strategies to reduce readmissions, sepsis, and health-care...
TRANSCRIPT

12/5/2016
1
Strategies to Reduce Readmissions, Sepsis, and Health-Care Associated Infections
DavidRenfro,MS,RNNE‐BCKellyFarnam,BSN,RNGloriaMartinez,MS,RN,NEA‐BCDeniseRenfro,MS,RNJenniferEllman,MSN,RN,NE‐BC,CEN
C10This presenter has nothing to disclose
Tuesday,December61:30pm
#IHIFORUM CoordinatedbyEmilyStallings
Session ObjectivesP2
#IHIFORUM
• Describe proven strategies for leveraging nurses to improve rates of readmission, sepsis, and healthcare‐associated infections
• Understand the potential impact of direct‐care nurse leadership
• Identify focus areas at your facility in which nurse‐driven improvement could have a positive impact on clinical outcomes

12/5/2016
2
Session GuideP3
• Four short presentations about improvement work led by direct-care staff.
1. Readmission Reduction (Project RED)2. Transition Education3. Reducing Sepsis Mortality4. Reducing Healthcare-Associated Infections
• Time for questions between each presentation
• Lessons learned and advice to take with you

12/5/2016
3
VA Palo Alto Health Care SystemP5
• Enrolled Veterans 84,432• Veterans treated in FY 15: 67,640 • Outpatient visits: 829,990• Inpatient Admissions: 6,144• Catchment area: 13,500 Square miles• Total Budget: $930 million• Total FTE: +4,000• Academic Affiliation
Characteristics for Nurse-Driven ImprovementsP6
• Patient‐safety‐ or satisfaction‐focused
• Evidence‐based practice change
• Includes a range of environments
• Willingness to lead at the direct‐care level
• Strong leadership commitment, support and coaching
• Change evident in patient outcomes
• Commitment to developing confident, competent, credible nursing staff

12/5/2016
4
Leveraging the Expertise of Direct-Care Staff to Reduce
Hospital Readmissions
P7
Kelly Farnam, BSN, RNWillie Payton Jr., MHSA
Nicole Briones
Identifying a ProblemP8
• Lack of standardized discharge process • Readmission rates rising• 2011 rate of 13%• Medication discrepancy rate of 38%

12/5/2016
5
Choosing a StrategyP9
• Strategy options: BOOST, STAAR, TCM, Project RED
• Existing case management structure• Nurse engagement for planning
The RED Model: 12 ElementsP10
1. Educate the patient throughout the hospital stay
2. Make post‐discharge appointments prior to discharge with patient input
3. Discuss pending tests and studies and how to learn results
4. Organize post‐discharge services5. Medication reconciliation6. Reconcile the discharge plan with
national guidelines and clinical pathways
7. Review what to do in an emergency and who to contact
8. Ensure discharge summary follows patient to next care location
9. Utilize teach‐back to assess patient understanding of instructions
10.Give the patient a written discharge plan
11.Call the patient after discharge to answer any questions and follow up on any pending items
12.Ascertain the need for language assistance
1.Educate the patient throughout the hospital stay
7. Review what to do in an emergency and who to contact

12/5/2016
6
Empowering Direct Care StaffP11
Standardize Discharge Across the Board• Multidisciplinary collaboration• Focus on the whole transition of care• Empower bedside nurse to ensure a safe discharge• Discharge education documents are created by
nurse to eliminate education gaps
P12

12/5/2016
7
A Strategy for SuccessP13
Direct actions for bedside nurses• Voice concerns about readmission before dischargeTransition Coordinators• Access patient data for those readmitted within 30 days
• Facilitate communication between inpatient and outpatient providers
• Attend daily multidisciplinary meeting to identify patients with key diagnosis, and assess need for enrollment in Project RED
A Strategy for SuccessP14
ICU Discharge• All Intensive Care Unit patients being discharged
directly home have their care coordination assessed by Project RED Transition Coordinators
Discharge Appointment Coordinator• Works with each individual patient prior to
discharge to schedule follow up appointments at the most convenient time and date for the patient
After Hospital Care Plan (AHCP)

