2016 renewal presentation universal …macademyk8.com/adobeforms/school reports/umc 10,1,2016.pdfa...
TRANSCRIPT
UNIVERSAL MANAGEMENT COMPANY2016 Renewal Presentation
TABLE OF CONTENTS1 HEALTH CARE REFORM
2 FINANCIAL ANALYSIS & MEDICAL PLAN OPTIONS
3 DENTAL & VISION PLAN OPTIONS
4 LIFE AND DISABILITY OPTIONS
5 SPECIALTY BENEFIT PLAN OPTIONS
SMART BENEFIT SOLUTIONS

CARRIERS CONTACTED
MEDICAL – BCBSM
• BCN: Presented• Priority Health: Presented• AHL / HAP: Presented
DENTAL – NEW LINE
• Delta Dental: Presented• Guardian: Presented• Principal Financial: Presented• Ameritas: Presented
VISION – NEW LINE
• Heritage: Presented• Ameritas: Presented• Guardian: Presented• Principal: Presented
LIFE & DISABILITY – Reliance Standard
• Guardian: Presented• Mutual of Omaha: Presented• Sun Life: Presented• MMA / MetLife: Presented• The Hartford: Requested• UNUM: Presented
Detailed below is a categorical listing of carriers that were contacted regarding assumingcoverage for Universal Management Company. Noted below are the responses that were
received per carrier.
SMART BENEFIT SOLUTIONS
3

HEALTH CARE REFORM
SMART BENEFIT SOLUTIONS
4
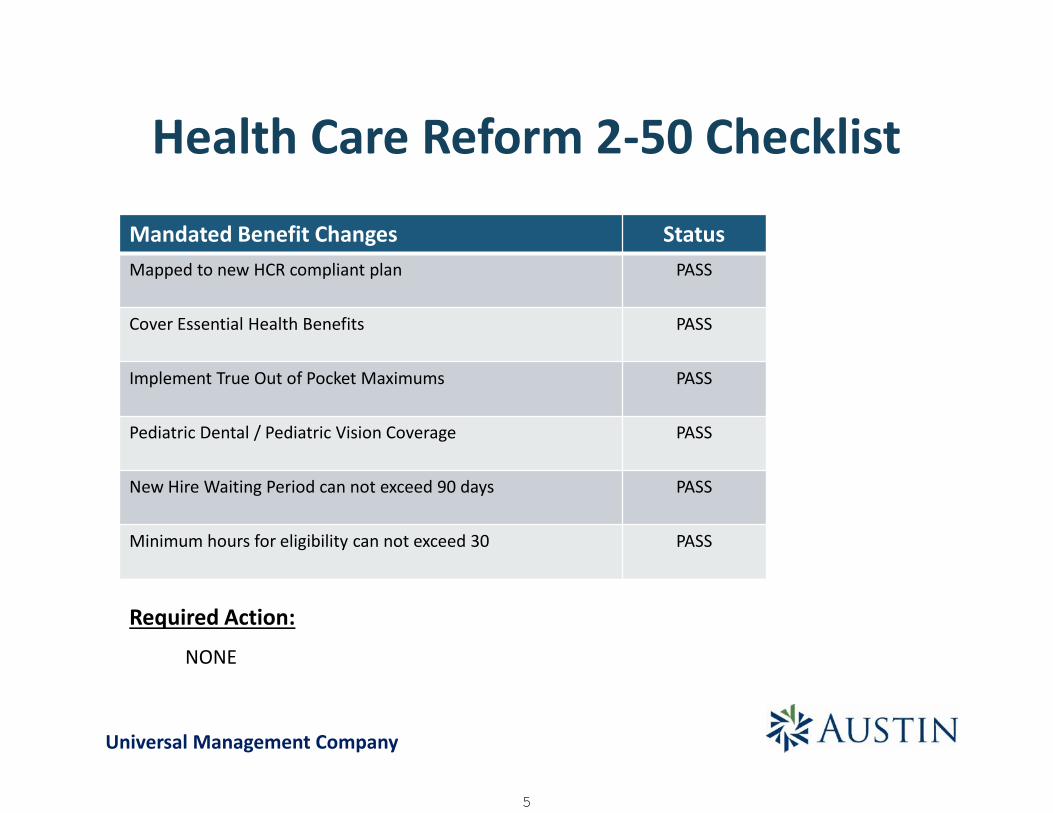
Health Care Reform 2-50 Checklist
Mandated Benefit Changes StatusMapped to new HCR compliant plan PASS
Cover Essential Health Benefits PASS
Implement True Out of Pocket Maximums PASS
Pediatric Dental / Pediatric Vision Coverage PASS
New Hire Waiting Period can not exceed 90 days PASS
Minimum hours for eligibility can not exceed 30 PASS
Required Action:
NONE
Universal Management Company
5

2016 ACA/Regulatory Renewal Checklist For Small Groups (1-50)
The Affordable Care Act (ACA) has made a number of significant changes to group health plans since the law was enacted in 2010.
This checklist provides a brief overview of the ACA’s key reforms that are in effect or will take effect in 2016. Employers should review this checklist to help confirm they are ready to comply with the ACA’s current reforms. Please contact Austin Benefits Group if you would like more information about any of the following.
Plan Design Changes
ACA Requirement Action Items
Grandfathered Plan Status
A grandfathered plan is one that was in existence when the ACA was enacted on March 23, 2010. If you make certain changes to your plan that go beyond permitted guidelines, your plan is no longer grandfathered.
□ If you have a grandfathered plan, determine whether it will maintain its grandfathered status for the 2016 plan year.
□ If your plan will lose its grandfathered status for 2016, confirm that the plan has all of the additional patient rights and benefits required by the ACA for non-grandfathered plans.
Health FSA Contributions
Effective for plan years beginning on or after Jan. 1, 2013, the ACA placed an annual limit on an employee’s pre-tax salary reduction contributions to a health flexible spending account (FSA). The health FSA limit was $2,550 in 2015 and will remain the same in 2016.
□ If you had a health FSA in 2015, there are no changes.
□ If you start a health FSA in 2016, the annual limit will be $2,550.
Essential Health Benefits (EHBs)
ACA Requirement Action Items
EHBs and Pediatric Dental and Vision Certain health benefits that are deemed “essential” must be covered. The minimum package of items and services that must be covered by these plans generally defined by each state’s EHB benchmark plan. Grandfathered plans don’t have to cover EHBs but, if they do, they can’t set any annual or life dollar limits on those EHBs. ACA requires that each employee and dependent (enrolled in an applicable medical plan) must have pediatric dental and vision EHB coverage. The law requires pediatric dental and vision coverage as an EHB for non-grandfathered fully insured small group and non-grandfathered individual plans with plan/policy years beginning on or after Jan. 1, 2014.
□ Ensure your health care plan covers EHBs
□ Ensure you offer pediatric dental and vision EHB coverage (excluding grandfathered plans)
6

2016 ACA/Regulatory Renewal Checklist For Small Groups (1-50)
Out-of-pocket Maximums for EHBs
For plan years beginning on or after Jan. 1, 2016, member cost sharing for in-network EHBs, across all service providers, cannot exceed the OOPM set by ACA. The OOPM cannot exceed $6,850 for individual coverage, and $13,700 for family coverage in the 2016 plan year. Generally, member cost sharing that is considered part of the OOPM includes:
Deductibles for in-network EHBs Coinsurance for in-network EHBs Copayments for in-network EHBs Any other expenditure required by, or on behalf
of, an enrollee for in-network EHBs including out-of-network emergency services and member liability on reference-based pricing (RBP) claims
□ Confirm that the OOPM for your 2015 plan with EHBs does not exceed $6,850 for individual, or $13,700 for family coverage
Minimum Value Coverage
ACA Requirement Action Items
A plan provides minimum value if the plan’s share of total allowed costs of benefits provided under the plan is at least 60 percent of those costs. The IRS and HHS provided the following approaches for determining minimum value: a Minimum Value Calculator; design-based safe harbor checklists; and actuarial certification. In addition, any plan in the small group market that meets any of the “metal levels” of coverage (that is, bronze, silver, gold or platinum) provides minimum value.
□ Determine whether your health plan provides minimum value by using one of the four available methods (minimum value calculator, safe harbor checklists, actuarial certification or metal level).
Taxes & Fees
ACA Requirement Action Items
Reinsurance Fee
Health insurance issuers and self-funded group health plans that provide major medical coverage must pay fees to a reinsurance program for the first three years of the Exchanges’ operation (2014-2016). Certain self-insured plans are exempt from the reinsurance fees, such as health FSAs and health reimbursement arrangements (HRAs) that are integrated with major medical coverage. For 2015 and 2016, self-insured health plans are exempt from the reinsurance fees if they do not use a third-party administrator in connection with the core administrative functions of claims processing or adjudication or plan enrollment. Health insurers and third-party administrators (TPAs) are responsible for paying the reinsurance program fees on behalf of insured and self-insured plans, respectively.
□ Taking into account the new exception for self-insured, self-administered health plans, review the health coverage you provide to your employees to determine the plan(s) subject to the reinsurance fees for 2016.
□ For 2016, HHS announced a national contribution rate of $27 per enrollee per year (about $2.25 per month). The reinsurance fee is calculated by multiplying the number of covered lives (employees and their dependents) for all of the entity’s plans and coverage that must pay contributions by the national contribution rate for the year.
7
2016 ACA/Regulatory Renewal Checklist For Small Groups (1-50)
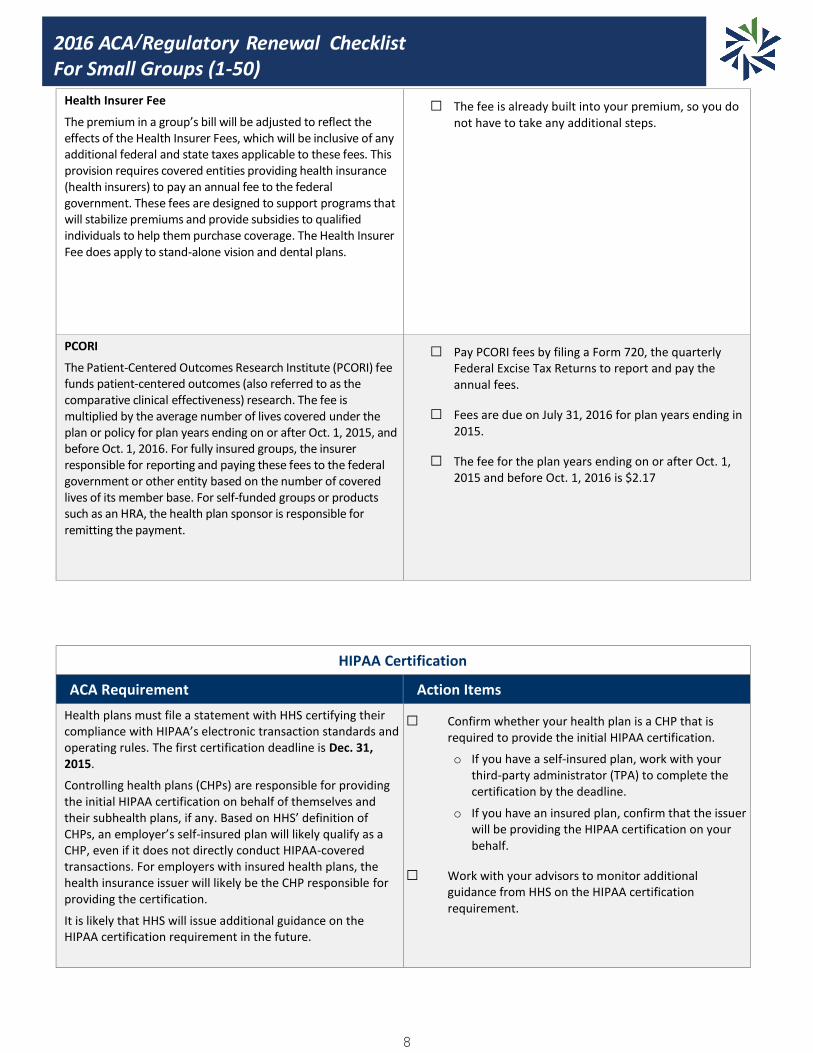
Health Insurer Fee
The premium in a group’s bill will be adjusted to reflect the effects of the Health Insurer Fees, which will be inclusive of any additional federal and state taxes applicable to these fees. This provision requires covered entities providing health insurance (health insurers) to pay an annual fee to the federal government. These fees are designed to support programs that will stabilize premiums and provide subsidies to qualified individuals to help them purchase coverage. The Health Insurer Fee does apply to stand-alone vision and dental plans.
□ The fee is already built into your premium, so you do not have to take any additional steps.
PCORI
The Patient-Centered Outcomes Research Institute (PCORI) fee funds patient-centered outcomes (also referred to as the comparative clinical effectiveness) research. The fee is multiplied by the average number of lives covered under the plan or policy for plan years ending on or after Oct. 1, 2015, and before Oct. 1, 2016. For fully insured groups, the insurer responsible for reporting and paying these fees to the federal government or other entity based on the number of covered lives of its member base. For self-funded groups or products such as an HRA, the health plan sponsor is responsible for remitting the payment.
□ Pay PCORI fees by filing a Form 720, the quarterly Federal Excise Tax Returns to report and pay the annual fees.
□ Fees are due on July 31, 2016 for plan years ending in 2015.
□ The fee for the plan years ending on or after Oct. 1, 2015 and before Oct. 1, 2016 is $2.17
HIPAA Certification
ACA Requirement Action Items
Health plans must file a statement with HHS certifying their compliance with HIPAA’s electronic transaction standards and operating rules. The first certification deadline is Dec. 31, 2015.
Controlling health plans (CHPs) are responsible for providing the initial HIPAA certification on behalf of themselves and their subhealth plans, if any. Based on HHS’ definition of CHPs, an employer’s self-insured plan will likely qualify as a CHP, even if it does not directly conduct HIPAA-covered transactions. For employers with insured health plans, the health insurance issuer will likely be the CHP responsible for providing the certification.
It is likely that HHS will issue additional guidance on the HIPAA certification requirement in the future.
□ Confirm whether your health plan is a CHP that is required to provide the initial HIPAA certification.
o If you have a self-insured plan, work with your third-party administrator (TPA) to complete the certification by the deadline.
o If you have an insured plan, confirm that the issuer will be providing the HIPAA certification on your behalf.
□ Work with your advisors to monitor additional guidance from HHS on the HIPAA certification requirement.
8

2016 ACA/Regulatory Renewal Checklist For Small Groups (1-50)
Health Plan Identifier (HPID) - DELAYED
ACA Requirement Action Items
The HPID, along with the national provider identifier implemented in 2004, is a standard identifier that was required by the original Health Insurance Portability and Accountability Act of 1996 (HIPAA). The original deadline required by the Centers for Medicare and Medicaid services has since been delayed indefinitely until further notice.
No action items at this time, but should a new deadline be provided, the following actions should be taken:
□ To apply for an HPID, go to the CMS Enterprise Portal to obtain a user ID and password (verification process).
□ Then select the link to register in the HIOS (this may take up to 48 hours).
□ After registering, select the HPOES and follow the prompts.
Wellness Incentives
ACA Requirement Action Items
ACA changes the maximum reward that can be provided under HIPAA’s health factor-based wellness program from 20 to 30 percent. The reward under such a program can be up to 30 percent of the cost of employee coverage. Additionally, the secretaries of Health and Human Services, Labor and Treasury can expand the reward up to 50 percent of cost coverage if deemed appropriate.
□ Consider offering wellness incentives as part of a corporate wellness program, which Austin Benefits Group can assist with putting together.
Employer Penalty Rules For employers that are considered large (50 or more employees – including full-time equivalents), there are penalty rules that come into effect, such as:
Employer Shared Responsibility (ESR)
-Affordability test
-Minimum value coverage
-Full-time equivalent tracking
6055/6056 Reporting
Employer Responsibilities
Marketplace Notices – As of Oct. 1, 2013, employers have to provide employees with written notice of the Marketplace. For 2014 and beyond, an employer has to provide the notice to new employees within 14 days of an employee’s start date. The notice is required to be provided automatically, free of charge. It can be provided in writing either by first-class mail, or electronically (www.dol.gov/ebsa/) if the Department of Labor’s electronic disclosure safe harbor requirements are met.
9
2016 ACA/Regulatory Renewal Checklist For Small Groups (1-50)
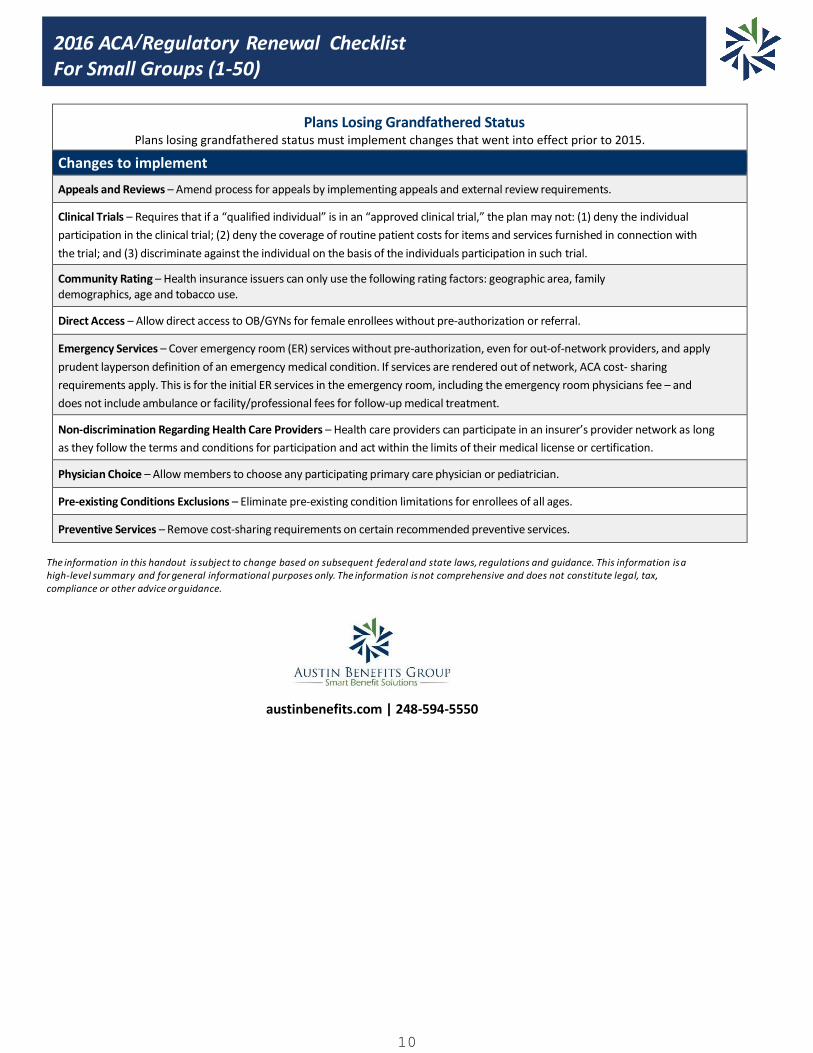
Plans Losing Grandfathered Status Plans losing grandfathered status must implement changes that went into effect prior to 2015.
Changes to implement
Appeals and Reviews – Amend process for appeals by implementing appeals and external review requirements.
Clinical Trials – Requires that if a “qualified individual” is in an “approved clinical trial,” the plan may not: (1) deny the individual
participation in the clinical trial; (2) deny the coverage of routine patient costs for items and services furnished in connection with
the trial; and (3) discriminate against the individual on the basis of the individuals participation in such trial.
Community Rating – Health insurance issuers can only use the following rating factors: geographic area, family demographics, age and tobacco use.
Direct Access – Allow direct access to OB/GYNs for female enrollees without pre-authorization or referral.
Emergency Services – Cover emergency room (ER) services without pre-authorization, even for out-of-network providers, and apply
prudent layperson definition of an emergency medical condition. If services are rendered out of network, ACA cost- sharing
requirements apply. This is for the initial ER services in the emergency room, including the emergency room physicians fee – and
does not include ambulance or facility/professional fees for follow-up medical treatment.
Non-discrimination Regarding Health Care Providers – Health care providers can participate in an insurer’s provider network as long
as they follow the terms and conditions for participation and act within the limits of their medical license or certification.
Physician Choice – Allow members to choose any participating primary care physician or pediatrician.
Pre-existing Conditions Exclusions – Eliminate pre-existing condition limitations for enrollees of all ages.
Preventive Services – Remove cost-sharing requirements on certain recommended preventive services.
The information in this handout is subject to change based on subsequent federal and state laws, regulations and guidance. This information is a high-level summary and for general informational purposes only. The information is not comprehensive and does not constitute legal, tax, compliance or other advice or guidance.
austinbenefits.com | 248-594-5550
10

