden or progressive HLo Involves both earso Associated with vestibular
symptoms o Strongly mimic Ménière’s
disease
o Humoral autoimmunity Abnormal
o Responsiveness of the HL to steroids or cytotoxic drugs The hallmark
o Used Methotrexate Reduce the need for continued high-dose steroids

28-Dec-2006 51
Etiology
• Development & Hereditary disorder• Infectious disorder• Pharmacologic disorder• Trauma• Neurologic disorder• Vascular & Hematologic disorder• Immune disorder• Bone disorder• Neoplasms• Disorder of unknown etiology
28-Dec-2006 52
Bone disorders
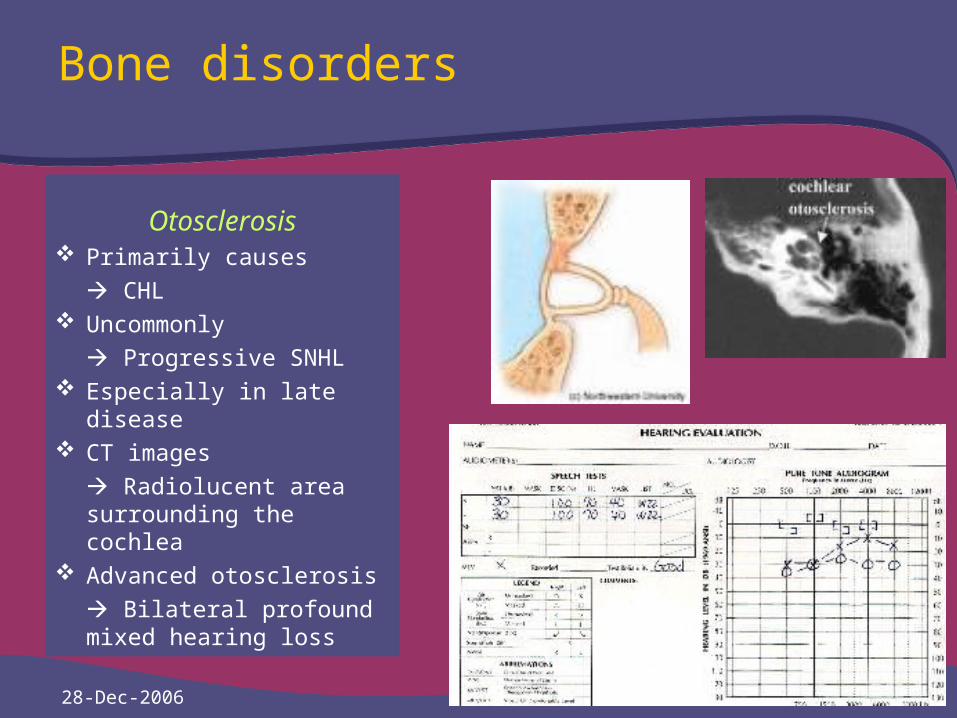
Otosclerosis Primarily causes
CHL Uncommonly
Progressive SNHL Especially in late disease CT images
Radiolucent area surrounding the cochlea
Advanced otosclerosis
Bilateral profound mixed hearing loss
28-Dec-2006 53
Bone disorders
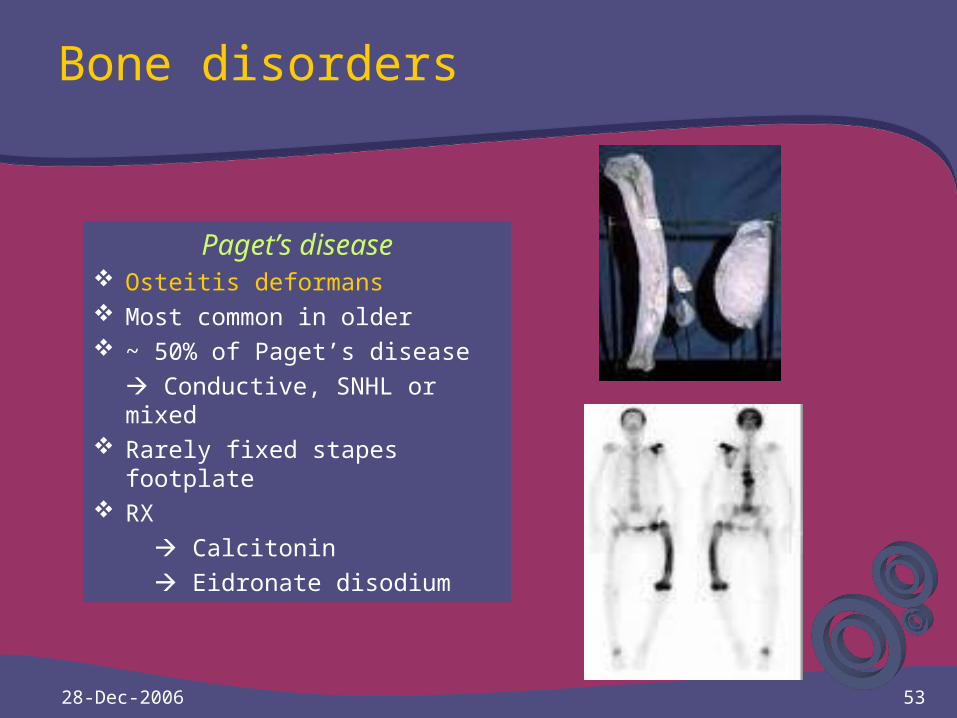
Paget’s disease Osteitis deformans Most common in older ~ 50% of Paget’s disease
Conductive, SNHL or mixed Rarely fixed stapes footplate RX
Calcitonin
Eidronate disodium
28-Dec-2006 54
Etiology