12/5/2016
8
OutcomesP15
• Decreased readmissions by >30%• Established reliable nursing discharge process• Increased nursing communication with
interdisciplinary teams• Created a culture focusing on process, not people• Decreased medication discrepancies
P16
0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
20%
Jan
Feb
Mar
April
May Jun
Jul
Aug
Sep
Oct
Nov
Dec Jan
Feb
Mar
Apr
May Jun
Jul
Aug
Sep
Oct
Nov
Dec Jan
Feb
Mar
Apr
May Jun
Jul
Aug
Sep
2014 2015 2016
30 Day Readmission Rates
30 Day Rate
Baseline (12.8%)
Goal
Linear (30 Day Rate)
12/5/2016
9
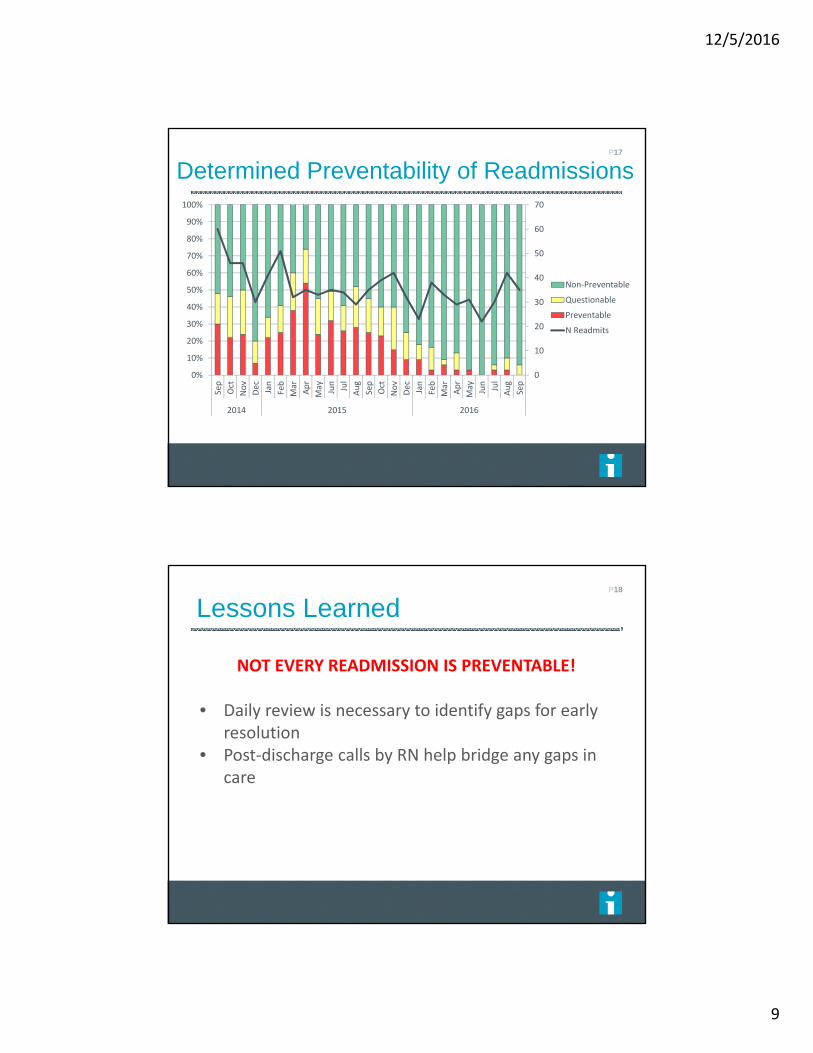
Determined Preventability of ReadmissionsP17
0
10
20
30
40
50
60
70
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Sep
Oct
Nov
Dec Jan
Feb
Mar
Apr
May Jun
Jul
Aug
Sep
Oct
Nov
Dec Jan
Feb
Mar
Apr
May Jun
Jul
Aug
Sep
2014 2015 2016
Non‐Preventable
Questionable
Preventable
N Readmits
Lessons LearnedP18
NOT EVERY READMISSION IS PREVENTABLE!
• Daily review is necessary to identify gaps for early resolution
• Post‐discharge calls by RN help bridge any gaps in care

12/5/2016
10
Questions?
P19
Improving Education Through Engaging Direct-Care Staff
P20
Gloria Martinez, MS, RN, NEA‐BCKelly Farnam, BSN, RN
Nicole Briones

12/5/2016
11
State of EducationP21
Call to Action: • Only 40% of patients at discharge could state why
they had been admitted• Discharge Instructions confusing and hard to readSolutions Implemented:• Began discharge education process at admission• Implemented a new teaching tool (After Hospital
Care Plan)• Educated the patient utilizing teach back• Have direct‐care nurses lead and coach the process• Created teach back videos to train staff
Video- The BadP22
#IHIFORUM

12/5/2016
12
P23
Video- The Good
Maintaining the MomentumP24
• Teach back as the only way to educate patients• Taking ownership of the teaching process• Teach back champions on each unit to address unit
specific challenges (OR/PACU‐ how to make teach back relevant)
• Ensure all nurses get teach back education as part of their new hire orientation
• Incorporate teach back as a part of nursing documentation

12/5/2016
13
Educational MaterialsP25
#IHIFORUM
P26

12/5/2016
14
Get Feedback from Patients!P27
• Veteran and family friendly information. No medical jargon
• Allows for sharing of pertinent information with family/caregivers
• Has a notes section for patient or family to write questions to ask PCP
Lessons Learned and OutcomesP28
Lessons Learned• Staff development• Investment• Actively listen• Patients learn better when you engage themOutcomes• Peer accountability• Active partner in care• Patients love the care plan!