FINANCIAL ANALYSIS
SMART BENEFIT SOLUTIONS
11
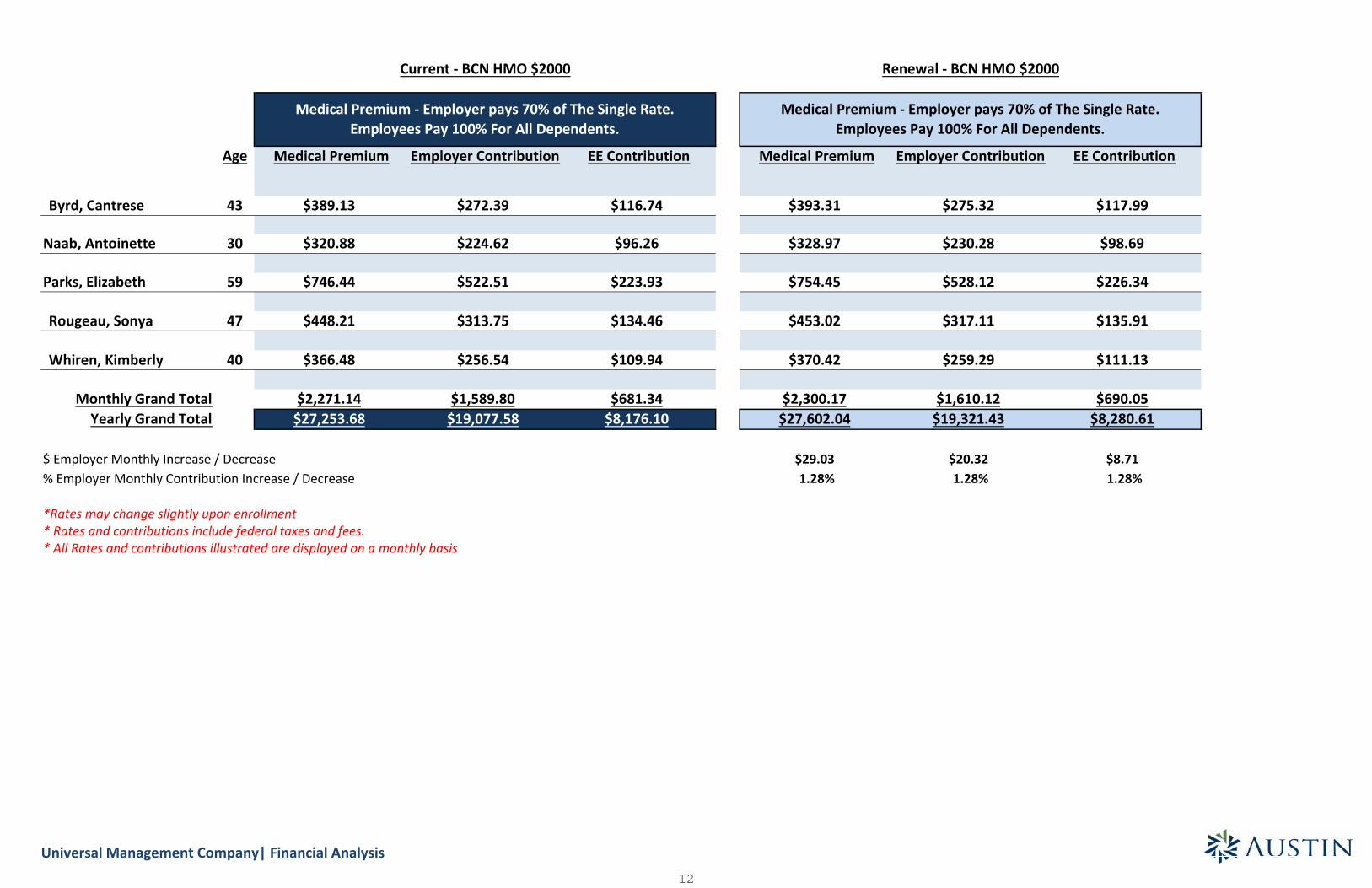
Age Medical Premium Employer Contribution EE Contribution Medical Premium Employer Contribution EE Contribution
Byrd, Cantrese 43 $389.13 $272.39 $116.74 $393.31 $275.32 $117.99
Naab, Antoinette 30 $320.88 $224.62 $96.26 $328.97 $230.28 $98.69
Parks, Elizabeth 59 $746.44 $522.51 $223.93 $754.45 $528.12 $226.34
Rougeau, Sonya 47 $448.21 $313.75 $134.46 $453.02 $317.11 $135.91
Whiren, Kimberly 40 $366.48 $256.54 $109.94 $370.42 $259.29 $111.13
Monthly Grand Total $2,271.14 $1,589.80 $681.34 $2,300.17 $1,610.12 $690.05Yearly Grand Total $27,253.68 $19,077.58 $8,176.10 $27,602.04 $19,321.43 $8,280.61
$ Employer Monthly Increase / Decrease $29.03 $20.32 $8.71% Employer Monthly Contribution Increase / Decrease 1.28% 1.28% 1.28%
*Rates may change slightly upon enrollment* Rates and contributions include federal taxes and fees.* All Rates and contributions illustrated are displayed on a monthly basis
Current - BCN HMO $2000 Renewal - BCN HMO $2000
Medical Premium - Employer pays 70% of The Single Rate.Employees Pay 100% For All Dependents.
Medical Premium - Employer pays 70% of The Single Rate.Employees Pay 100% For All Dependents.
Universal Management Company| Financial Analysis12

MEDICAL PLAN OPTIONS
SMART BENEFIT SOLUTIONS
13
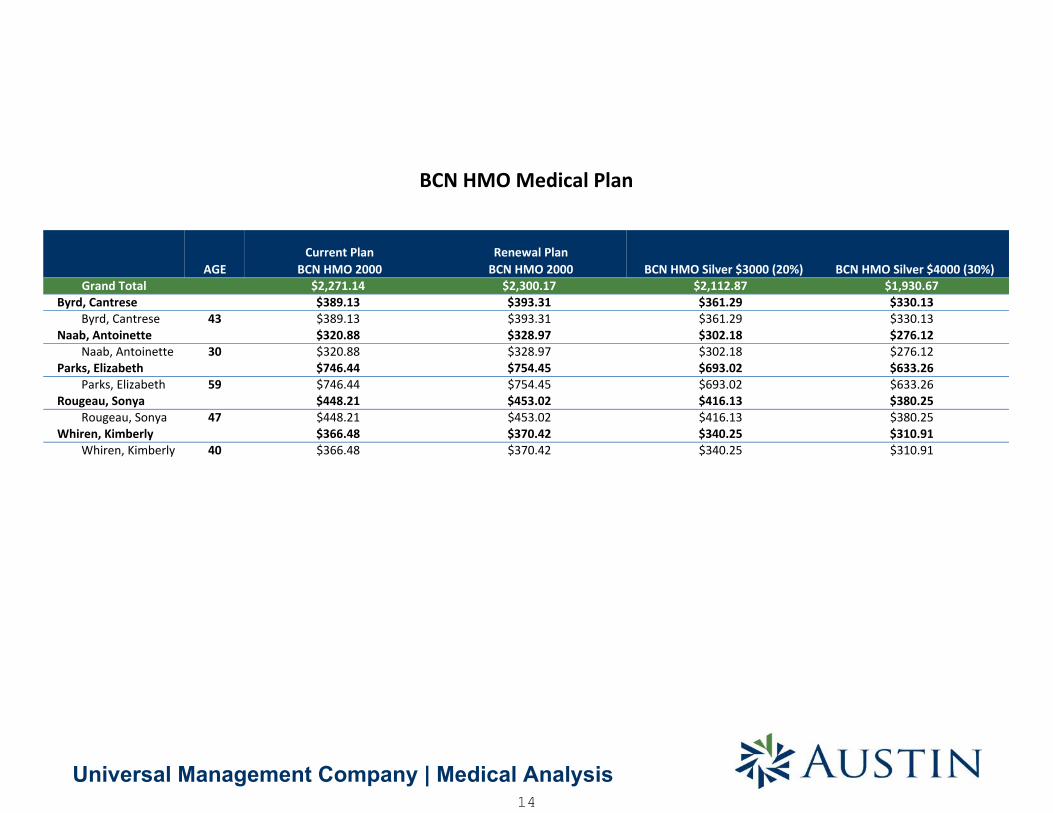
AGECurrent Plan
BCN HMO 2000Renewal Plan
BCN HMO 2000 BCN HMO Silver $3000 (20%) BCN HMO Silver $4000 (30%)Grand Total $2,271.14 $2,300.17 $2,112.87 $1,930.67
Byrd, Cantrese $389.13 $393.31 $361.29 $330.13Byrd, Cantrese 43 $389.13 $393.31 $361.29 $330.13
Naab, Antoinette $320.88 $328.97 $302.18 $276.12Naab, Antoinette 30 $320.88 $328.97 $302.18 $276.12
Parks, Elizabeth $746.44 $754.45 $693.02 $633.26Parks, Elizabeth 59 $746.44 $754.45 $693.02 $633.26
Rougeau, Sonya $448.21 $453.02 $416.13 $380.25Rougeau, Sonya 47 $448.21 $453.02 $416.13 $380.25
Whiren, Kimberly $366.48 $370.42 $340.25 $310.91Whiren, Kimberly 40 $366.48 $370.42 $340.25 $310.91
BCN HMO Medical Plan
Universal Management Company | Medical Analysis14