• Development & Hereditary disorder• Infectious disorder• Pharmacologic disorder• Trauma• Neurologic disorder• Vascular & Hematologic disorder• Immune disorder• Bone disorder• Neoplasms• Disorder of unknown etiology
28-Dec-2006 55
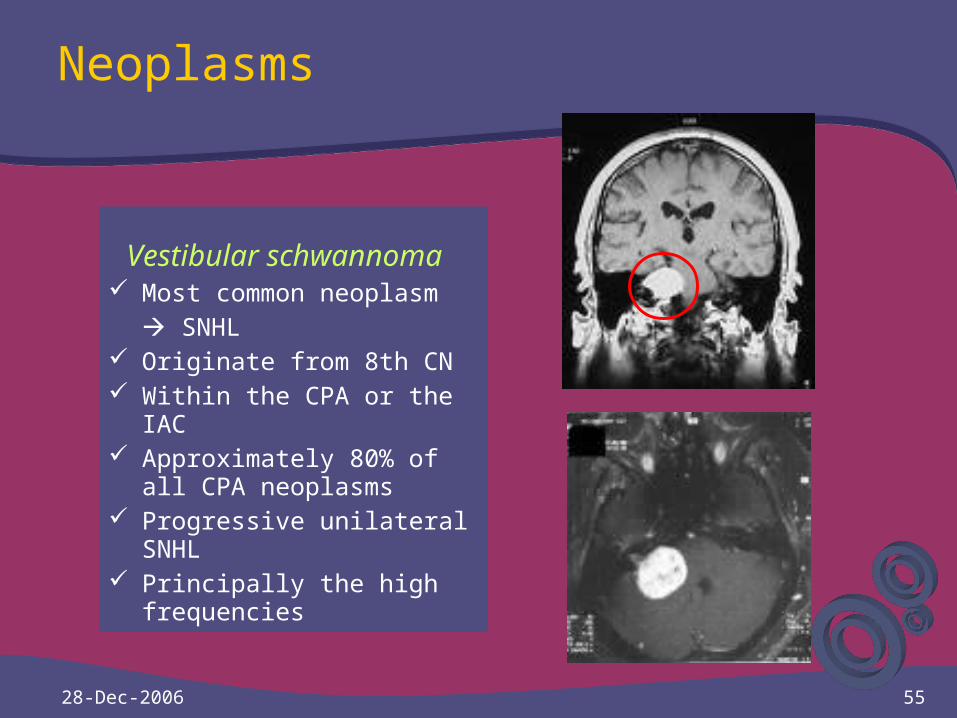
Neoplasms
Vestibular schwannoma Most common neoplasm
SNHL Originate from 8th CN Within the CPA or the IAC Approximately 80% of all
CPA neoplasms Progressive unilateral
SNHL Principally the high
frequencies
28-Dec-2006 56
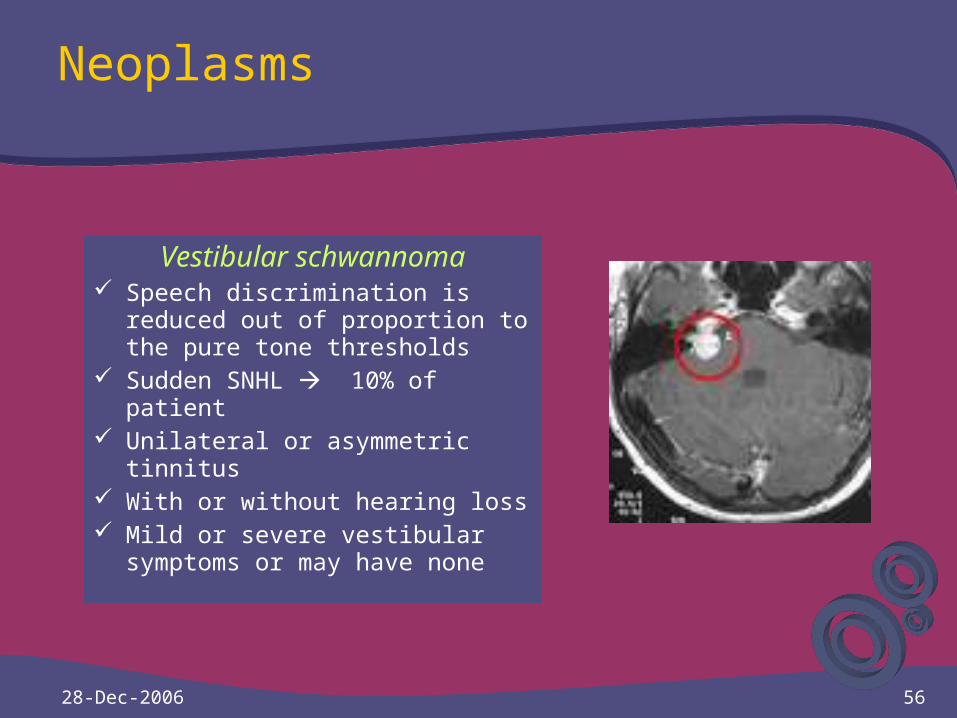
Neoplasms
Vestibular schwannoma Speech discrimination is reduced
out of proportion to the pure tone thresholds
Sudden SNHL 10% of patient Unilateral or asymmetric tinnitus With or without hearing loss Mild or severe vestibular
symptoms or may have none
28-Dec-2006 58
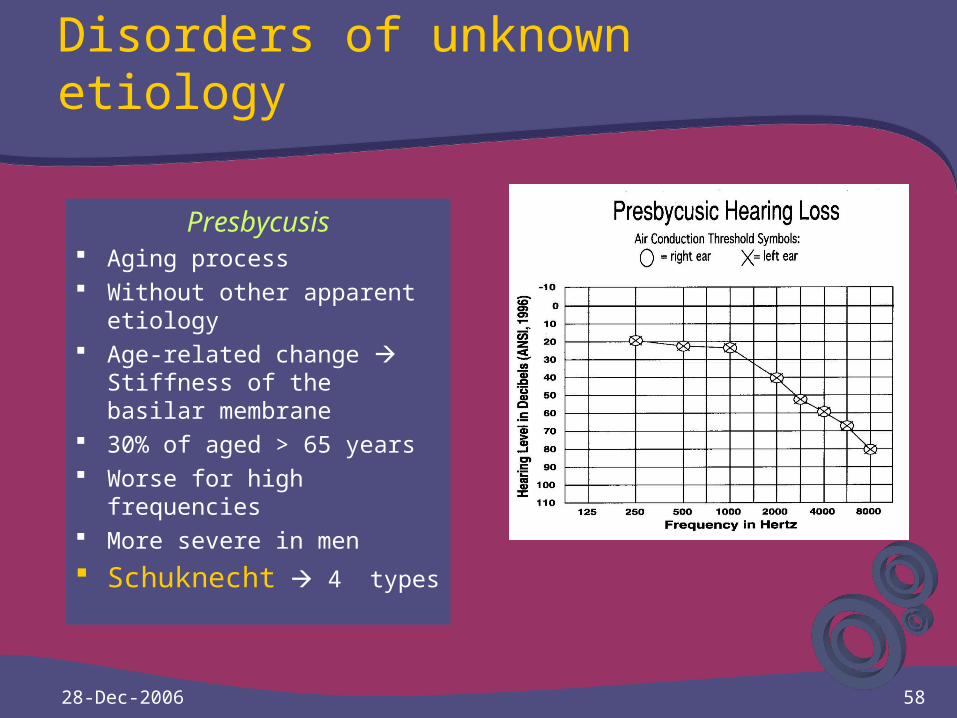
Disorders of unknown etiology
Presbycusis Aging process Without other apparent
etiology Age-related change
Stiffness of the basilar membrane
30% of aged > 65 years Worse for high frequencies More severe in men
Schuknecht 4 types

28-Dec-2006 59
Presbycusis
Neural presbycusis - Loss of auditory nerve fibers
- Reduced speech discrimination out of proportion to their pure tone thresholds
Cochlear presbycusis - Mechanical CHL
Sensory presbycusis - Progressively hair cells loss - Steeply sloping HF-SNHL
Strial presbycusis - Atrophy of the stria vascularis - Flat audiograms
28-Dec-2006 60
Disorders of unknown etiology
Ménière’s disease Fluctuant SNHL Tinnitus, episodic vertigo,
and aural fullness Progresses, gradually or
quickly HL Tinnitus “Buzzing” or
“Roaring” Aural fullness Typically
fluctuates
Vertigo Several hours After attacks Fatigued for
24 hours or more Profound loss is rare Low F Commonly Bilateral in 30% to 50% Endolymphatic spaces
dilatation of the inner ear
28-Dec-2006 61
Disorders of unknown etiology
Ménière’s disease Vestibular destructive
therapy No effective No therapy Effective in HL Medical therapy
- Sodium-restricted diet - Diuretic administration
Lack of an objective diagnostic test
Idiopathic endolymphatic hydrops
Other pathologic endolymphatic hydrops processes - Syphilis - Temporal bone trauma - Serous labyrinthitis - Stapedectomy - Autoimmune disease

28-Dec-2006 62
Thank YouThank You