12/5/2016
15
Questions?
P29
Sepsis Initiative: Developing Nurses as Leaders and Evidence-Based
Practitioners
P30
Denise Renfro, MS, RN

12/5/2016
16
GoalP31
Develop emerging nurse leaders with the ability to be:1. EBP Practitioners2. Change Agents3. Facilitators of learning4. Consultants and initiative champions5. Collaborators across disciplines6. Confident communicators and presenters
While also improving a facility clinical practice
StrategyP32
Evidence‐Based Practice Fellowship Program• Rigorous application process• Investment of 72 hours (9 learning sessions)• Theory and Application• Development of Leadership Skills
Regional goal to reduce sepsis mortality rate by 10%

12/5/2016
17
Staff-Driven ImprovementsP33
Johns Hopkins Model
Sepsis Guidelines
Pilot tests of change
Screening Tool
Order Set Simulation
OutcomesP34
• Leadership development of direct‐care nurses• Skill development and confidence• Peer accountability and recognition
Decreased sepsis mortality by 12% and saved 14 lives!
0
5
10
15
20
25
2009 2010 2011 2012 2013 2014 2015
VA Palo Alto Sepsis Mortality
My Rate
Regional Rate
Linear (My Rate)

12/5/2016
18
Lessons LearnedP35
• Team stability
• Just‐in‐time coaching
• Interdisciplinary champions
• Evolving learner milestones
Special ThanksP36
EBP Fellows:
Kristina Castro, MSN, RN, CNL
Kristen Valente, BSN, RN
Desiree Picazo, BSN, RN
Leisa Ann Bunte, BSN, RN
Support From:
Jane He, MD
Roberta Oka, PhD, Nurse Scientist
Jennifer Ellman, MSN, RN

12/5/2016
19
Questions?
P37
Developing Nurse-Led Teams
to Reduce Hospital-Acquired Infections
P38
Jennifer Ellman, MSN, RN, NE‐BC, CEN

12/5/2016
20
Call to ActionP39
C. difficile
MRSA
CLABSI
Plan: Partner for ExcellenceP40

12/5/2016
21
Develop Direct Care StaffP41
• Align units under common goal
• Support psychological safety
• Create a culture to “improve from within”
Strategy: Leverage the WorkforceP42
• Discover common challenges
• Appreciate uniqueness of specific practice environments
• Develop an inclusive plan
• Collaborate to remove barriers

12/5/2016
22
Create a Roadmap
Assemble the “right” team
Observe current state
Review best practices
Develop strategy and plan
Accountability
P43
Root Cause AnalysisP44
Why were we not meeting our goals?
• Education and Training
• Documentation and Communication
• Variability in Practice

12/5/2016
23
Develop a Mindset for Continuous Improvement P45
OutcomeP46
0.0
5.0
10.0
15.0
20.0
25.0
FY14Qtr1 FY14Qtr2 FY14QTR3 FY14QTR4 FY15QTR1 FY15QTR2 FY15QTR3 FY15QTR4 FY16QTR1 FY16QTR2 FY16QTR3
Rate per 10,000 bed days of care
Quarter
Hospital Onset Healthcare Facility Associated (HO‐HCFA) CDI Rate
Acute Care Units
CDI rate VAPAHCS Acute Care rate goal Linear (CDI rate)

12/5/2016
24
OutcomeP47
0.0
1.0
2.0
3.0
FY14Q1 FY14Q2 FY14Q3 FY14Q4 FY15Q1 FY15Q2 FY15Q3 FY15Q4 FY16Q1 FY16Q2 FY16Q3
Infection rate per
1,000 urinary catheter days
Quarter
Catheter Associated Urinary Tract Infections (CAUTI)Acute Care Units
CAUTI rate VAPAHCS Rate Goal (<=1.25)
Lessons LearnedP48
Challenges
• Hardwire the process
• Resistance
• High‐risk population
Keys to success:
• Focus on the patient
• Leverage direct‐care staff and decentralize improvement teams
• Use evidence‐based practice

12/5/2016
25
Questions?
P49
Lessons LearnedP50
• Developing direct‐care leadership is an investment
• Focus only on processes, and not on people
• Develop coaching relationships with your direct‐care staff
• Encourage your nurses to showcase their capabilities
• Provide the time and resources to allow PDCA to work
• Listen to staff and to patients
• Empower and appreciate

12/5/2016
26
Translating To Your FacilityP51
• Take the time to plan
• Build a strong team and include opinion leaders, direct‐care staff and patients
• Set ground rules for communication
• Assign champions and accountability
Translating To Your Facility
• “Chunk and check”
• Daily management
• Don’t take no for an answer. Challenge the status quo
• Bust the myth
• Take risks and celebrate wins!
P52

12/5/2016
27
Final Questions
P53