Universal Management Company | Medical Analysis
$-
$500.00
$1,000.00
$1,500.00
$2,000.00
$2,500.00
CurrentRates
RenewalRates
BCN HMOSilver$3000(20%)
BCN HMOSilver$4000(30%)
SB Silver$2000
SB PPOSilver$3000
HAP 2000HMO II
HAP 3000HMO
HAP 2000PPO II
HAP 3000PPO
PH HMO2000
PH HMO3000
PH PPO2000
PH PPO3000
15
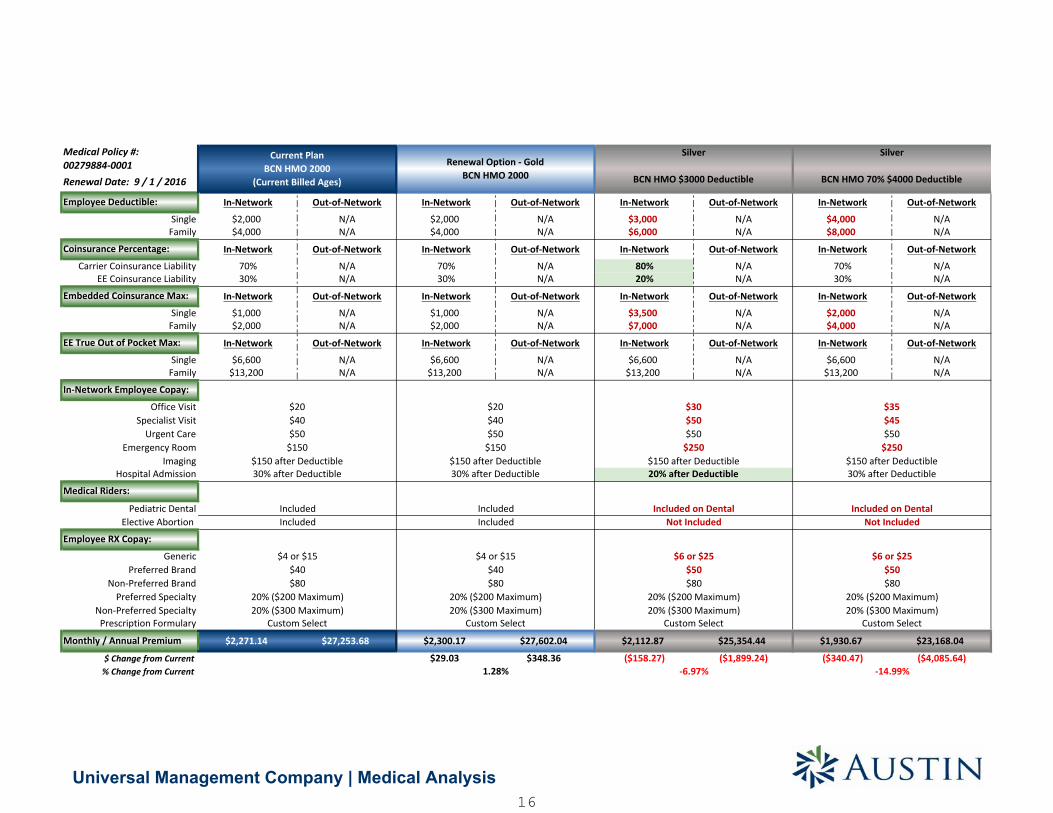
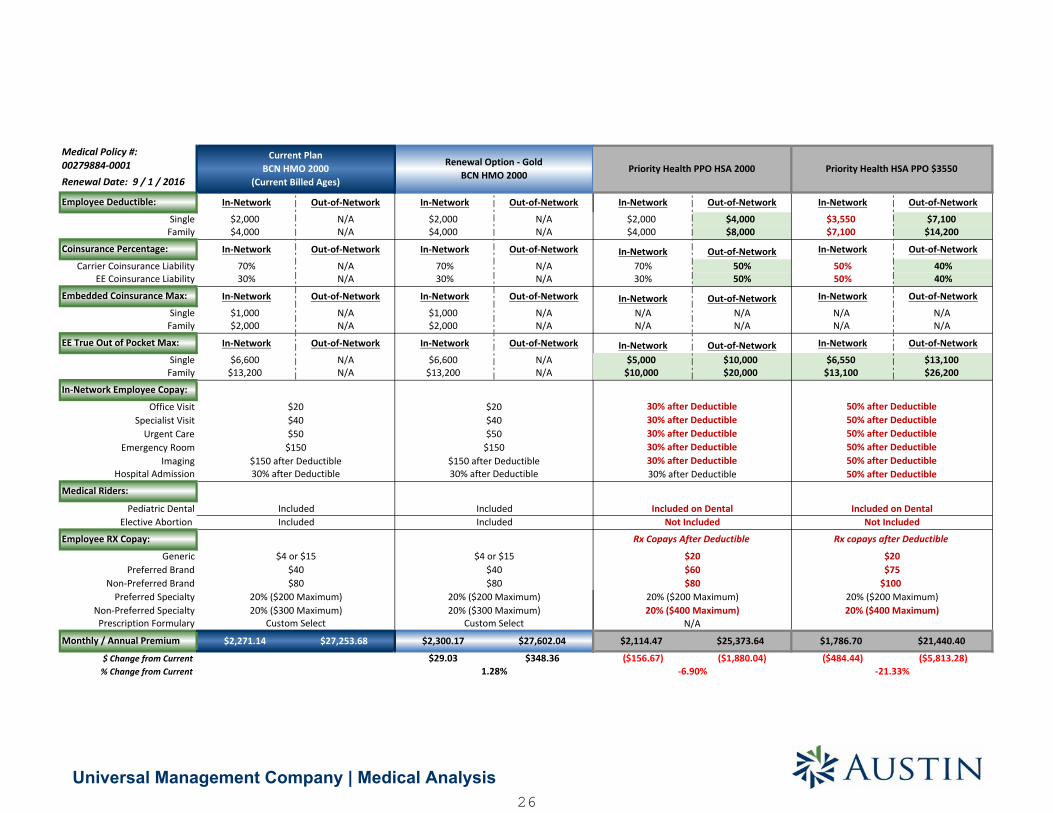
00279884-0001
In-Network Out-of-Network In-Network Out-of-Network In-Network Out-of-Network In-Network Out-of-Network
$2,000 N/A $2,000 N/A $3,000 N/A $4,000 N/A$4,000 N/A $4,000 N/A $6,000 N/A $8,000 N/A
In-Network Out-of-Network In-Network Out-of-Network In-Network Out-of-Network In-Network Out-of-Network
70% N/A 70% N/A 80% N/A 70% N/A30% N/A 30% N/A 20% N/A 30% N/A
In-Network Out-of-Network In-Network Out-of-Network In-Network Out-of-Network In-Network Out-of-Network
$1,000 N/A $1,000 N/A $3,500 N/A $2,000 N/A$2,000 N/A $2,000 N/A $7,000 N/A $4,000 N/A
In-Network Out-of-Network In-Network Out-of-Network In-Network Out-of-Network In-Network Out-of-Network
$6,600 N/A $6,600 N/A $6,600 N/A $6,600 N/A$13,200 N/A $13,200 N/A $13,200 N/A $13,200 N/A
Elective Abortion
Prescription Formulary
$2,271.14 $27,253.68 $2,300.17 $27,602.04 $2,112.87 $25,354.44 $1,930.67 $23,168.04
$29.03 $348.36 ($158.27) ($1,899.24) ($340.47) ($4,085.64)
Included
$40
Included
$ Change from Current% Change from Current 1.28%
Monthly / Annual Premium
Specialist Visit
EE Coinsurance Liability
EE True Out of Pocket Max:
Single
Office Visit $20
$40$80
20% ($200 Maximum)
Preferred Brand $40
Non-Preferred Specialty
$4 or $15
Non-Preferred Brand
20% ($300 Maximum)
$80
20% ($300 Maximum) 20% ($300 Maximum)
SingleFamily
30% after Deductible 30% after Deductible
Urgent Care $50 $50
Hospital Admission
$150 $150Emergency Room
Embedded Coinsurance Max:
Renewal Option - GoldBCN HMO 2000
Current PlanBCN HMO 2000
(Current Billed Ages)
Generic
20% ($300 Maximum)
Not Included Not Included
Custom Select
Silver
BCN HMO $3000 Deductible
Silver
BCN HMO 70% $4000 Deductible
Pediatric Dental
Preferred Specialty 20% ($200 Maximum)
$6 or $25 $6 or $25$50
$8020% ($200 Maximum)
Medical Riders:
Imaging $150 after Deductible $150 after Deductible
Included Included on DentalIncluded
Employee RX Copay:
$20 $35$45$50
Family
In-Network Employee Copay:
Coinsurance Percentage:
Carrier Coinsurance Liability
$40
Medical Policy #:
Employee Deductible:
Renewal Date: 9 / 1 / 2016
SingleFamily
$150 after Deductible30% after Deductible
Included on Dental
-6.97%
$30$50$50
$250$150 after Deductible20% after Deductible
$50
$250
-14.99%
$8020% ($200 Maximum)
Custom Select Custom Select Custom Select
$4 or $15
Universal Management Company | Medical Analysis16
00279884-0001
In-Network Out-of-Network In-Network Out-of-Network
$2,000 N/A $2,000 N/A$4,000 N/A $4,000 N/A
In-Network Out-of-Network In-Network Out-of-Network
70% N/A 70% N/A30% N/A 30% N/A
In-Network Out-of-Network In-Network Out-of-Network
$1,000 N/A $1,000 N/A$2,000 N/A $2,000 N/A
In-Network Out-of-Network In-Network Out-of-Network
$6,600 N/A $6,600 N/A$13,200 N/A $13,200 N/A
Elective Abortion
Prescription Formulary
$2,271.14 $27,253.68 $2,300.17 $27,602.04
$29.03 $348.36
Included
$40
Included
$ Change from Current% Change from Current 1.28%
Monthly / Annual Premium
Specialist Visit
EE Coinsurance Liability
EE True Out of Pocket Max:
Single
Office Visit $20
$40$80
20% ($200 Maximum)
Preferred Brand $40
Non-Preferred Specialty
$4 or $15
Non-Preferred Brand
20% ($300 Maximum)
$80
SingleFamily
30% after Deductible 30% after Deductible
Urgent Care $50 $50
Hospital Admission
$150 $150Emergency Room
Embedded Coinsurance Max:
Renewal Option - GoldBCN HMO 2000
Current PlanBCN HMO 2000
(Current Billed Ages)
Generic
20% ($300 Maximum)
Pediatric Dental
Preferred Specialty 20% ($200 Maximum)
Medical Riders:
Imaging $150 after Deductible $150 after Deductible
IncludedIncluded
Employee RX Copay:
$20
Family
In-Network Employee Copay:
Coinsurance Percentage:
Carrier Coinsurance Liability
$40
Medical Policy #:
Employee Deductible:
Renewal Date: 9 / 1 / 2016
SingleFamily
Custom Select Custom Select
$4 or $15
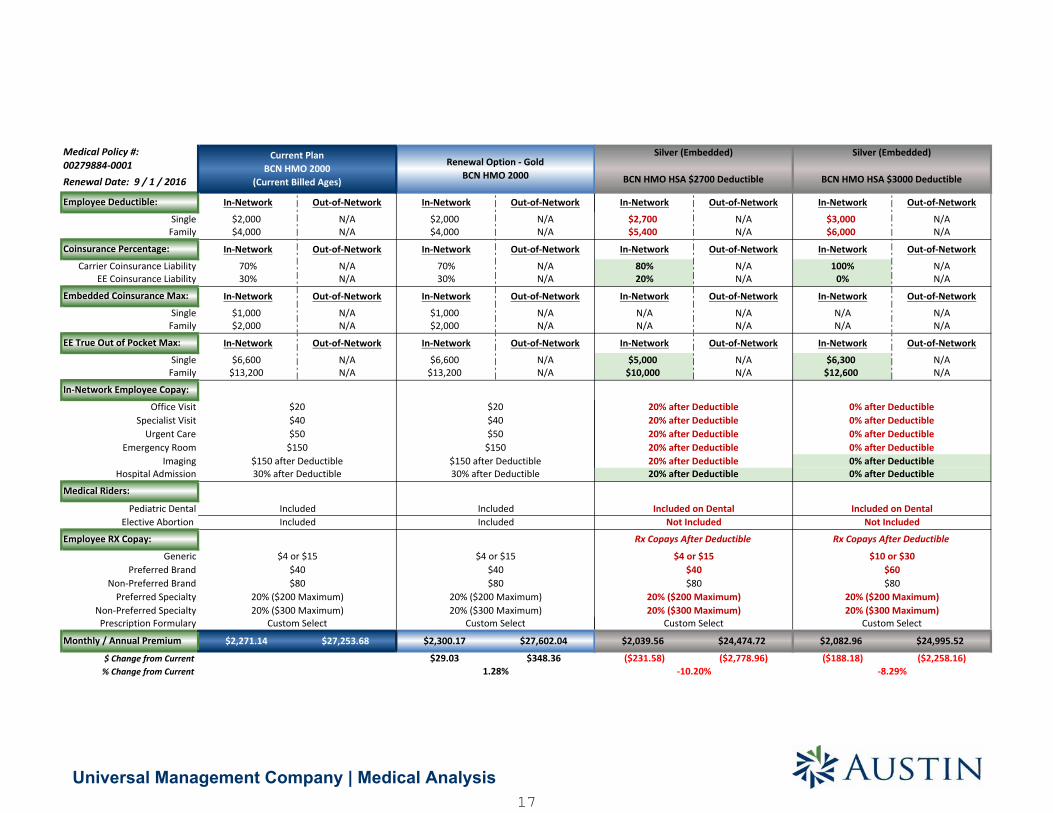
In-Network Out-of-Network In-Network Out-of-Network
$2,700 N/A $3,000 N/A$5,400 N/A $6,000 N/A
In-Network Out-of-Network In-Network Out-of-Network
80% N/A 100% N/A20% N/A 0% N/A
In-Network Out-of-Network In-Network Out-of-Network
N/A N/A N/A N/AN/A N/A N/A N/A
In-Network Out-of-Network In-Network Out-of-Network
$5,000 N/A $6,300 N/A$10,000 N/A $12,600 N/A
$2,039.56 $24,474.72 $2,082.96 $24,995.52
($231.58) ($2,778.96) ($188.18) ($2,258.16)
Not Included Not Included
Silver (Embedded)
BCN HMO HSA $3000 Deductible
Silver (Embedded)
BCN HMO HSA $2700 Deductible
20% ($300 Maximum)
0% after Deductible
Included on DentalIncluded on Dental
-8.29%
20% after Deductible20% after Deductible20% after Deductible20% after Deductible20% after Deductible20% after Deductible
Custom Select
Rx Copays After Deductible
$4 or $15$40
Rx Copays After Deductible
$10 or $30$60$80
20% ($200 Maximum)20% ($300 Maximum)
0% after Deductible0% after Deductible0% after Deductible0% after Deductible0% after Deductible
-10.20%
$8020% ($200 Maximum)
Custom Select
Universal Management Company | Medical Analysis17
00279884-0001
In-Network Out-of-Network In-Network Out-of-Network
$2,000 N/A $2,000 N/A$4,000 N/A $4,000 N/A
In-Network Out-of-Network In-Network Out-of-Network
70% N/A 70% N/A30% N/A 30% N/A
In-Network Out-of-Network In-Network Out-of-Network
$1,000 N/A $1,000 N/A$2,000 N/A $2,000 N/A
In-Network Out-of-Network In-Network Out-of-Network
$6,600 N/A $6,600 N/A$13,200 N/A $13,200 N/A
Elective Abortion
Prescription Formulary
$2,271.14 $27,253.68 $2,300.17 $27,602.04
$29.03 $348.36
Included
$40
Included
$ Change from Current% Change from Current 1.28%
Monthly / Annual Premium
Specialist Visit
EE Coinsurance Liability
EE True Out of Pocket Max:
Single
Office Visit $20
$40$80
20% ($200 Maximum)
Preferred Brand $40
Non-Preferred Specialty
$4 or $15
Non-Preferred Brand
20% ($300 Maximum)
$80
SingleFamily
30% after Deductible 30% after Deductible
Urgent Care $50 $50
Hospital Admission
$150 $150Emergency Room
Embedded Coinsurance Max:
Renewal Option - GoldBCN HMO 2000
Current PlanBCN HMO 2000
(Current Billed Ages)
Generic
20% ($300 Maximum)
Pediatric Dental
Preferred Specialty 20% ($200 Maximum)
Medical Riders:
Imaging $150 after Deductible $150 after Deductible
IncludedIncluded
Employee RX Copay:
$20
Family
In-Network Employee Copay:
Coinsurance Percentage:
Carrier Coinsurance Liability
$40
Medical Policy #:
Employee Deductible:
Renewal Date: 9 / 1 / 2016
SingleFamily
Custom Select Custom Select
$4 or $15
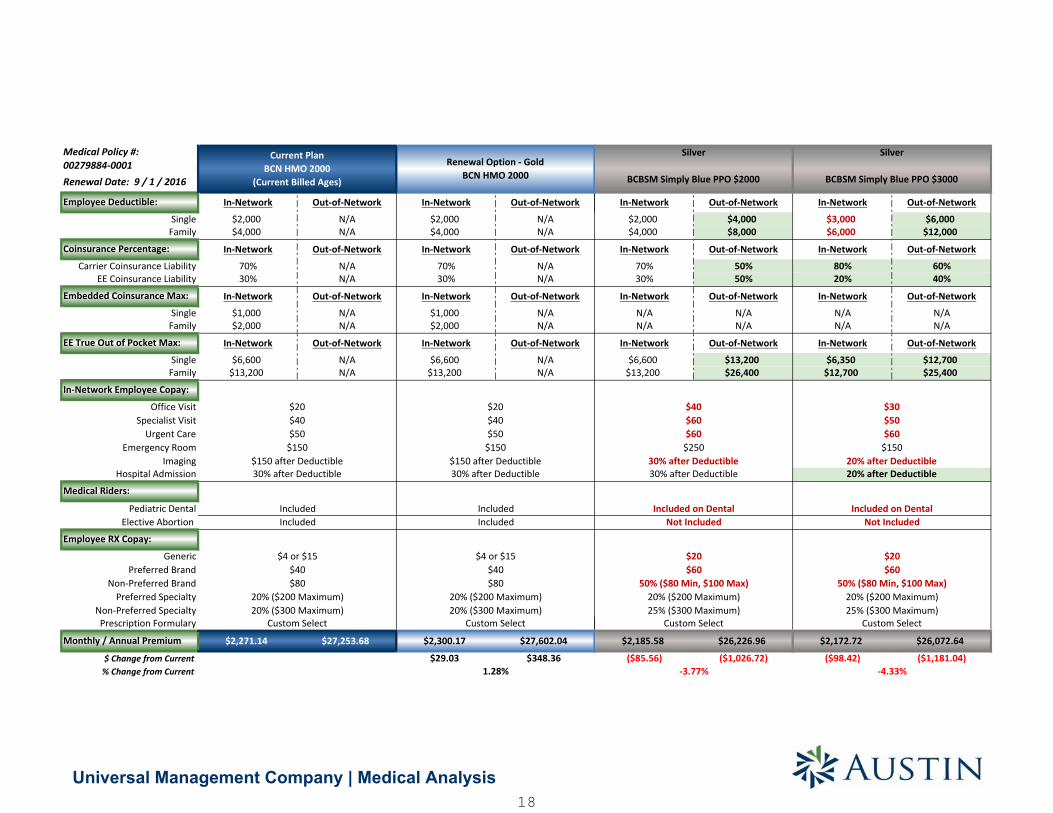
In-Network Out-of-Network In-Network Out-of-Network
$2,000 $4,000 $3,000 $6,000$4,000 $8,000 $6,000 $12,000
In-Network Out-of-Network In-Network Out-of-Network
70% 50% 80% 60%30% 50% 20% 40%
In-Network Out-of-Network In-Network Out-of-Network
N/A N/A N/A N/AN/A N/A N/A N/A
In-Network Out-of-Network In-Network Out-of-Network
$6,600 $13,200 $6,350 $12,700$13,200 $26,400 $12,700 $25,400
$2,185.58 $26,226.96 $2,172.72 $26,072.64
($85.56) ($1,026.72) ($98.42) ($1,181.04)-4.33%
Not Included
Custom Select
Not Included
30% after Deductible
25% ($300 Maximum) 25% ($300 Maximum)Custom Select
Included on Dental
50% ($80 Min, $100 Max)
$20$60
-3.77%
20% ($200 Maximum)
$15020% after Deductible20% after Deductible
$50$60
Silver
BCBSM Simply Blue PPO $2000
Silver
BCBSM Simply Blue PPO $3000
$30
20% ($200 Maximum)
30% after Deductible$250
$40
$60$60
Included on Dental
$20$60
50% ($80 Min, $100 Max)
Universal Management Company | Medical Analysis18
00279884-0001
In-Network Out-of-Network In-Network Out-of-Network
$2,000 N/A $2,000 N/A$4,000 N/A $4,000 N/A
In-Network Out-of-Network In-Network Out-of-Network
70% N/A 70% N/A30% N/A 30% N/A
In-Network Out-of-Network In-Network Out-of-Network
$1,000 N/A $1,000 N/A$2,000 N/A $2,000 N/A
In-Network Out-of-Network In-Network Out-of-Network
$6,600 N/A $6,600 N/A$13,200 N/A $13,200 N/A
Elective Abortion
Prescription Formulary
$2,271.14 $27,253.68 $2,300.17 $27,602.04
$29.03 $348.36
Included
$40
Included
$ Change from Current% Change from Current 1.28%
Monthly / Annual Premium
Specialist Visit
EE Coinsurance Liability
EE True Out of Pocket Max:
Single
Office Visit $20
$40$80
20% ($200 Maximum)
Preferred Brand $40
Non-Preferred Specialty
$4 or $15
Non-Preferred Brand
20% ($300 Maximum)
$80
SingleFamily
30% after Deductible 30% after Deductible
Urgent Care $50 $50
Hospital Admission
$150 $150Emergency Room
Embedded Coinsurance Max:
Renewal Option - GoldBCN HMO 2000
Current PlanBCN HMO 2000
(Current Billed Ages)
Generic
20% ($300 Maximum)
Pediatric Dental
Preferred Specialty 20% ($200 Maximum)
Medical Riders:
Imaging $150 after Deductible $150 after Deductible
IncludedIncluded
Employee RX Copay:
$20
Family
In-Network Employee Copay:
Coinsurance Percentage:
Carrier Coinsurance Liability
$40
Medical Policy #:
Employee Deductible:
Renewal Date: 9 / 1 / 2016
SingleFamily
Custom Select Custom Select
$4 or $15
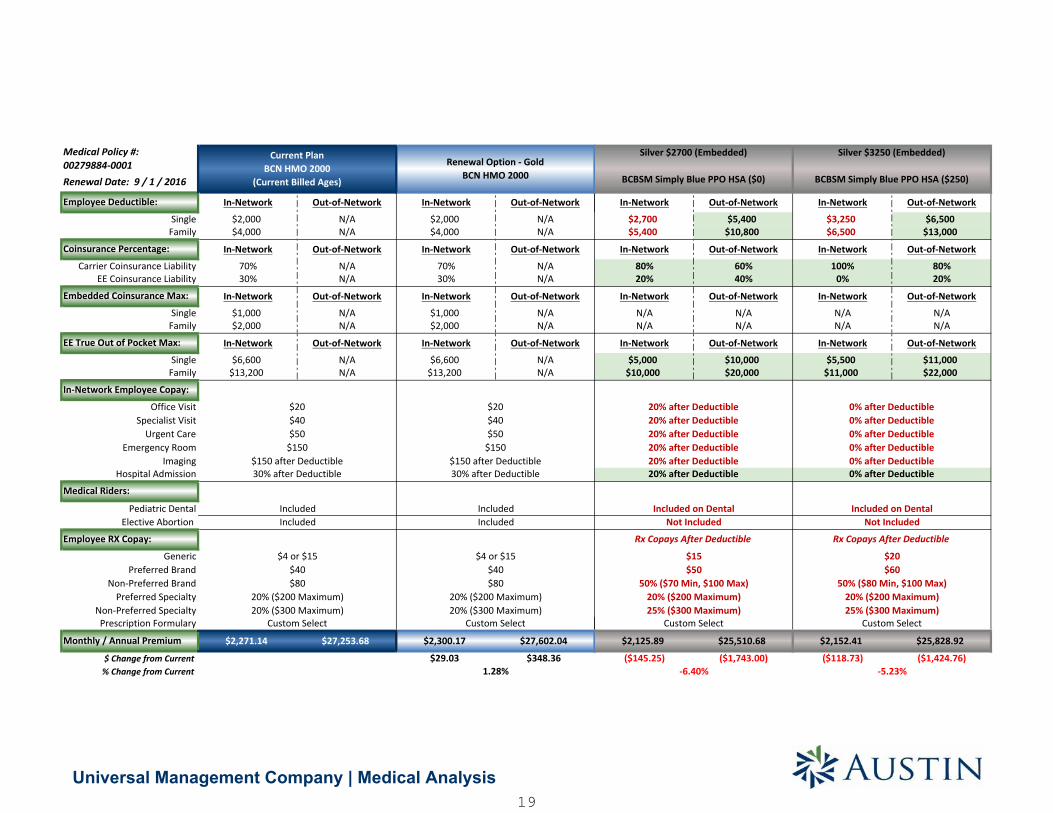
In-Network Out-of-Network In-Network Out-of-Network
$2,700 $5,400 $3,250 $6,500$5,400 $10,800 $6,500 $13,000
In-Network Out-of-Network In-Network Out-of-Network
80% 60% 100% 80%20% 40% 0% 20%
In-Network Out-of-Network In-Network Out-of-Network
N/A N/A N/A N/AN/A N/A N/A N/A
In-Network Out-of-Network In-Network Out-of-Network
$5,000 $10,000 $5,500 $11,000$10,000 $20,000 $11,000 $22,000
$2,125.89 $25,510.68 $2,152.41 $25,828.92
($145.25) ($1,743.00) ($118.73) ($1,424.76)
Custom Select
Not Included
25% ($300 Maximum)
-5.23%
50% ($70 Min, $100 Max)
-6.40%
0% after Deductible
$15$50
0% after Deductible
Not Included
20% after Deductible
Silver $3250 (Embedded)
BCBSM Simply Blue PPO HSA ($250)
0% after Deductible0% after Deductible
Rx Copays After Deductible
20% ($200 Maximum)
20% after Deductible20% after Deductible
20% after Deductible
20% after Deductible0% after Deductible
20% after Deductible
Included on Dental
0% after Deductible
Silver $2700 (Embedded)
BCBSM Simply Blue PPO HSA ($0)
Included on Dental
Rx Copays After Deductible
$20$60
50% ($80 Min, $100 Max)20% ($200 Maximum)25% ($300 Maximum)
Custom Select
Universal Management Company | Medical Analysis19
00279884-0001
In-Network Out-of-Network In-Network Out-of-Network
$2,000 N/A $2,000 N/A$4,000 N/A $4,000 N/A
In-Network Out-of-Network In-Network Out-of-Network
70% N/A 70% N/A30% N/A 30% N/A
In-Network Out-of-Network In-Network Out-of-Network
$1,000 N/A $1,000 N/A$2,000 N/A $2,000 N/A
In-Network Out-of-Network In-Network Out-of-Network
$6,600 N/A $6,600 N/A$13,200 N/A $13,200 N/A
Elective Abortion
Prescription Formulary
$2,271.14 $27,253.68 $2,300.17 $27,602.04
$29.03 $348.36
Included
$40
Included
$ Change from Current% Change from Current 1.28%
Monthly / Annual Premium
Specialist Visit
EE Coinsurance Liability
EE True Out of Pocket Max:
Single
Office Visit $20
$40$80
20% ($200 Maximum)
Preferred Brand $40
Non-Preferred Specialty
$4 or $15
Non-Preferred Brand
20% ($300 Maximum)
$80
SingleFamily
30% after Deductible 30% after Deductible
Urgent Care $50 $50
Hospital Admission
$150 $150Emergency Room
Embedded Coinsurance Max:
Renewal Option - GoldBCN HMO 2000
Current PlanBCN HMO 2000
(Current Billed Ages)
Generic
20% ($300 Maximum)
Pediatric Dental
Preferred Specialty 20% ($200 Maximum)
Medical Riders:
Imaging $150 after Deductible $150 after Deductible
IncludedIncluded
Employee RX Copay:
$20
Family
In-Network Employee Copay:
Coinsurance Percentage:
Carrier Coinsurance Liability
$40
Medical Policy #:
Employee Deductible:
Renewal Date: 9 / 1 / 2016
SingleFamily
Custom Select Custom Select
$4 or $15
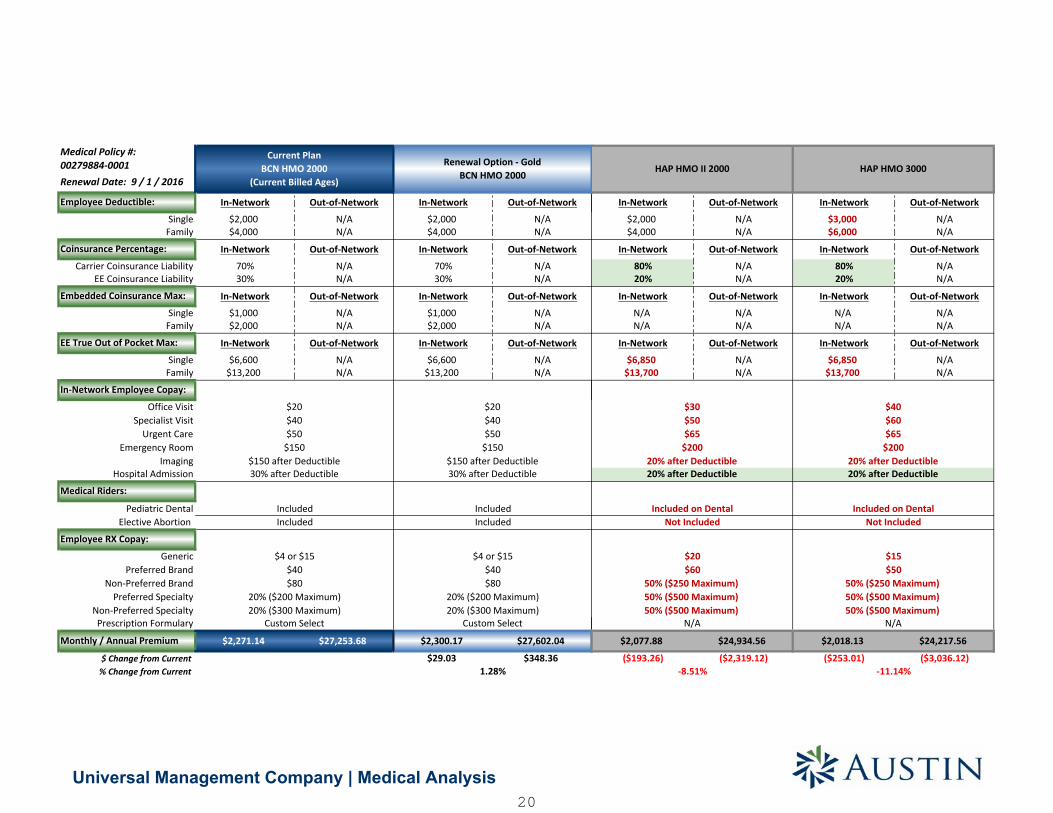
In-Network Out-of-Network In-Network Out-of-Network
$2,000 N/A $3,000 N/A$4,000 N/A $6,000 N/A
In-Network Out-of-Network In-Network Out-of-Network
80% N/A 80% N/A20% N/A 20% N/A
In-Network Out-of-Network In-Network Out-of-Network
N/A N/A N/A N/AN/A N/A N/A N/A
In-Network Out-of-Network In-Network Out-of-Network
$6,850 N/A $6,850 N/A$13,700 N/A $13,700 N/A
$2,077.88 $24,934.56 $2,018.13 $24,217.56
($193.26) ($2,319.12) ($253.01) ($3,036.12)
$30 $40
Not Included Not Included
$20 $15
$65
20% after Deductible 20% after Deductible
Included on Dental Included on Dental
$60 $50
HAP HMO II 2000 HAP HMO 3000
$50 $60$65
$200 $20020% after Deductible 20% after Deductible
50% ($250 Maximum) 50% ($250 Maximum)
50% ($500 Maximum) 50% ($500 Maximum)N/A N/A
-8.51% -11.14%
50% ($500 Maximum) 50% ($500 Maximum)
Universal Management Company | Medical Analysis20
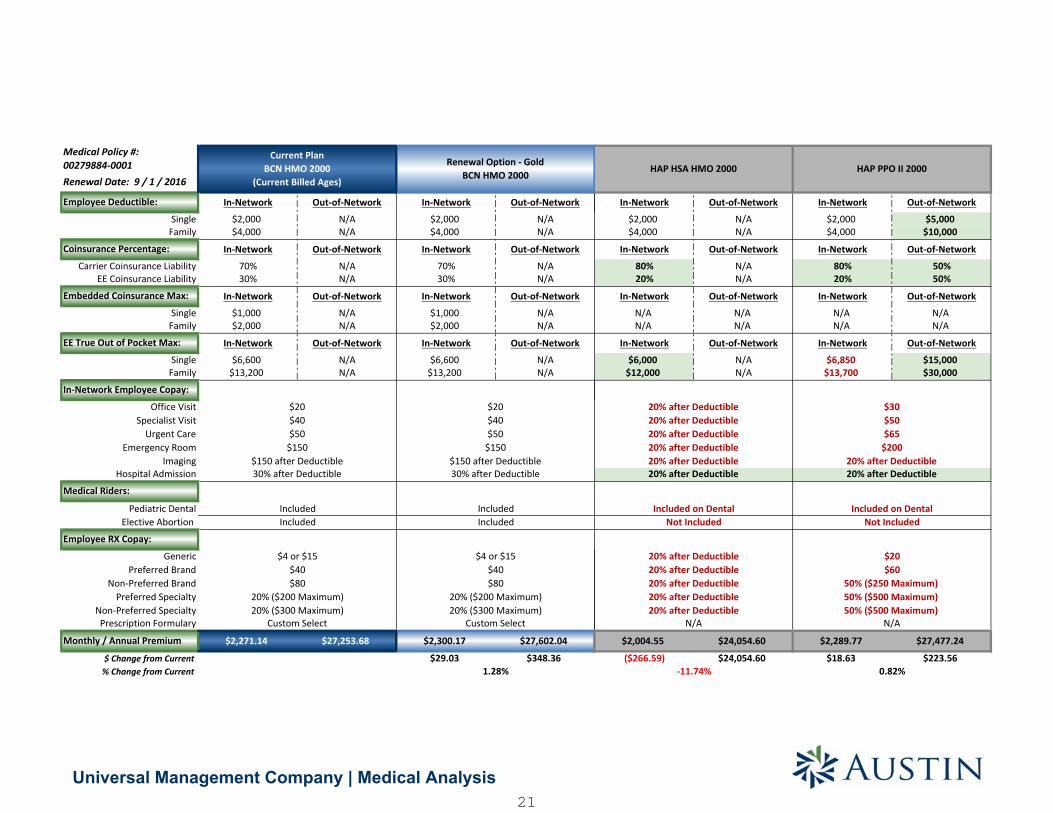
00279884-0001
In-Network Out-of-Network In-Network Out-of-Network
$2,000 N/A $2,000 N/A$4,000 N/A $4,000 N/A
In-Network Out-of-Network In-Network Out-of-Network
70% N/A 70% N/A30% N/A 30% N/A
In-Network Out-of-Network In-Network Out-of-Network
$1,000 N/A $1,000 N/A$2,000 N/A $2,000 N/A
In-Network Out-of-Network In-Network Out-of-Network
$6,600 N/A $6,600 N/A$13,200 N/A $13,200 N/A
Elective Abortion
Prescription Formulary
$2,271.14 $27,253.68 $2,300.17 $27,602.04
$29.03 $348.36
Included
$40
Included
$ Change from Current% Change from Current 1.28%
Monthly / Annual Premium
Specialist Visit
EE Coinsurance Liability
EE True Out of Pocket Max:
Single
Office Visit $20
$40$80
20% ($200 Maximum)
Preferred Brand $40
Non-Preferred Specialty
$4 or $15
Non-Preferred Brand
20% ($300 Maximum)
$80
SingleFamily
30% after Deductible 30% after Deductible
Urgent Care $50 $50
Hospital Admission
$150 $150Emergency Room
Embedded Coinsurance Max:
Renewal Option - GoldBCN HMO 2000
Current PlanBCN HMO 2000
(Current Billed Ages)
Generic
20% ($300 Maximum)
Pediatric Dental
Preferred Specialty 20% ($200 Maximum)
Medical Riders:
Imaging $150 after Deductible $150 after Deductible
IncludedIncluded
Employee RX Copay:
$20
Family
In-Network Employee Copay:
Coinsurance Percentage:
Carrier Coinsurance Liability
$40
Medical Policy #:
Employee Deductible:
Renewal Date: 9 / 1 / 2016
SingleFamily
Custom Select Custom Select
$4 or $15
In-Network Out-of-Network In-Network Out-of-Network
$2,000 N/A $2,000 $5,000$4,000 N/A $4,000 $10,000
In-Network Out-of-Network In-Network Out-of-Network
80% N/A 80% 50%20% N/A 20% 50%
In-Network Out-of-Network In-Network Out-of-Network
N/A N/A N/A N/AN/A N/A N/A N/A
In-Network Out-of-Network In-Network Out-of-Network
$6,000 N/A $6,850 $15,000$12,000 N/A $13,700 $30,000
$2,004.55 $24,054.60 $2,289.77 $27,477.24
($266.59) $24,054.60 $18.63 $223.56
HAP PPO II 2000
50% ($250 Maximum)
0.82%
$30$50$65
$200
Included on Dental
$20
50% ($500 Maximum)
$60
50% ($500 Maximum)
Not Included
20% after Deductible
20% after Deductible
HAP HSA HMO 2000
20% after Deductible20% after Deductible
20% after Deductible20% after Deductible20% after Deductible
20% after Deductible20% after Deductible
Included on DentalNot Included
20% after Deductible20% after Deductible
-11.74%
20% after Deductible20% after Deductible
N/AN/A
Universal Management Company | Medical Analysis21
00279884-0001
In-Network Out-of-Network In-Network Out-of-Network
$2,000 N/A $2,000 N/A$4,000 N/A $4,000 N/A
In-Network Out-of-Network In-Network Out-of-Network
70% N/A 70% N/A30% N/A 30% N/A
In-Network Out-of-Network In-Network Out-of-Network
$1,000 N/A $1,000 N/A$2,000 N/A $2,000 N/A
In-Network Out-of-Network In-Network Out-of-Network
$6,600 N/A $6,600 N/A$13,200 N/A $13,200 N/A
Elective Abortion
Prescription Formulary
$2,271.14 $27,253.68 $2,300.17 $27,602.04
$29.03 $348.36
Included
$40
Included
$ Change from Current% Change from Current 1.28%
Monthly / Annual Premium
Specialist Visit
EE Coinsurance Liability
EE True Out of Pocket Max:
Single
Office Visit $20
$40$80
20% ($200 Maximum)
Preferred Brand $40
Non-Preferred Specialty
$4 or $15
Non-Preferred Brand
20% ($300 Maximum)
$80
SingleFamily
30% after Deductible 30% after Deductible
Urgent Care $50 $50
Hospital Admission
$150 $150Emergency Room
Embedded Coinsurance Max:
Renewal Option - GoldBCN HMO 2000
Current PlanBCN HMO 2000
(Current Billed Ages)
Generic
20% ($300 Maximum)
Pediatric Dental
Preferred Specialty 20% ($200 Maximum)
Medical Riders:
Imaging $150 after Deductible $150 after Deductible
IncludedIncluded
Employee RX Copay:
$20
Family
In-Network Employee Copay:
Coinsurance Percentage:
Carrier Coinsurance Liability
$40
Medical Policy #:
Employee Deductible:
Renewal Date: 9 / 1 / 2016
SingleFamily
Custom Select Custom Select
$4 or $15
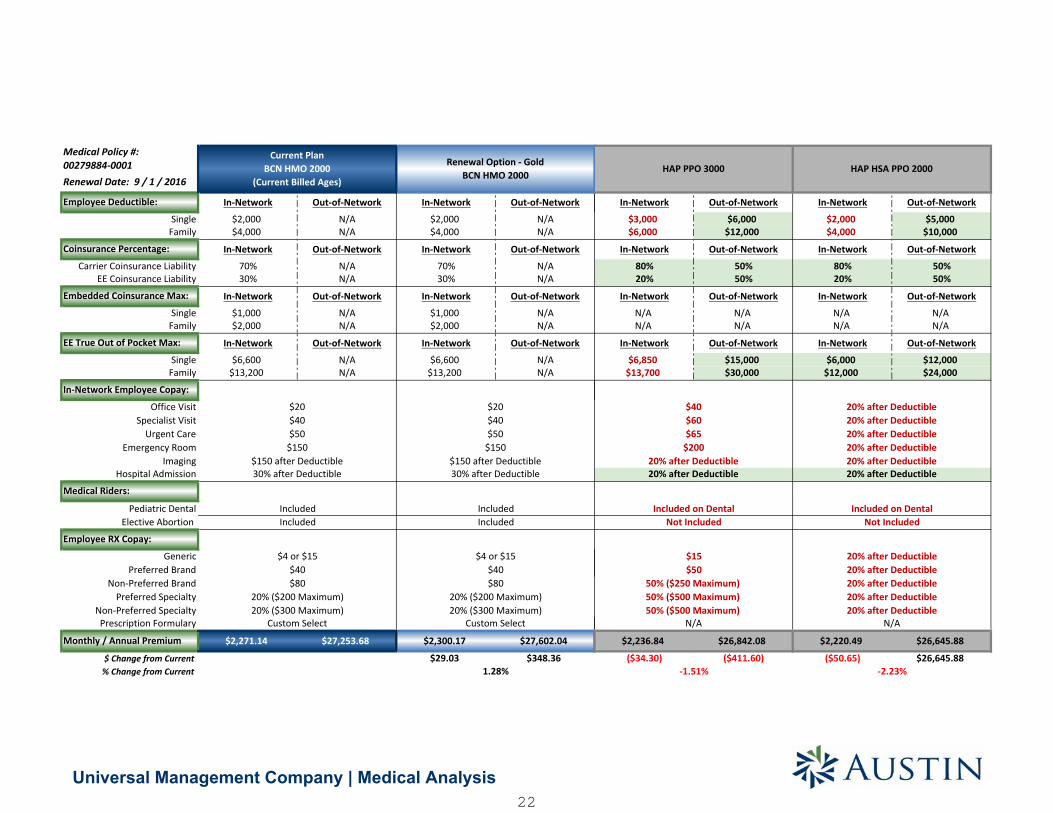
In-Network Out-of-Network In-Network Out-of-Network
$3,000 $6,000 $2,000 $5,000$6,000 $12,000 $4,000 $10,000
In-Network Out-of-Network In-Network Out-of-Network
80% 50% 80% 50%20% 50% 20% 50%
In-Network Out-of-Network In-Network Out-of-Network
N/A N/A N/A N/AN/A N/A N/A N/A
In-Network Out-of-Network In-Network Out-of-Network
$6,850 $15,000 $6,000 $12,000$13,700 $30,000 $12,000 $24,000
$2,236.84 $26,842.08 $2,220.49 $26,645.88
($34.30) ($411.60) ($50.65) $26,645.88
HAP PPO 3000
$5050% ($250 Maximum)50% ($500 Maximum)
$65$200
20% after Deductible20% after Deductible
Included on Dental
HAP HSA PPO 2000
$40$60
Not IncludedNot IncludedIncluded on Dental
20% after Deductible20% after Deductible
20% after Deductible$15
-2.23%
20% after Deductible20% after Deductible50% ($500 Maximum)
-1.51%
N/A N/A
20% after Deductible20% after Deductible20% after Deductible20% after Deductible20% after Deductible20% after Deductible
Universal Management Company | Medical Analysis22
00279884-0001
In-Network Out-of-Network In-Network Out-of-Network
$2,000 N/A $2,000 N/A$4,000 N/A $4,000 N/A
In-Network Out-of-Network In-Network Out-of-Network
70% N/A 70% N/A30% N/A 30% N/A
In-Network Out-of-Network In-Network Out-of-Network
$1,000 N/A $1,000 N/A$2,000 N/A $2,000 N/A
In-Network Out-of-Network In-Network Out-of-Network
$6,600 N/A $6,600 N/A$13,200 N/A $13,200 N/A
Elective Abortion
Prescription Formulary
$2,271.14 $27,253.68 $2,300.17 $27,602.04
$29.03 $348.36
Included
$40
Included
$ Change from Current% Change from Current 1.28%
Monthly / Annual Premium
Specialist Visit
EE Coinsurance Liability
EE True Out of Pocket Max:
Single
Office Visit $20
$40$80
20% ($200 Maximum)
Preferred Brand $40
Non-Preferred Specialty
$4 or $15
Non-Preferred Brand
20% ($300 Maximum)
$80
SingleFamily
30% after Deductible 30% after Deductible
Urgent Care $50 $50
Hospital Admission
$150 $150Emergency Room
Embedded Coinsurance Max:
Renewal Option - GoldBCN HMO 2000
Current PlanBCN HMO 2000
(Current Billed Ages)
Generic
20% ($300 Maximum)
Pediatric Dental
Preferred Specialty 20% ($200 Maximum)
Medical Riders:
Imaging $150 after Deductible $150 after Deductible
IncludedIncluded
Employee RX Copay:
$20
Family
In-Network Employee Copay:
Coinsurance Percentage:
Carrier Coinsurance Liability
$40
Medical Policy #:
Employee Deductible:
Renewal Date: 9 / 1 / 2016
SingleFamily
Custom Select Custom Select
$4 or $15
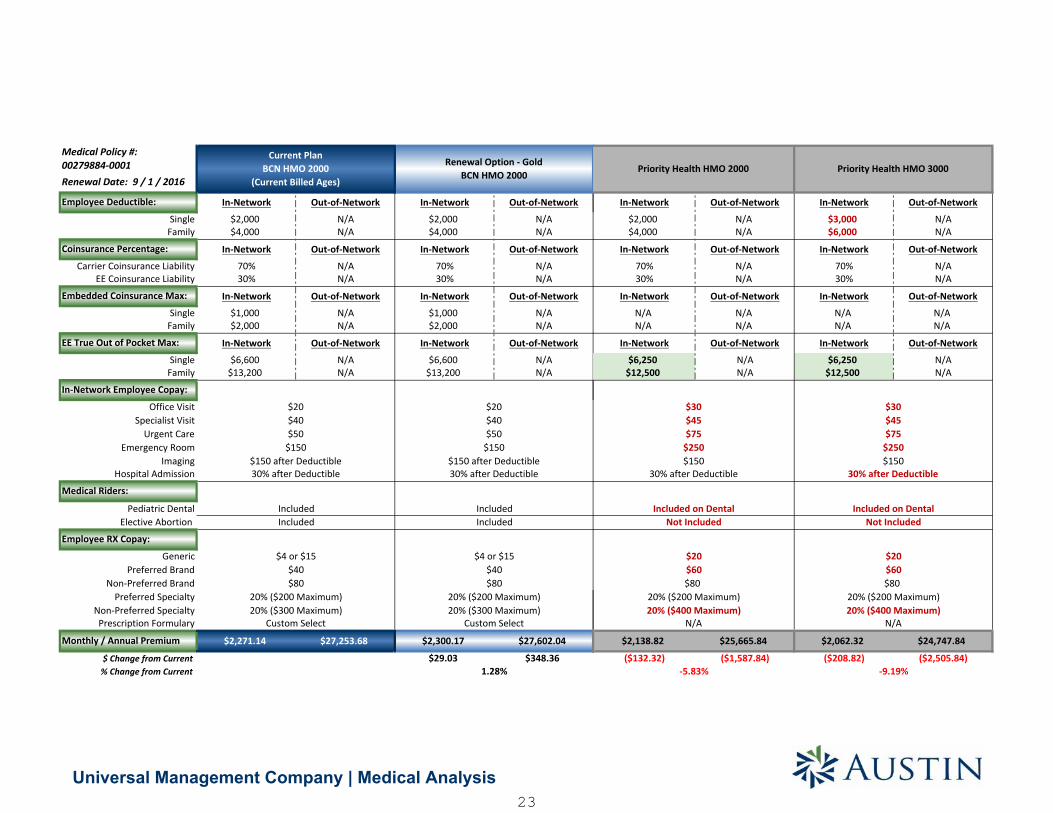
In-Network Out-of-Network In-Network Out-of-Network
$2,000 N/A $3,000 N/A$4,000 N/A $6,000 N/A
In-Network Out-of-Network In-Network Out-of-Network
70% N/A 70% N/A30% N/A 30% N/A
In-Network Out-of-Network In-Network Out-of-Network
N/A N/A N/A N/AN/A N/A N/A N/A
In-Network Out-of-Network In-Network Out-of-Network
$6,250 N/A $6,250 N/A$12,500 N/A $12,500 N/A
$2,138.82 $25,665.84 $2,062.32 $24,747.84
($132.32) ($1,587.84) ($208.82) ($2,505.84)
Priority Health HMO 2000 Priority Health HMO 3000
$30$45$75
$30
$250$150
30% after Deductible
Included on DentalNot Included
$20$60$80
$60$80
20% ($200 Maximum)20% ($400 Maximum)
N/A
-5.83%
$45$75
$250$150
30% after Deductible
Included on DentalNot Included
$20
20% ($200 Maximum)20% ($400 Maximum)
N/A
-9.19%
Universal Management Company | Medical Analysis23

00279884-0001
In-Network Out-of-Network In-Network Out-of-Network
$2,000 N/A $2,000 N/A$4,000 N/A $4,000 N/A
In-Network Out-of-Network In-Network Out-of-Network
70% N/A 70% N/A30% N/A 30% N/A
In-Network Out-of-Network In-Network Out-of-Network
$1,000 N/A $1,000 N/A$2,000 N/A $2,000 N/A
In-Network Out-of-Network In-Network Out-of-Network
$6,600 N/A $6,600 N/A$13,200 N/A $13,200 N/A
Elective Abortion
Prescription Formulary
$2,271.14 $27,253.68 $2,300.17 $27,602.04
$29.03 $348.36
Included
$40
Included
$ Change from Current% Change from Current 1.28%
Monthly / Annual Premium
Specialist Visit
EE Coinsurance Liability
EE True Out of Pocket Max:
Single
Office Visit $20
$40$80
20% ($200 Maximum)
Preferred Brand $40
Non-Preferred Specialty
$4 or $15
Non-Preferred Brand
20% ($300 Maximum)
$80
SingleFamily
30% after Deductible 30% after Deductible
Urgent Care $50 $50
Hospital Admission
$150 $150Emergency Room
Embedded Coinsurance Max:
Renewal Option - GoldBCN HMO 2000
Current PlanBCN HMO 2000
(Current Billed Ages)
Generic
20% ($300 Maximum)
Pediatric Dental
Preferred Specialty 20% ($200 Maximum)
Medical Riders:
Imaging $150 after Deductible $150 after Deductible
IncludedIncluded
Employee RX Copay:
$20
Family
In-Network Employee Copay:
Coinsurance Percentage:
Carrier Coinsurance Liability
$40
Medical Policy #:
Employee Deductible:
Renewal Date: 9 / 1 / 2016
SingleFamily
Custom Select Custom Select
$4 or $15
In-Network Out-of-Network In-Network Out-of-Network
$2,000 N/A $3,550 N/A$4,000 N/A $7,100 N/A
In-Network Out-of-Network In-Network Out-of-Network
70% N/A 50% N/A30% N/A 50% N/A
In-Network Out-of-Network In-Network Out-of-Network
N/A N/A N/A N/AN/A N/A N/A N/A
In-Network Out-of-Network In-Network Out-of-Network
$5,000 N/A $6,550 N/A$10,000 N/A $13,100 N/A
$1,986.46 $23,837.52 $1,720.21 $20,642.52
($284.68) ($3,416.16) ($550.93) ($6,611.16)
30% after Deductible
Included on Dental
30% after Deductible30% after Deductible30% after Deductible30% after Deductible30% after Deductible
-12.53%
Priority Health HSA HMO $3550
50% after Deductible50% after Deductible50% after Deductible50% after Deductible50% after Deductible50% after Deductible
Included on DentalNot Included
Rx copays after Deductible
$20$75
$10020% ($200 Maximum)20% ($400 Maximum)
N/A
-24.26%
Not Included
Rx Copays After Deductible
$20$60$80
20% ($200 Maximum)20% ($400 Maximum)
N/A
Priority Health HMO HSA 2000
Universal Management Company | Medical Analysis24
00279884-0001
In-Network Out-of-Network In-Network Out-of-Network
$2,000 N/A $2,000 N/A$4,000 N/A $4,000 N/A
In-Network Out-of-Network In-Network Out-of-Network
70% N/A 70% N/A30% N/A 30% N/A
In-Network Out-of-Network In-Network Out-of-Network
$1,000 N/A $1,000 N/A$2,000 N/A $2,000 N/A
In-Network Out-of-Network In-Network Out-of-Network
$6,600 N/A $6,600 N/A$13,200 N/A $13,200 N/A
Elective Abortion
Prescription Formulary
$2,271.14 $27,253.68 $2,300.17 $27,602.04
$29.03 $348.36
Included
$40
Included
$ Change from Current% Change from Current 1.28%
Monthly / Annual Premium
Specialist Visit
EE Coinsurance Liability
EE True Out of Pocket Max:
Single
Office Visit $20
$40$80
20% ($200 Maximum)
Preferred Brand $40
Non-Preferred Specialty
$4 or $15
Non-Preferred Brand
20% ($300 Maximum)
$80
SingleFamily
30% after Deductible 30% after Deductible
Urgent Care $50 $50
Hospital Admission
$150 $150Emergency Room
Embedded Coinsurance Max:
Renewal Option - GoldBCN HMO 2000
Current PlanBCN HMO 2000
(Current Billed Ages)
Generic
20% ($300 Maximum)
Pediatric Dental
Preferred Specialty 20% ($200 Maximum)
Medical Riders:
Imaging $150 after Deductible $150 after Deductible
IncludedIncluded
Employee RX Copay:
$20
Family
In-Network Employee Copay:
Coinsurance Percentage:
Carrier Coinsurance Liability
$40
Medical Policy #:
Employee Deductible:
Renewal Date: 9 / 1 / 2016
SingleFamily
Custom Select Custom Select
$4 or $15
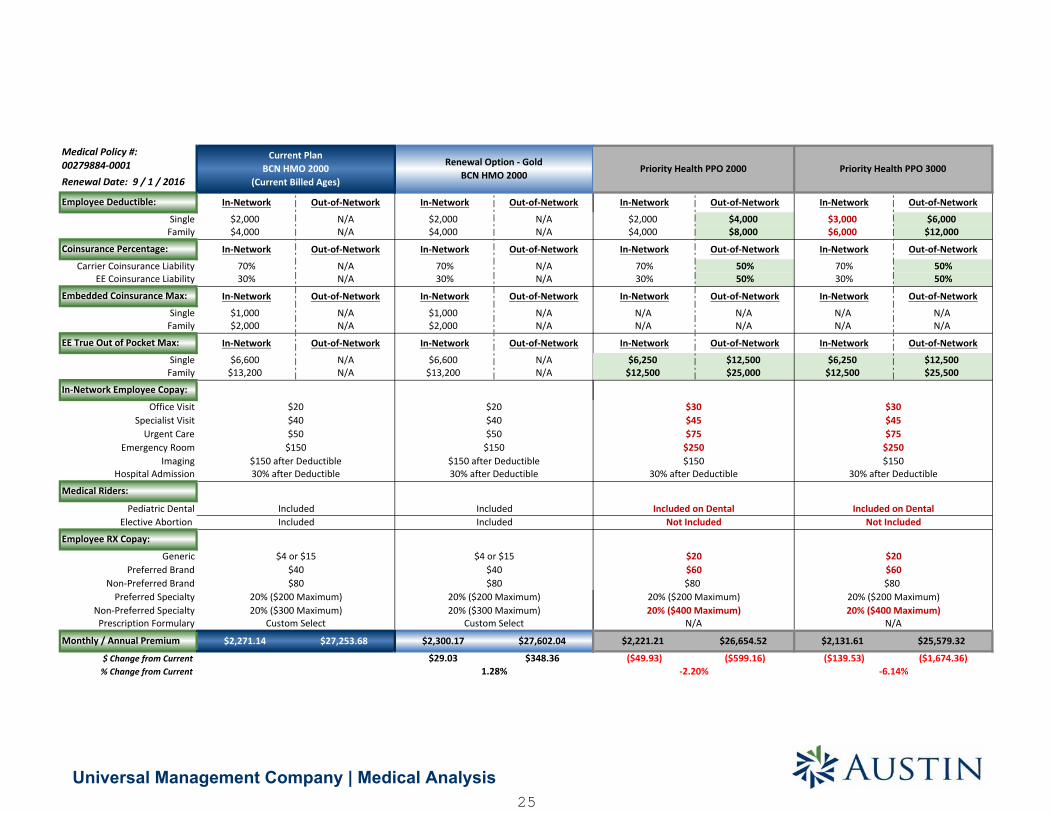
In-Network Out-of-Network In-Network Out-of-Network
$2,000 $4,000 $3,000 $6,000$4,000 $8,000 $6,000 $12,000
In-Network Out-of-Network In-Network Out-of-Network
70% 50% 70% 50%30% 50% 30% 50%
In-Network Out-of-Network In-Network Out-of-Network
N/A N/A N/A N/AN/A N/A N/A N/A
In-Network Out-of-Network In-Network Out-of-Network
$6,250 $12,500 $6,250 $12,500$12,500 $25,000 $12,500 $25,500
$2,221.21 $26,654.52 $2,131.61 $25,579.32
($49.93) ($599.16) ($139.53) ($1,674.36)
Priority Health PPO 2000
$30$45$75
$250$150
30% after Deductible
Included on DentalNot Included
$20
$80$60
20% ($400 Maximum)N/A
20% ($200 Maximum)
N/A
-2.20% -6.14%
Priority Health PPO 3000
$30$45$75
$250$150
30% after Deductible
Included on DentalNot Included
$20$60$80
20% ($200 Maximum)20% ($400 Maximum)
Universal Management Company | Medical Analysis25
00279884-0001
In-Network Out-of-Network In-Network Out-of-Network
$2,000 N/A $2,000 N/A$4,000 N/A $4,000 N/A
In-Network Out-of-Network In-Network Out-of-Network
70% N/A 70% N/A30% N/A 30% N/A
In-Network Out-of-Network In-Network Out-of-Network
$1,000 N/A $1,000 N/A$2,000 N/A $2,000 N/A
In-Network Out-of-Network In-Network Out-of-Network
$6,600 N/A $6,600 N/A$13,200 N/A $13,200 N/A
Elective Abortion
Prescription Formulary
$2,271.14 $27,253.68 $2,300.17 $27,602.04
$29.03 $348.36
Included
$40
Included
$ Change from Current% Change from Current 1.28%
Monthly / Annual Premium
Specialist Visit
EE Coinsurance Liability
EE True Out of Pocket Max:
Single
Office Visit $20
$40$80
20% ($200 Maximum)
Preferred Brand $40
Non-Preferred Specialty
$4 or $15
Non-Preferred Brand
20% ($300 Maximum)
$80
SingleFamily
30% after Deductible 30% after Deductible
Urgent Care $50 $50
Hospital Admission
$150 $150Emergency Room
Embedded Coinsurance Max:
Renewal Option - GoldBCN HMO 2000
Current PlanBCN HMO 2000
(Current Billed Ages)
Generic
20% ($300 Maximum)
Pediatric Dental
Preferred Specialty 20% ($200 Maximum)
Medical Riders:
Imaging $150 after Deductible $150 after Deductible
IncludedIncluded
Employee RX Copay:
$20
Family
In-Network Employee Copay:
Coinsurance Percentage:
Carrier Coinsurance Liability
$40
Medical Policy #:
Employee Deductible:
Renewal Date: 9 / 1 / 2016
SingleFamily
Custom Select Custom Select
$4 or $15
In-Network Out-of-Network In-Network Out-of-Network
$2,000 $4,000 $3,550 $7,100$4,000 $8,000 $7,100 $14,200
In-Network Out-of-Network In-Network Out-of-Network
70% 50% 50% 40%30% 50% 50% 40%
In-Network Out-of-Network In-Network Out-of-Network
N/A N/A N/A N/AN/A N/A N/A N/A
In-Network Out-of-Network In-Network Out-of-Network
$5,000 $10,000 $6,550 $13,100$10,000 $20,000 $13,100 $26,200
$2,114.47 $25,373.64 $1,786.70 $21,440.40
($156.67) ($1,880.04) ($484.44) ($5,813.28)
Included on DentalNot Included
Rx Copays After Deductible
$20$60$80
20% ($200 Maximum)20% ($400 Maximum)
30% after Deductible30% after Deductible30% after Deductible30% after Deductible
N/A
-6.90%
Priority Health HSA PPO $3550
50% after Deductible50% after Deductible50% after Deductible50% after Deductible50% after Deductible50% after Deductible
Included on DentalNot Included
Rx copays after Deductible
$20$75
$10020% ($200 Maximum)20% ($400 Maximum)
-21.33%
Priority Health PPO HSA 2000
30% after Deductible30% after Deductible
Universal Management Company | Medical Analysis26

1) Employee headcounts obtained from May 2016 census.2) Final premium cost subject to change based on employee enrollment.3) Medical plan premiums shown above exclude Pediatric Dental EHBs and may increase if a ACA Compliant Dental plan is NOT purchased.4) The benefits shown in this section are not an insurance contract. The information provided is for illustrative purposes only. Please refer to the contractfor the exact description and details.5) The Embedded Coinsurance Maximum excludes the deductible, office visit copay, prescription drug copays and private duty nursing coinsurance.
HMO Plan Disclaimers
Benefit Improvements Benefit Reductions
Universal Management Company | Medical Analysis27
DENTAL PLAN OPTIONS
SMART BENEFIT SOLUTIONS
28

Universal Management Company | Dental Analysis
$0.00
$500.00
$1,000.00
$1,500.00
$2,000.00
$2,500.00
$3,000.00
Principal 100/75/50 Ameritas 100/75/50 Guardain 100/75/50 Principal Plan 2100/80/50
Ameritas Plan 2100/80/50
Delta Dental100/80/50
Guardian Plan 2100/80/50
29
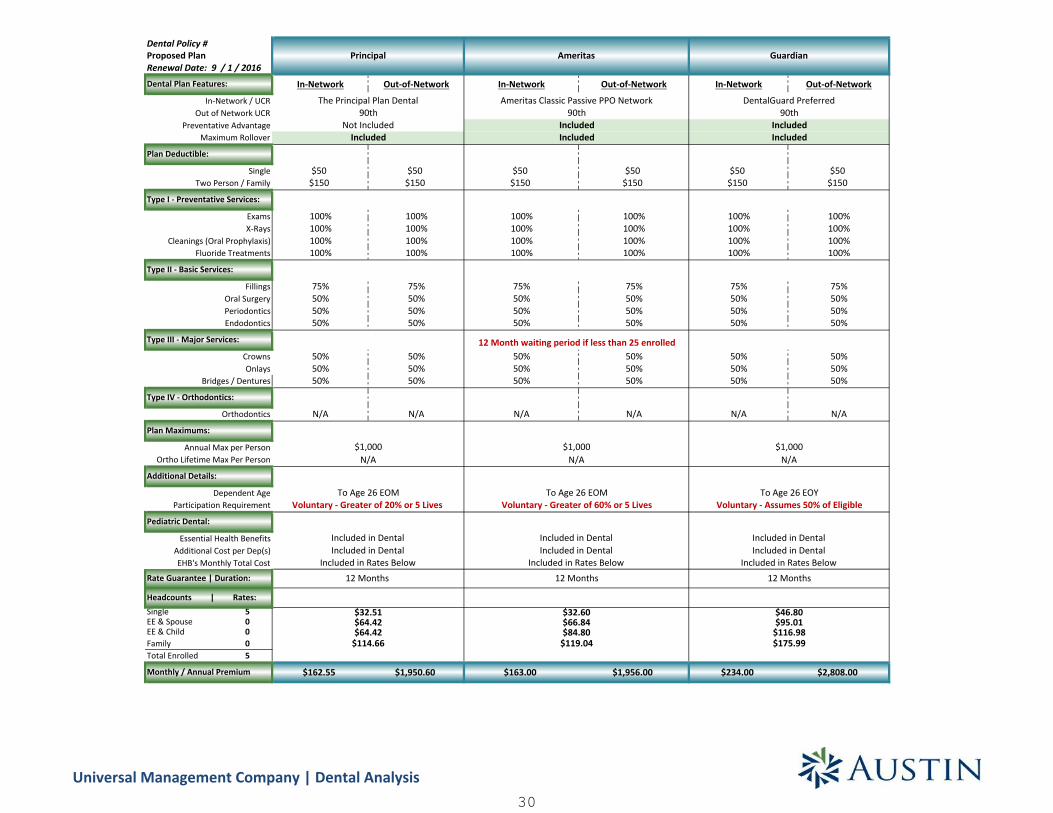
Dental Policy #
In-Network Out-of-Network In-Network Out-of-Network In-Network Out-of-Network
$50 $50 $50 $50 $50 $50$150 $150 $150 $150 $150 $150
100% 100% 100% 100% 100% 100%100% 100% 100% 100% 100% 100%100% 100% 100% 100% 100% 100%100% 100% 100% 100% 100% 100%
75% 75% 75% 75% 75% 75%50% 50% 50% 50% 50% 50%50% 50% 50% 50% 50% 50%50% 50% 50% 50% 50% 50%
50% 50% 50% 50% 50% 50%50% 50% 50% 50% 50% 50%50% 50% 50% 50% 50% 50%
N/A N/A N/A N/A N/A N/A
Single 5EE & Spouse 0EE & Child 0Family 0Total Enrolled 5
$162.55 $1,950.60 $163.00 $1,956.00 $234.00 $2,808.00
$1,000N/A
To Age 26 EOMVoluntary - Greater of 20% or 5 Lives
Included in DentalIncluded in Dental
Included in Rates Below
Principal
The Principal Plan Dental90th
Not IncludedIncluded
$1,000N/A
To Age 26 EOMVoluntary - Greater of 60% or 5 Lives
Included in DentalIncluded in Dental
Included in Rates Below
Ameritas
Ameritas Classic Passive PPO Network90th
IncludedIncluded
12 Month waiting period if less than 25 enrolled
Rate Guarantee | Duration:
Annual Max per Person
Included in Dental
12 MonthsIncluded in Rates BelowEHB's Monthly Total Cost
Headcounts | Rates:
Monthly / Annual Premium
$32.60$66.84$84.80
$119.04
12 Months12 Months
$32.51$64.42$64.42
$114.66
Onlays
Orthodontics
Ortho Lifetime Max Per Person
Pediatric Dental:
Additional Cost per Dep(s)Essential Health Benefits
X-Rays
Fluoride TreatmentsCleanings (Oral Prophylaxis)
FillingsOral SurgeryPeriodontics
Participation RequirementDependent Age
Additional Details:
Plan Maximums:
Crowns
Renewal Date: 9 / 1 / 2016
Plan Deductible:
Proposed Plan
Dental Plan Features:
Type IV - Orthodontics:
Bridges / Dentures
In-Network / UCR
Endodontics
Type III - Major Services:
Type I - Preventative Services:
Exams
Type II - Basic Services:
Preventative AdvantageOut of Network UCR
Maximum Rollover
SingleTwo Person / Family
Guardian
DentalGuard Preferred90th
IncludedIncluded
$46.80$95.01
$116.98$175.99
$1,000N/A
To Age 26 EOYVoluntary - Assumes 50% of Eligible
Included in Dental
Universal Management Company | Dental Analysis30

Dental Policy #
Single 5EE & Spouse 0EE & Child 0Family 0Total Enrolled 5
Rate Guarantee | Duration:
Annual Max per Person
EHB's Monthly Total Cost
Headcounts | Rates:
Monthly / Annual Premium
Onlays
Orthodontics
Ortho Lifetime Max Per Person
Pediatric Dental:
Additional Cost per Dep(s)Essential Health Benefits
X-Rays
Fluoride TreatmentsCleanings (Oral Prophylaxis)
FillingsOral SurgeryPeriodontics
Participation RequirementDependent Age
Additional Details:
Plan Maximums:
Crowns
Renewal Date: 9 / 1 / 2016
Plan Deductible:
Proposed Plan
Dental Plan Features:
Type IV - Orthodontics:
Bridges / Dentures
In-Network / UCR
Endodontics
Type III - Major Services:
Type I - Preventative Services:
Exams
Type II - Basic Services:
Preventative AdvantageOut of Network UCR
Maximum Rollover
SingleTwo Person / Family
In-Network Out-of-Network In-Network Out-of-Network Delta PPO Premier Nonparticipating In-Network Out-of-Network
$50 $50 $50 $50 $50 $50$150 $150 $150 $150 $150 $150
100% 100% 100% 100% 100% 80% 80% 100% 100%100% 100% 100% 100% 100% 80% 80% 100% 100%100% 100% 100% 100% 100% 80% 80% 100% 100%100% 100% 100% 100% 100% 80% 80% 100% 100%
80% 80% 80% 80% 80% 60% 60% 80% 80%50% 50% 50% 50% 50% 50% 50% 50% 50%50% 50% 50% 50% 50% 50% 50% 50% 50%50% 50% 50% 50% 50% 50% 50% 50% 50%
50% 50% 50% 50% 50% 50% 50% 50% 50%50% 50% 50% 50% 50% 50% 50% 50% 50%50% 50% 50% 50% 50% 50% 50% 50% 50%
N/A N/A N/A N/A N/A N/A N/A N/A N/A
$165.10 $1,981.20 $165.20 $1,982.40 $193.80 $2,325.60 $237.75 $2,853.00
Principal
The Principal Plan Dental90th
IncludedIncluded
Delta Dental PPO | PremierOut of Network Fee Schedule
Not Included
12 Months 12 Months12 Months
Not IncludedIncluded
$1,000N/A N/A
Included in Rates Below
$1,000
Ameritas Classic Passive PPO Network90th
GuardianAmeritasDelta Dental
(Plan A - Area 1 Standard)
Included in DentalIncluded in Dental
Included in Rates Below
$1,000
$65.38
$75 Per Person
12 Months
Included in Dental
To Age 26 EOM
$1,000
Included in Rates Below
Voluntary - 50% of Eligible
Included in DentalIncluded in Rates Below
To Age 26 EOMVoluntary - Greater of 20% or 5 Lives
Included in DentalIncluded in Dental
Voluntary - Greater of 60% or 5 Lives
Included in DentalIncluded in Dental
$38.76$71.74
$120.84$71.74
$123.67 $179.28
$47.55$96.52
$119.27
Not Included
N/A N/A
To Age 26 EOYVoluntary - Assumes 50% of Eligible
To Age 26 EOY
DentalGuard Preferred90th
IncludedIncluded
12 month waiting period for new enrollees12 Month waiting period if less than 25 enrolled
$65.38$116.40
$33.02 $33.04$67.68$86.20
Universal Management Company | Dental Analysis31

1) Employee headcounts obtained from May 2016 census.2) Rates are contingent on a packaged sale.3) Final premium cost subject to change based on employee enrollment (age banded rates only).4) Some carriers offer multi-product discounts, if you move a line of coverage it may increase cost to other lines if this discount is in place.5) If the pediatric essential health benefits are not included in the dental plan, the medical plan premium may increase. No one currently enrolled under age 19.6) Mutual of Omaha: Late Entrant Waiting Period for Type B, C and Ortho is 12 Months.7) MMA/MetLife: Late Entrant Waiting Period for Type B is 6 months (fillings)/12 months (other services), C and Ortho is 24 Months.8) Principal: Late Entrant Waiting Period for Type B is 6 months (fillings)/12 months (other services), C and Ortho is 24 Months.9) The benefits shown in this section are not an insurance contract. The information provided is for illustrative purposes only. Please refer to the contractfor the exact description and details.
Dental Plan Disclaimers
Benefit Improvements Benefit Reductions
Universal Management Company | Dental Analysis32

VISION PLAN OPTIONS
SMART BENEFIT SOLUTIONS
33
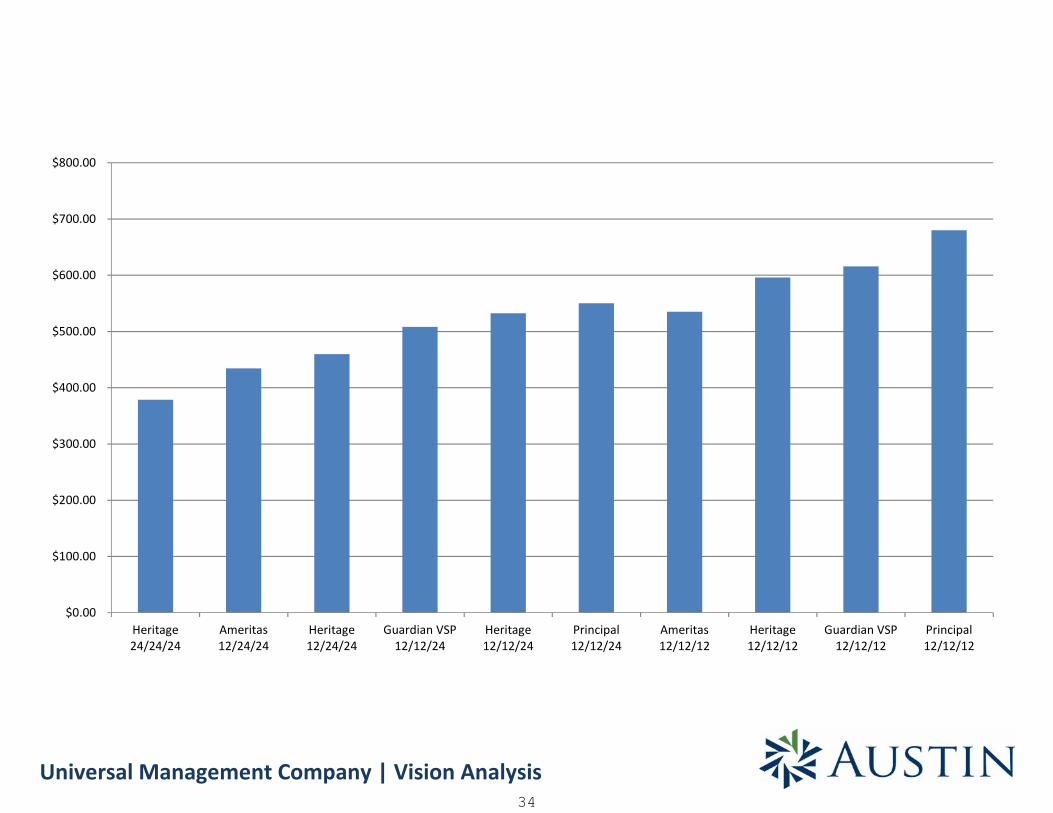
Universal Management Company | Vision Analysis
$0.00
$100.00
$200.00
$300.00
$400.00
$500.00
$600.00
$700.00
$800.00
Heritage24/24/24
Ameritas12/24/24
Heritage12/24/24
Guardian VSP12/12/24
Heritage12/12/24
Principal12/12/24
Ameritas12/12/12
Heritage12/12/12
Guardian VSP12/12/12
Principal12/12/12
34
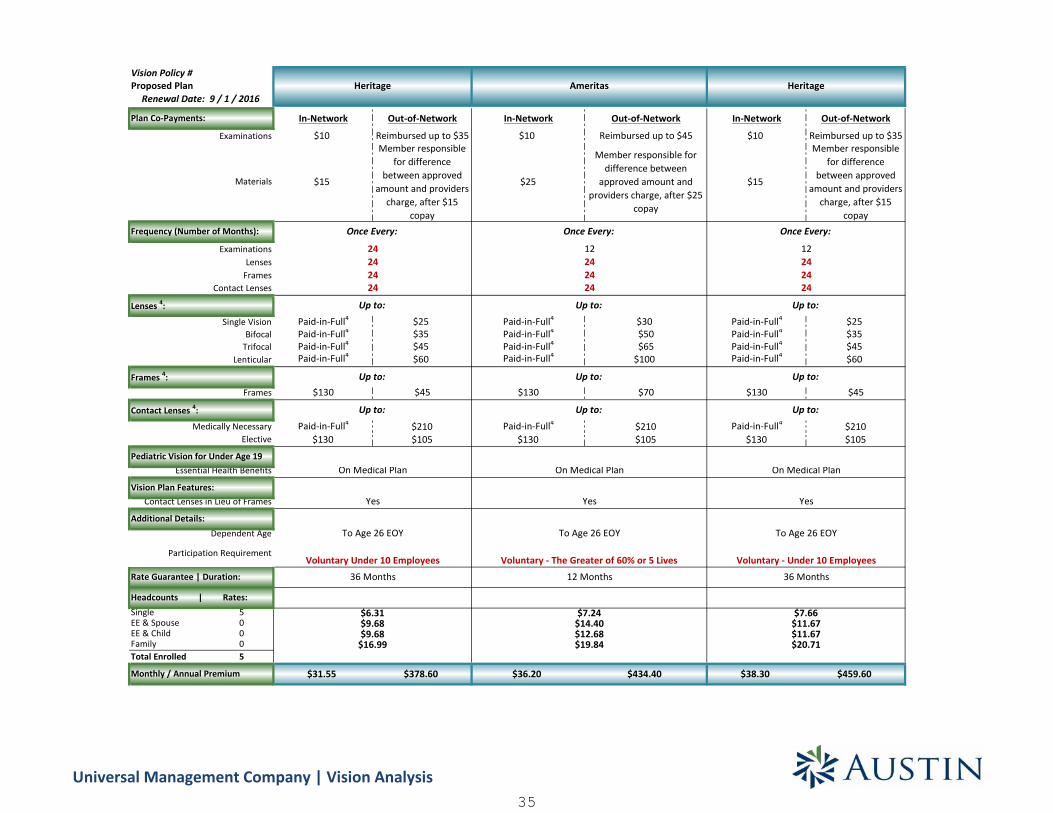
Vision Policy #
In-Network Out-of-Network In-Network Out-of-Network In-Network Out-of-Network
$10 Reimbursed up to $35 $10 Reimbursed up to $45 $10 Reimbursed up to $35
$15
Member responsiblefor difference
between approvedamount and providers
charge, after $15copay
$25
Member responsible fordifference between
approved amount andproviders charge, after $25
copay
$15
Member responsiblefor difference
between approvedamount and providers
charge, after $15copay
Paid-in-Full4 $25 Paid-in-Full4 $30 Paid-in-Full4 $25Paid-in-Full4 $35 Paid-in-Full4 $50 Paid-in-Full4 $35Paid-in-Full4 $45 Paid-in-Full4 $65 Paid-in-Full4 $45Paid-in-Full4 $60 Paid-in-Full4 $100 Paid-in-Full4 $60
$130 $45 $130 $70 $130 $45
Paid-in-Full4 $210 Paid-in-Full4 $210 Paid-in-Full4 $210$130 $105 $130 $105 $130 $105
Single 5EE & Spouse 0EE & Child 0Family 0Total Enrolled 5
$31.55 $378.60 $36.20 $434.40 $38.30 $459.60
$9.68$9.68
$16.99
$11.67$11.67$20.71
Heritage
Once Every:
24242424
Up to:
Up to:
Up to:
On Medical Plan
Yes
36 Months
On Medical Plan
Yes
To Age 26 EOY
Heritage
Once Every:
12242424
Up to:
Up to:
Up to:
12 Months
$7.24$14.40$12.68$19.84
On Medical Plan
Yes
To Age 26 EOY
Voluntary - The Greater of 60% or 5 Lives
Ameritas
Once Every:
12242424
Up to:
Up to:
Up to:
Monthly / Annual Premium
Headcounts | Rates:
$6.31 $7.66
Rate Guarantee | Duration: 36 Months
Participation Requirement
Dependent Age
Voluntary - Under 10 Employees
To Age 26 EOY
Voluntary Under 10 Employees
Additional Details:
Contact Lenses in Lieu of Frames
Elective
Vision Plan Features:
Pediatric Vision for Under Age 19Essential Health Benefits
Medically Necessary
ExaminationsLenses
Proposed Plan
Plan Co-Payments:
Examinations
Materials
Renewal Date: 9 / 1 / 2016
Contact Lenses 4:
Frames
Single Vision
Lenticular
Frequency (Number of Months):
FramesContact Lenses
Lenses 4:
BifocalTrifocal
Frames 4:
Universal Management Company | Vision Analysis35

Vision Policy #
Single 5EE & Spouse 0EE & Child 0Family 0Total Enrolled 5
Monthly / Annual Premium
Headcounts | Rates:
Rate Guarantee | Duration:
Participation Requirement
Dependent AgeAdditional Details:
Contact Lenses in Lieu of Frames
Elective
Vision Plan Features:
Pediatric Vision for Under Age 19Essential Health Benefits
Medically Necessary
ExaminationsLenses
Proposed Plan
Plan Co-Payments:
Examinations
Materials
Renewal Date: 9 / 1 / 2016
Contact Lenses 4:
Frames
Single Vision
Lenticular
Frequency (Number of Months):
FramesContact Lenses
Lenses 4:
BifocalTrifocal
Frames 4:
In-Network Out-of-Network In-Network Out-of-Network In-Network Out-of-Network
$10 Reimbursed up to $39 $10 Reimbursed up to $35 $10 Reimbursed up to $45
$25
Member responsible fordifference between
approved amount andproviders charge, after
$25 copay
$15
Member responsiblefor difference
between approvedamount and providers
charge, after $15copay
$25
Member responsiblefor difference
between approvedamount and providers
charge, after $25copay
Paid-in-Full4 $23 Paid-in-Full4 $25 Paid-in-Full4 $30Paid-in-Full4 $37 Paid-in-Full4 $35 Paid-in-Full4 $50Paid-in-Full4 $49 Paid-in-Full4 $45 Paid-in-Full4 $65Paid-in-Full4 $64 Paid-in-Full4 $60 Paid-in-Full4 $100
$130 $46 $130 $45 $150 $70
Paid-in-Full4 $210 Paid-in-Full4 $210 Paid-in-Full4 $210$130 $100 $130 $105 $150 $105
$42.35 $508.20 $44.35 $532.20 $45.85 $550.20
Heritage
Once Every:
12122412
Up to:
Up to:
Up to:
On Medical Plan
Yes
To Age 26 EOY
$13.51$23.97
24 Months
On Medical Plan
Principal(VSP)
Once Every:
12122412
Up to:
Up to:
Up to:
$29.77
Yes
To Age 26 EOM
Voluntary - Greater of 20% or 5 Lives
$23.01
$8.47$14.26$14.54
$9.17$17.83$18.72
$8.87$13.51
12 Months36 MonthsVoluntary - Under 10 Employees
Guardian(VSP)
Once Every:
12122412
Up to:
Up to:
Up to:
On Medical Plan
Yes
To Age 26 EOYVoluntary
50% of elgible employees - Sold with Dental
Universal Management Company | Vision Analysis36
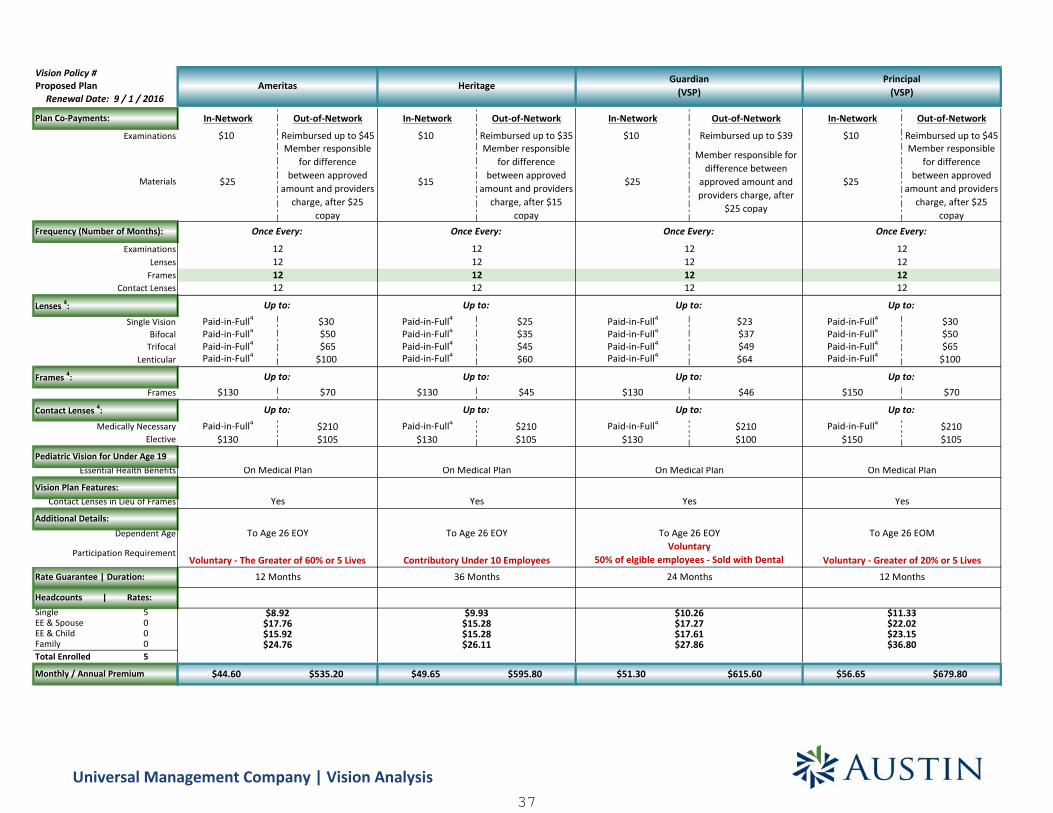
Vision Policy #
Single 5EE & Spouse 0EE & Child 0Family 0Total Enrolled 5
Monthly / Annual Premium
Headcounts | Rates:
Rate Guarantee | Duration:
Participation Requirement
Dependent AgeAdditional Details:
Contact Lenses in Lieu of Frames
Elective
Vision Plan Features:
Pediatric Vision for Under Age 19Essential Health Benefits
Medically Necessary
ExaminationsLenses
Proposed Plan
Plan Co-Payments:
Examinations
Materials
Renewal Date: 9 / 1 / 2016
Contact Lenses 4:
Frames
Single Vision
Lenticular
Frequency (Number of Months):
FramesContact Lenses
Lenses 4:
BifocalTrifocal
Frames 4:
In-Network Out-of-Network In-Network Out-of-Network In-Network Out-of-Network In-Network Out-of-Network
$10 Reimbursed up to $45 $10 Reimbursed up to $35 $10 Reimbursed up to $39 $10 Reimbursed up to $45
$25
Member responsiblefor difference
between approvedamount and providers
charge, after $25copay
$15
Member responsiblefor difference
between approvedamount and providers
charge, after $15copay
$25
Member responsible fordifference between
approved amount andproviders charge, after
$25 copay
$25
Member responsiblefor difference
between approvedamount and providers
charge, after $25copay
Paid-in-Full4 $30 Paid-in-Full4 $25 Paid-in-Full4 $23 Paid-in-Full4 $30Paid-in-Full4 $50 Paid-in-Full4 $35 Paid-in-Full4 $37 Paid-in-Full4 $50Paid-in-Full4 $65 Paid-in-Full4 $45 Paid-in-Full4 $49 Paid-in-Full4 $65Paid-in-Full4 $100 Paid-in-Full4 $60 Paid-in-Full4 $64 Paid-in-Full4 $100
$130 $70 $130 $45 $130 $46 $150 $70
Paid-in-Full4 $210 Paid-in-Full4 $210 Paid-in-Full4 $210 Paid-in-Full4 $210$130 $105 $130 $105 $130 $100 $150 $105
$44.60 $535.20 $49.65 $595.80 $51.30 $615.60 $56.65 $679.80
On Medical Plan
Yes
To Age 26 EOY
Contributory Under 10 Employees
Heritage
Once Every:
12121212
Up to:
Up to:
Up to:
Guardian(VSP)
24 Months
Once Every:
12121212
Up to:
Up to:
Up to:
Yes
To Age 26 EOYVoluntary
50% of elgible employees - Sold with Dental
$9.93$15.28$15.28$26.11 $27.86
$10.26$17.27$17.61
36 Months
On Medical Plan
Principal(VSP)
Once Every:
12121212
Up to:
Up to:
Up to:
On Medical Plan
Yes
To Age 26 EOM
Voluntary - Greater of 20% or 5 Lives12 Months
$11.33$22.02$23.15$36.80
Ameritas
Once Every:
12121212
Up to:
Up to:
Up to:
On Medical Plan
Yes
To Age 26 EOY
Voluntary - The Greater of 60% or 5 Lives12 Months
$8.92$17.76$15.92$24.76
Universal Management Company | Vision Analysis37
1) Employee headcounts obtained from May 2016 census.2) Rates are contingent on a packaged sale.3) Final premium cost subject to change based on employee enrollment (age banded rates only).4) Applicable copayments apply.5) Some carriers offer multi-product discounts, if you move a line of coverage it may increase cost to other lines if this discount is in place.6) The benefits shown in this section are not an insurance contract. The information provided is for illustrative purposes only. Please refer to the contractfor the exact description and details.
Vision Plan Disclaimers
Benefit Improvements Benefit Reductions
Universal Management Company | Vision Analysis38

BASIC LIFE PLAN OPTIONS
SMART BENEFIT SOLUTIONS
39
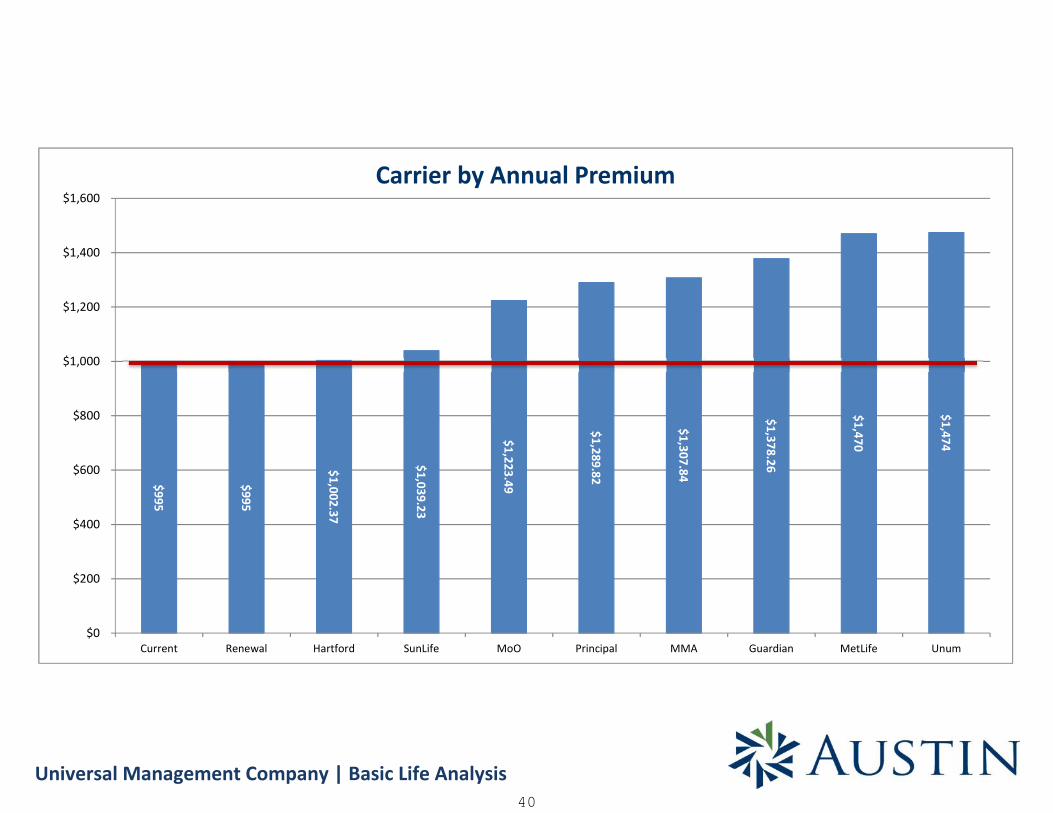
Universal Management Company | Basic Life Analysis
$995
$995
$1,002.37
$1,039.23
$1,223.49
$1,289.82
$1,307.84
$1,378.26
$1,470
$1,474
$0
$200
$400
$600
$800
$1,000
$1,200
$1,400
$1,600
Current Renewal Hartford SunLife MoO Principal MMA Guardian MetLife Unum
Carrier by Annual Premium
40

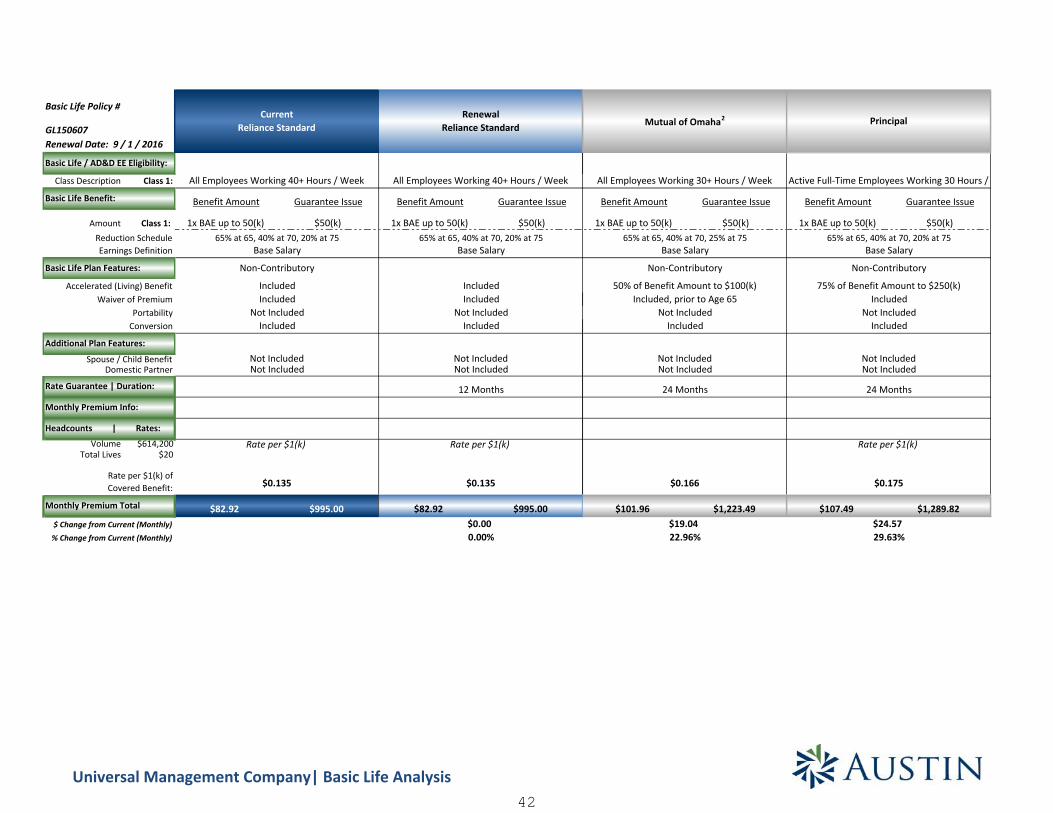
GL150607
Class Description Class 1:
Benefit Amount Guarantee Issue Benefit Amount Guarantee Issue Benefit Amount Guarantee Issue Benefit Amount Guarantee Issue
Amount Class 1: 1x BAE up to 50(k) $50(k) 1x BAE up to 50(k) $50(k) 1x BAE up to 50(k) $50(k) 1x BAE up to 50(k) $50(k)
Domestic Partner
Volume $614,200Total Lives $20
$82.92 $995.00 $82.92 $995.00 $83.53 $1,002.37 $86.60 $1,039.23
Rate per $1(k)
Not Included
75% of Benefit Amount to $500(k)
$0.136
$3.69
Rate per $1(k)
$0.141
SunLife2
Included, prior to Age 65IncludedIncluded
Not Included
Non-Contributory
All Employees Working 40+ Hours / Week
Basic Life Plan Features:
Reduction Schedule
Basic Life / AD&D EE Eligibility:
65% at 65, 40% at 70, 20% at 75
All Employees Working 40+ Hours / Week All Employees Working 40+ Hours / Week
Accelerated (Living) Benefit
Basic Life Policy #
Earnings Definition
Additional Plan Features:
IncludedConversion
Waiver of PremiumIncludedIncluded
Rate Guarantee | Duration:
Renewal Date: 9 / 1 / 2016
CurrentReliance Standard
Spouse / Child BenefitNot Included
Base Salary
Basic Life Benefit:
Not Included
Monthly Premium Info:
Not Included
IncludedPortability Not Included
Not IncludedNot Included
24 Months
$0.135 $0.135
% Change from Current (Monthly)
Monthly Premium Total
$ Change from Current (Monthly)0.00%
Rate per $1(k) ofCovered Benefit:
Rate per $1(k)
$0.00
Included, prior to Age 60
Base Salary65% at 65, 40% at 70, 20% at 75
80% of Benefit Amount to $250(k)
Non-Contributory
Active Full-Time Employees Working 30 Hours /
65% at 65, 50% at 70Base Salary
Non-Contributory
Base Salary65% at 65, 40% at 70, 20% at 75
Included
Rate per $1(k)
12 Months
Included
Headcounts | Rates:
RenewalReliance Standard
Hartford
IncludedIncluded
Not IncludedNot Included
24 Months
4.44%$0.610.74%
Universal Management Company| Basic Life Analysis41
GL150607
Class Description Class 1:
Benefit Amount Guarantee Issue Benefit Amount Guarantee Issue
Amount Class 1: 1x BAE up to 50(k) $50(k) 1x BAE up to 50(k) $50(k)
Domestic Partner
Volume $614,200Total Lives $20
$82.92 $995.00 $82.92 $995.00
Basic Life Plan Features:
Reduction Schedule
Basic Life / AD&D EE Eligibility:
65% at 65, 40% at 70, 20% at 75
All Employees Working 40+ Hours / Week All Employees Working 40+ Hours / Week
Accelerated (Living) Benefit
Basic Life Policy #
Earnings Definition
Additional Plan Features:
IncludedConversion
Waiver of PremiumIncludedIncluded
Rate Guarantee | Duration:
Renewal Date: 9 / 1 / 2016
CurrentReliance Standard
Spouse / Child BenefitNot Included
Base Salary
Basic Life Benefit:
Not Included
Monthly Premium Info:
Not Included
IncludedPortability Not Included
Not IncludedNot Included
$0.135 $0.135
% Change from Current (Monthly)
Monthly Premium Total
$ Change from Current (Monthly)0.00%
Rate per $1(k) ofCovered Benefit:
Rate per $1(k)
$0.00
Base Salary65% at 65, 40% at 70, 20% at 75
Non-Contributory
Included
Rate per $1(k)
12 Months
Included
Headcounts | Rates:
RenewalReliance Standard
Benefit Amount Guarantee Issue Benefit Amount Guarantee Issue
1x BAE up to 50(k) $50(k) 1x BAE up to 50(k) $50(k)
$101.96 $1,223.49 $107.49 $1,289.82
65% at 65, 40% at 70, 25% at 75Base Salary
Non-Contributory
Not Included
Not IncludedNot Included
Included
24 Months
Rate per $1(k)
Not Included
$19.0422.96%
$0.166
All Employees Working 30+ Hours / Week
Not Included
50% of Benefit Amount to $100(k)Included, prior to Age 65 Included
Mutual of Omaha2
75% of Benefit Amount to $250(k)
Base Salary
Included
Not Included
$0.175
24 Months
Principal
Active Full-Time Employees Working 30 Hours /
65% at 65, 40% at 70, 20% at 75
Non-Contributory
$24.5729.63%
Universal Management Company| Basic Life Analysis42

GL150607
Class Description Class 1:
Benefit Amount Guarantee Issue Benefit Amount Guarantee Issue
Amount Class 1: 1x BAE up to 50(k) $50(k) 1x BAE up to 50(k) $50(k)
Domestic Partner
Volume $614,200Total Lives $20
$82.92 $995.00 $82.92 $995.00
Basic Life Plan Features:
Reduction Schedule
Basic Life / AD&D EE Eligibility:
65% at 65, 40% at 70, 20% at 75
All Employees Working 40+ Hours / Week All Employees Working 40+ Hours / Week
Accelerated (Living) Benefit
Basic Life Policy #
Earnings Definition
Additional Plan Features:
IncludedConversion
Waiver of PremiumIncludedIncluded
Rate Guarantee | Duration:
Renewal Date: 9 / 1 / 2016
CurrentReliance Standard
Spouse / Child BenefitNot Included
Base Salary
Basic Life Benefit:
Not Included
Monthly Premium Info:
Not Included
IncludedPortability Not Included
Not IncludedNot Included
$0.135 $0.135
% Change from Current (Monthly)
Monthly Premium Total
$ Change from Current (Monthly)0.00%
Rate per $1(k) ofCovered Benefit:
Rate per $1(k)
$0.00
Base Salary65% at 65, 40% at 70, 20% at 75
Non-Contributory
Included
Rate per $1(k)
12 Months
Included
Headcounts | Rates:
RenewalReliance Standard
Benefit Amount Guarantee Issue Benefit Amount Guarantee Issue
1x BAE up to 50(k) $50(k) 1x BAE up to 50(k) $50(k)
$108.99 $1,307.84 $114.86 $1,378.26
31.44%
65% at 65, 50% at 70Base Salary
Included, prior to Age 60
$26.07
Not IncludedNot Included
21 Months (Renews June 1, 2018)
MMA2
($240 Mandatory Membership Fee)
Active Full-Time Employees Working 30 Hours /
80% to a Maximum of $500(k)
Rates Based on Package Sale
24 Months
Included
38.52%
Active Full-Time Employees Working 30 Hours /
Non-Contributory
65% at 65, 40% at 70, 20% at 75
Not Included
$31.94
Not IncludedNot Included
Included, prior to Age 65Included w/EOI
Guardian
Base Salary
Non-Contributory
75% to a Maximum of $250(k)
Included
Rate per $1(k)
$0.187
Rate per $1(k)
$0.154
Universal Management Company| Basic Life Analysis43
GL150607
Class Description Class 1:
Benefit Amount Guarantee Issue Benefit Amount Guarantee Issue
Amount Class 1: 1x BAE up to 50(k) $50(k) 1x BAE up to 50(k) $50(k)
Domestic Partner
Volume $614,200Total Lives $20
$82.92 $995.00 $82.92 $995.00
Basic Life Plan Features:
Reduction Schedule
Basic Life / AD&D EE Eligibility:
65% at 65, 40% at 70, 20% at 75
All Employees Working 40+ Hours / Week All Employees Working 40+ Hours / Week
Accelerated (Living) Benefit
Basic Life Policy #
Earnings Definition
Additional Plan Features:
IncludedConversion
Waiver of PremiumIncludedIncluded
Rate Guarantee | Duration:
Renewal Date: 9 / 1 / 2016
CurrentReliance Standard
Spouse / Child BenefitNot Included
Base Salary
Basic Life Benefit:
Not Included
Monthly Premium Info:
Not Included
IncludedPortability Not Included
Not IncludedNot Included
$0.135 $0.135
% Change from Current (Monthly)
Monthly Premium Total
$ Change from Current (Monthly)0.00%
Rate per $1(k) ofCovered Benefit:
Rate per $1(k)
$0.00
Base Salary65% at 65, 40% at 70, 20% at 75
Non-Contributory
Included
Rate per $1(k)
12 Months
Included
Headcounts | Rates:
RenewalReliance Standard
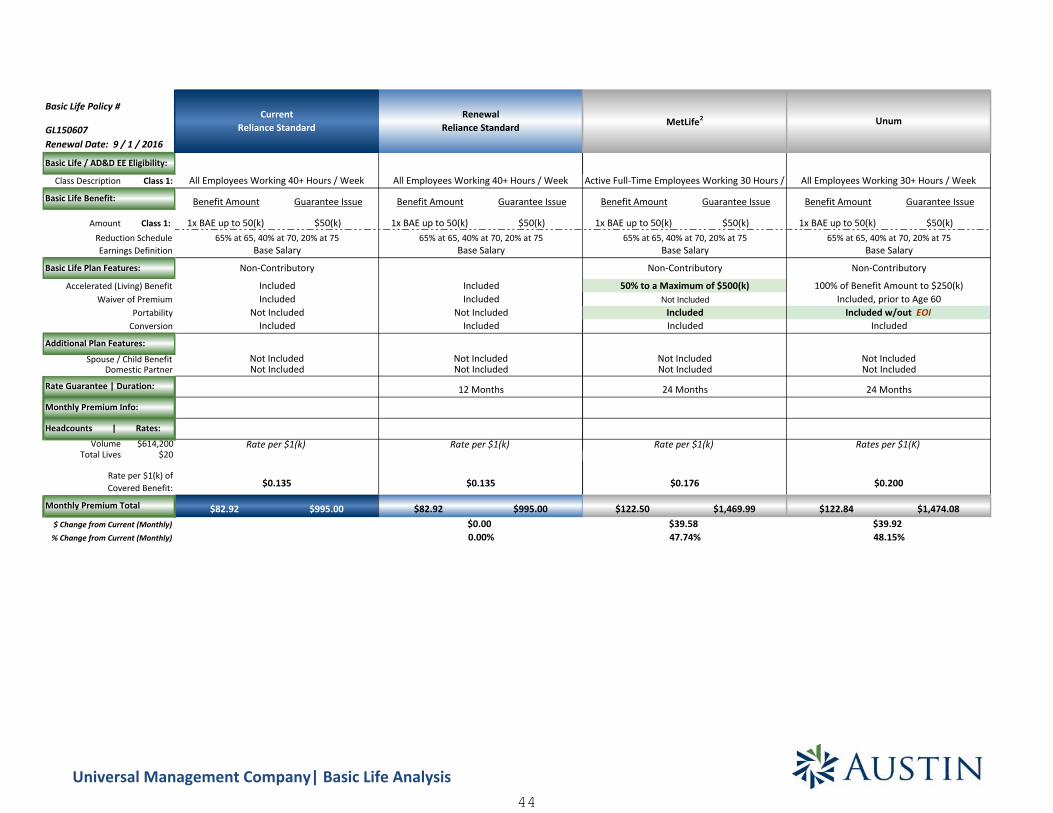
Benefit Amount Guarantee Issue Benefit Amount Guarantee Issue
1x BAE up to 50(k) $50(k) 1x BAE up to 50(k) $50(k)
$122.50 $1,469.99 $122.84 $1,474.08
$0.176
$39.5847.74%
Not IncludedNot Included
24 Months
MetLife2
Active Full-Time Employees Working 30 Hours /
65% at 65, 40% at 70, 20% at 75Base Salary
Non-Contributory
50% to a Maximum of $500(k)Not Included
IncludedIncluded
Rate per $1(k) Rates per $1(K)
24 Months
Not Included
Base Salary
All Employees Working 30+ Hours / Week
Not Included
$0.200
100% of Benefit Amount to $250(k)
Non-Contributory
65% at 65, 40% at 70, 20% at 75
48.15%$39.92
Unum
Included, prior to Age 60Included w/out EOI
Included
Universal Management Company| Basic Life Analysis44

1) Employee headcounts obtained from May 2016 census.2) Rates are contingent on a packaged sale.3) Some carriers offer multi-product discounts, if you move a line of coverage it may increase cost to other lines if this discount is in place.4) The benefits shown in this section are not an insurance contract. The information provided is for illustrative purposes only. Please refer to the contractfor the exact description and details.
Basic Life Plan Disclaimers
Benefit Improvements Benefit Reductions
Universal Management Company| Basic Life Analysis45

OPTIONAL LIFE PLAN OPTIONS
SMART BENEFIT SOLUTIONS
46
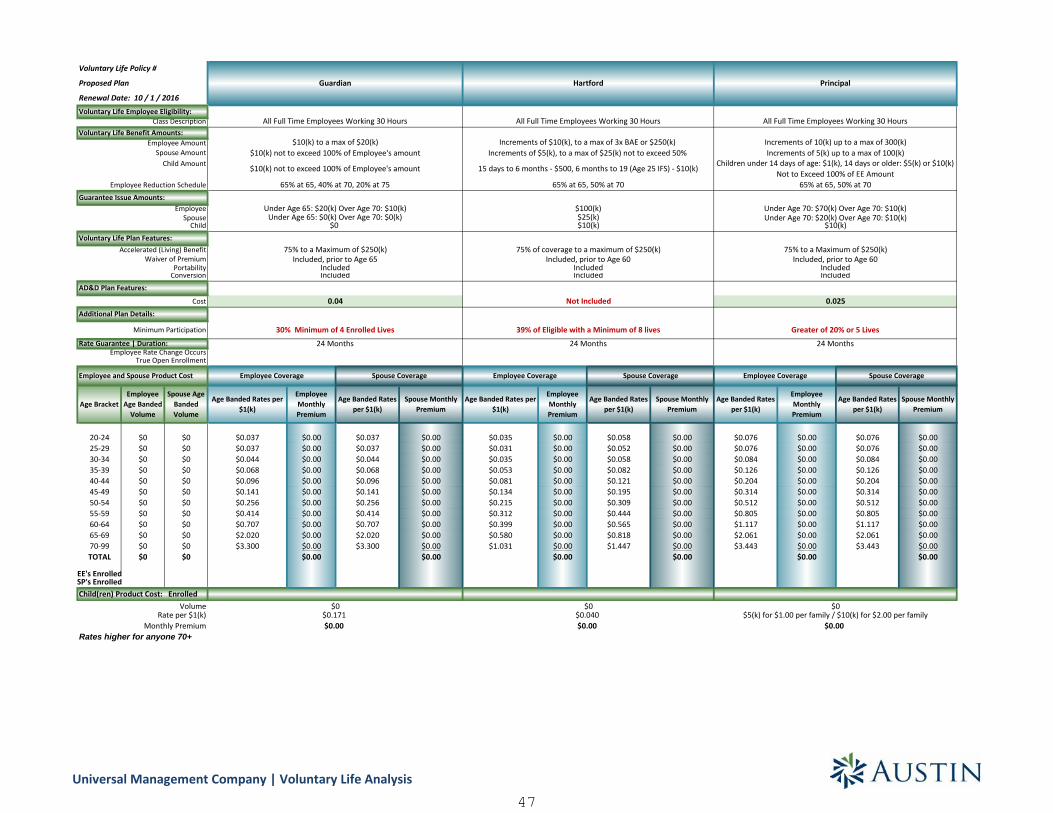
Proposed Plan
Renewal Date: 10 / 1 / 2016
Age BracketEmployee
Age BandedVolume
Spouse AgeBandedVolume
Age Banded Rates per$1(k)
EmployeeMonthlyPremium
Age Banded Ratesper $1(k)
Spouse MonthlyPremium
Age Banded Rates per$1(k)
EmployeeMonthlyPremium
Age Banded Ratesper $1(k)
Spouse MonthlyPremium
Age Banded Ratesper $1(k)
EmployeeMonthlyPremium
Age Banded Ratesper $1(k)
Spouse MonthlyPremium
20-24 $0 $0 $0.037 $0.00 $0.037 $0.00 $0.035 $0.00 $0.058 $0.00 $0.076 $0.00 $0.076 $0.0025-29 $0 $0 $0.037 $0.00 $0.037 $0.00 $0.031 $0.00 $0.052 $0.00 $0.076 $0.00 $0.076 $0.0030-34 $0 $0 $0.044 $0.00 $0.044 $0.00 $0.035 $0.00 $0.058 $0.00 $0.084 $0.00 $0.084 $0.0035-39 $0 $0 $0.068 $0.00 $0.068 $0.00 $0.053 $0.00 $0.082 $0.00 $0.126 $0.00 $0.126 $0.0040-44 $0 $0 $0.096 $0.00 $0.096 $0.00 $0.081 $0.00 $0.121 $0.00 $0.204 $0.00 $0.204 $0.0045-49 $0 $0 $0.141 $0.00 $0.141 $0.00 $0.134 $0.00 $0.195 $0.00 $0.314 $0.00 $0.314 $0.0050-54 $0 $0 $0.256 $0.00 $0.256 $0.00 $0.215 $0.00 $0.309 $0.00 $0.512 $0.00 $0.512 $0.0055-59 $0 $0 $0.414 $0.00 $0.414 $0.00 $0.312 $0.00 $0.444 $0.00 $0.805 $0.00 $0.805 $0.0060-64 $0 $0 $0.707 $0.00 $0.707 $0.00 $0.399 $0.00 $0.565 $0.00 $1.117 $0.00 $1.117 $0.0065-69 $0 $0 $2.020 $0.00 $2.020 $0.00 $0.580 $0.00 $0.818 $0.00 $2.061 $0.00 $2.061 $0.0070-99 $0 $0 $3.300 $0.00 $3.300 $0.00 $1.031 $0.00 $1.447 $0.00 $3.443 $0.00 $3.443 $0.00TOTAL $0 $0 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00
EE's EnrolledSP's Enrolled
Rates higher for anyone 70+
Spouse Coverage
$0$0.040$0.00
Not Included
39% of Eligible with a Minimum of 8 lives
24 Months
75% of coverage to a maximum of $250(k)Included, prior to Age 60
IncludedIncluded
Employee Coverage
Hartford
All Full Time Employees Working 30 Hours
Increments of $10(k), to a max of 3x BAE or $250(k)Increments of $5(k), to a max of $25(k) not to exceed 50%
15 days to 6 months - $500, 6 months to 19 (Age 25 IFS) - $10(k)
65% at 65, 50% at 70
$10(k) not to exceed 100% of Employee's amount
Employee Coverage Spouse Coverage
65% at 65, 50% at 70
Under Age 70: $20(k) Over Age 70: $10(k)$10(k)
Included
$0
$0.00
0.025
Greater of 20% or 5 Lives
24 Months
$0$5(k) for $1.00 per family / $10(k) for $2.00 per family
$10(k)
75% to a Maximum of $250(k)Included, prior to Age 60
Under Age 70: $70(k) Over Age 70: $10(k)$100(k)$25(k)
IncludedIncluded
All Full Time Employees Working 30 Hours
Increments of 10(k) up to a max of 300(k)Increments of 5(k) up to a max of 100(k)
Children under 14 days of age: $1(k), 14 days or older: $5(k) or $10(k)Not to Exceed 100% of EE Amount
Under Age 65: $20(k) Over Age 70: $10(k)Under Age 65: $0(k) Over Age 70: $0(k)
Monthly Premium
VolumeRate per $1(k)
Employee Rate Change Occurs
Employee and Spouse Product Cost
Cost
Child(ren) Product Cost: Enrolled
Rate Guarantee | Duration:
Additional Plan Details:
True Open Enrollment
AD&D Plan Features:
75% to a Maximum of $250(k)
24 Months
IncludedPortability
Voluntary Life Employee Eligibility:Class Description
Employee AmountSpouse Amount
Child
Guarantee Issue Amounts:
Child Amount
Employee Reduction Schedule
Spouse Employee
Voluntary Life Benefit Amounts:
30% Minimum of 4 Enrolled LivesMinimum Participation
$10(k) not to exceed 100% of Employee's amount
Conversion
Voluntary Life Plan Features:
Waiver of PremiumAccelerated (Living) Benefit
$0.00
All Full Time Employees Working 30 Hours
Employee Coverage Spouse Coverage
$10(k) to a max of $20(k)
$0.171$0
Included, prior to Age 65
65% at 65, 40% at 70, 20% at 75
0.04
Principal
Voluntary Life Policy #
Guardian
Universal Management Company | Voluntary Life Analysis
47

Proposed Plan
Renewal Date: 10 / 1 / 2016
Age BracketEmployee
Age BandedVolume
Spouse AgeBandedVolume
20-24 $0 $025-29 $0 $030-34 $0 $035-39 $0 $040-44 $0 $045-49 $0 $050-54 $0 $055-59 $0 $060-64 $0 $065-69 $0 $070-99 $0 $0TOTAL $0 $0
EE's EnrolledSP's Enrolled
Rates higher for anyone 70+Monthly Premium
VolumeRate per $1(k)
Employee Rate Change Occurs
Employee and Spouse Product Cost
Cost
Child(ren) Product Cost: Enrolled
Rate Guarantee | Duration:
Additional Plan Details:
True Open Enrollment
AD&D Plan Features:
Portability
Voluntary Life Employee Eligibility:Class Description
Employee AmountSpouse Amount
Child
Guarantee Issue Amounts:
Child Amount
Employee Reduction Schedule
Spouse Employee
Voluntary Life Benefit Amounts:
Minimum Participation
Conversion
Voluntary Life Plan Features:
Waiver of PremiumAccelerated (Living) Benefit
Voluntary Life Policy #
Age Banded Rates per$1(k)
EmployeeMonthlyPremium
Age Banded Ratesper $1(k)
Spouse MonthlyPremium
Age Banded Rates per$1(k)
EmployeeMonthlyPremium
Age Banded Ratesper $1(k)
Spouse MonthlyPremium
Age Banded Rates per$1(k)
EmployeeMonthlyPremium
Age Banded Ratesper $1(k)
Spouse MonthlyPremium
$0.057 $0.00 $0.084 $0.00 $0.060 $0.00 $0.060 $0.00 $0.065 $0.00 $0.064 $0.00$0.068 $0.00 $0.101 $0.00 $0.060 $0.00 $0.060 $0.00 $0.071 $0.00 $0.070 $0.00$0.091 $0.00 $0.134 $0.00 $0.070 $0.00 $0.070 $0.00 $0.095 $0.00 $0.094 $0.00$0.102 $0.00 $0.151 $0.00 $0.090 $0.00 $0.090 $0.00 $0.142 $0.00 $0.142 $0.00$0.113 $0.00 $0.168 $0.00 $0.140 $0.00 $0.140 $0.00 $0.216 $0.00 $0.216 $0.00$0.170 $0.00 $0.252 $0.00 $0.230 $0.00 $0.230 $0.00 $0.336 $0.00 $0.336 $0.00$0.260 $0.00 $0.387 $0.00 $0.390 $0.00 $0.390 $0.00 $0.496 $0.00 $0.496 $0.00$0.487 $0.00 $0.723 $0.00 $0.600 $0.00 $0.600 $0.00 $0.709 $0.00 $0.710 $0.00$0.747 $0.00 $1.109 $0.00 $0.940 $0.00 $0.940 $0.00 $0.912 $0.00 $0.912 $0.00$1.437 $0.00 $2.134 $0.00 $1.690 $0.00 $1.690 $0.00 $1.297 $0.00 $1.298 $0.00$2.331 $0.00 $0.00 $3.020 $0.00 $3.020 $0.00 $2.454 $0.00 $2.454 $0.00
$0.00 $0.00 $0.00 $0.00 $0.00 $0.00
Included
All Full Time Employees Working 40 Hours
Birth to 14 days old: $0(k), 14 days to 6 months: $500,6 months to age 19 (23 IFS) months to 19 (26 IFS) increments of $2(k)
Lesser of current amount or $50(k)
0.028
$0.00
20% of Eligible
24 Months
$0
Employee Coverage Spouse Coverage
$0.250
75% of coverage to a maximum of $500(k)Included, prior to Age 65
IncludedIncluded
50% of employee coverage
65% at 70, 45% at 75, 30% at 80, 20% at 85, 15% at 90
All Full Time Employees Working 30 Hours
Increments of $5(k), to a max of 5x BAE or 100(k)
65% at 65, 40% at 70, 20% at 75
Increments of $5(k) up to a max of $10(k)
Greater of 50% or 10 lives
$50(k)$25(k)
Increments of $10(k), to a max of 5x BAE or $300(k)
$0.140$0.00
$10(k)
50% of coverage to a maximum of $100(k)
Included
$0
Employee Coverage Spouse Coverage
Included, prior to Age 65
24 Months
Not Included
Live birth to 14 days old: $1(k), 14 days to 6 months: $1(k),6 months to 19 (26 IFS) increments of $2(k) up to $10(k)
SunLife2 Mutual of Omaha2
Increments of $10(k), to a max of 5x BAE or $300(k)Increments of $5(k) to the lesser of 100% or up to a max of $50(k)
IncludedIncluded
Unum
All Full Time Employees Working 30 Hours
Increments of $10(k), to a max of 5x BAE or $500(k)
65% at 65, 50% at 70
Increments of $5(k) to the lesser of 100% or Employee amount or $500(k)
Employee Coverage
$50(k)$15(k)$10(k)
Spouse Coverage
100% of coverage to a maximum of $250(k)Included
Not Included
$0$0.500$0.00
Greater of 20% or 10 lives
36 Months
Universal Management Company | Voluntary Life Analysis
48

Proposed Plan
Renewal Date: 10 / 1 / 2016
Age BracketEmployee
Age BandedVolume
Spouse AgeBandedVolume
20-24 $0 $025-29 $0 $030-34 $0 $035-39 $0 $040-44 $0 $045-49 $0 $050-54 $0 $055-59 $0 $060-64 $0 $065-69 $0 $070-99 $0 $0TOTAL $0 $0
EE's EnrolledSP's Enrolled
Rates higher for anyone 70+Monthly Premium
VolumeRate per $1(k)
Employee Rate Change Occurs
Employee and Spouse Product Cost
Cost
Child(ren) Product Cost: Enrolled
Rate Guarantee | Duration:
Additional Plan Details:
True Open Enrollment
AD&D Plan Features:
Portability
Voluntary Life Employee Eligibility:Class Description
Employee AmountSpouse Amount
Child
Guarantee Issue Amounts:
Child Amount
Employee Reduction Schedule
Spouse Employee
Voluntary Life Benefit Amounts:
Minimum Participation
Conversion
Voluntary Life Plan Features:
Waiver of PremiumAccelerated (Living) Benefit
Voluntary Life Policy #
Age Banded Rates per$1(k)
EmployeeMonthlyPremium
Age Banded Ratesper $1(k)
Spouse MonthlyPremium
$0.044 $0.00 $0.044 $0.00$0.044 $0.00 $0.044 $0.00$0.056 $0.00 $0.056 $0.00$0.074 $0.00 $0.074 $0.00$0.100 $0.00 $0.100 $0.00$0.150 $0.00 $0.150 $0.00$0.230 $0.00 $0.230 $0.00$0.400 $0.00 $0.400 $0.00$0.533 $0.00 $0.533 $0.00$1.000 $0.00 $1.000 $0.00$1.607 $0.00 $1.607 $0.00
$0.00 $0.00
Child 15 days to 6 months old: $1,000, 6 months to 19 (23 IFS): Options of$1,000, $2,000, $4,000, $5,000, or $10,000
All Full Time Employees Working 30 Hours
Increments of $10(k), to a max of 5x BAE or $500(k)Increments of $5(k) to a max of $100(k) not to exceed 50% of EE amount
24 Months
None
$50(k)$25(k)
48% and at least 10 covered lives
$10(k)
80% of coverage to a maximum of $500(k)Included, prior to Age 60
IncludedIncluded
MetLife2
$0.00
Employee Coverage Spouse Coverage
$0$0.240
$0.017 Spouse / $0.051 / Child
Universal Management Company | Voluntary Life Analysis
49

1) Employee headcounts obtained from May 2016 census.2) Some carriers offer multi-product discounts, if you move a line of coverage it may increase cost to other lines if this discount is in place.3) The benefits shown in this section are not an insurance contract. The information provided is for illustrative purposes only.Please refer to the contract for the exact description and details.
Optional Life Plan Disclaimers
Benefit Improvements Benefit Reductions
Universal Management Company | Voluntary Life Analysis
50

SHORT TERM DISABILITY PLAN OPTIONS
SMART BENEFIT SOLUTIONS
51
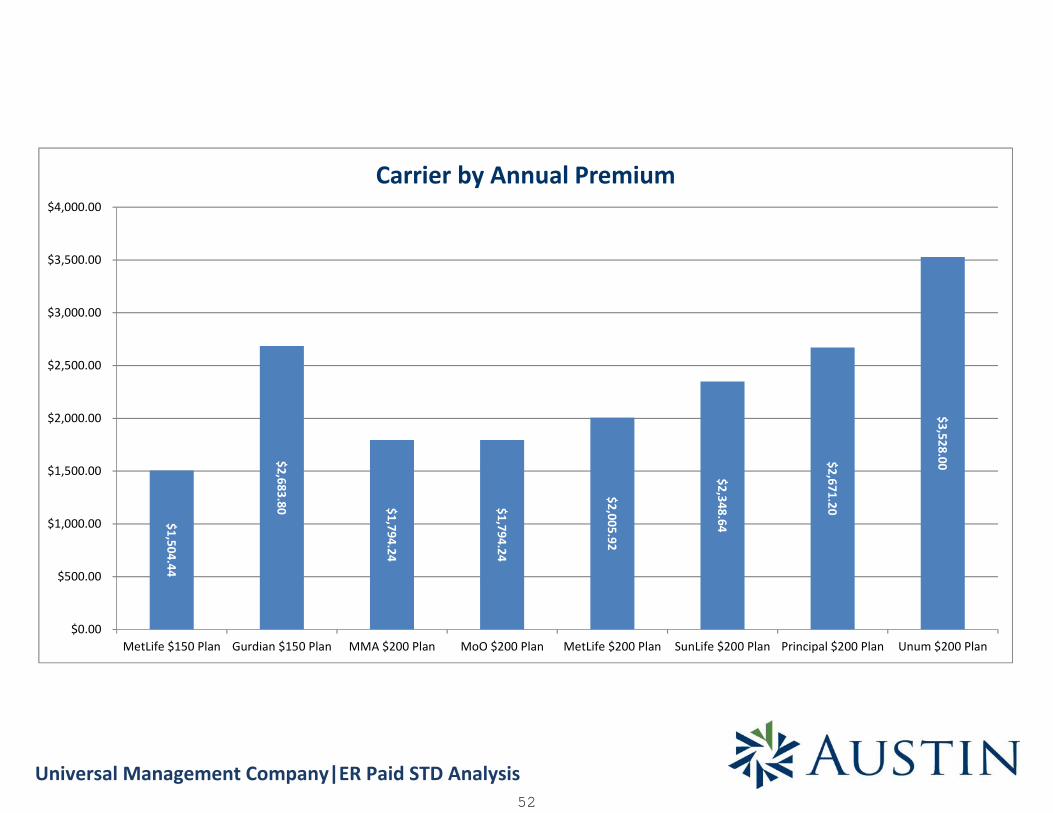
Universal Management Company|ER Paid STD Analysis
$1,504.44
$2,683.80 $1,794.24
$1,794.24
$2,005.92
$2,348.64
$2,671.20
$3,528.00
$0.00
$500.00
$1,000.00
$1,500.00
$2,000.00
$2,500.00
$3,000.00
$3,500.00
$4,000.00
MetLife $150 Plan Gurdian $150 Plan MMA $200 Plan MoO $200 Plan MetLife $200 Plan SunLife $200 Plan Principal $200 Plan Unum $200 Plan
Carrier by Annual Premium
52
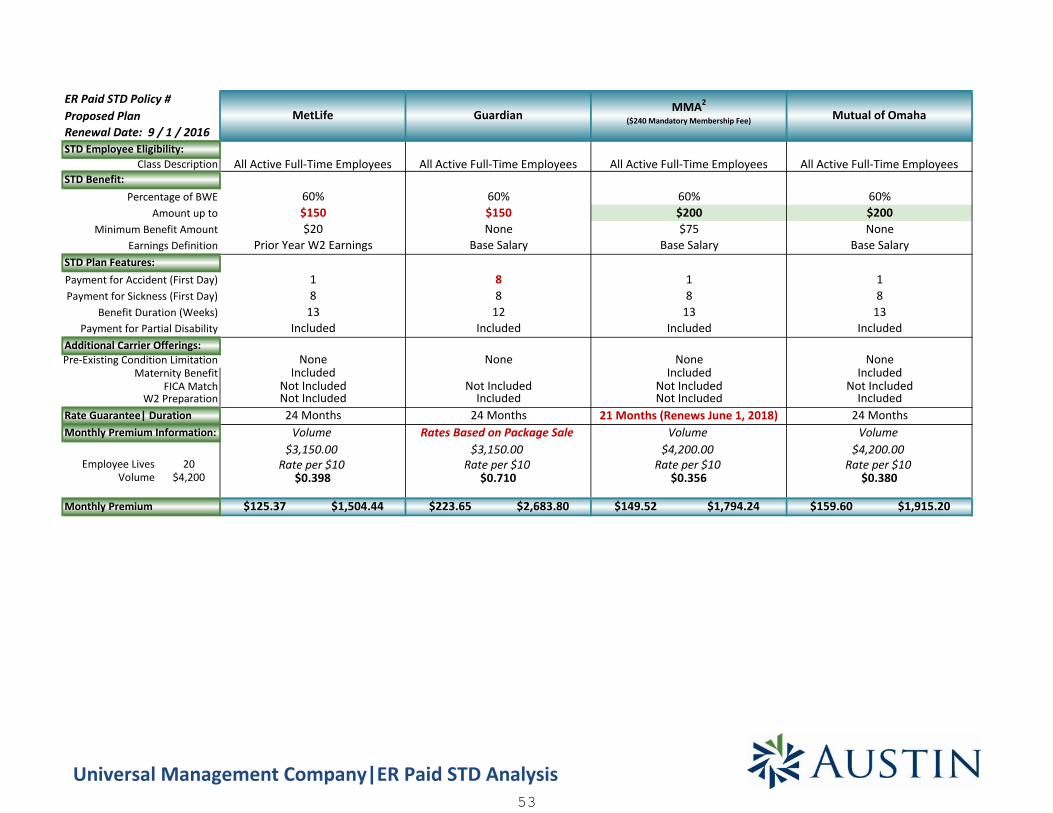
Employee Lives 20Volume $4,200
$125.37 $1,504.44 $223.65 $2,683.80 $149.52 $1,794.24 $159.60 $1,915.20
24 Months
$3,150.00 $3,150.00
NoneIncluded
Rate per $10$0.356
$4,200.00 $4,200.00
Not Included
18
$75Base Salary
MMA2
($240 Mandatory Membership Fee)
All Active Full-Time Employees
$200
Monthly Premium
W2 Preparation IncludedRate Guarantee| DurationMonthly Premium Information:
Not Included21 Months (Renews June 1, 2018)
Volume
Pre-Existing Condition Limitation NoneMaternity Benefit
FICA Match
Payment for Partial Disability IncludedAdditional Carrier Offerings:
Included
Payment for Sickness (First Day) 8Benefit Duration (Weeks) 1313
STD Plan Features:Payment for Accident (First Day) 11
Minimum Benefit Amount NoneEarnings Definition Base Salary
$20Prior Year W2 Earnings
Percentage of BWE 60%Amount up to $200
60%
Class Description All Active Full-Time EmployeesSTD Benefit:
ER Paid STD Policy #
STD Employee Eligibility:
Proposed PlanRenewal Date: 9 / 1 / 2016
Mutual of OmahaMetLife
All Active Full-Time Employees
60%$150
813
Included
NoneIncluded
Not IncludedNot Included
Volume
Rate per $10$0.398
None
Guardian
All Active Full-Time Employees
60%$150None
Base Salary
$0.710
Not Included
$0.380
VolumeRates Based on Package Sale
Rate per $10 Rate per $10
88
12Included
Included
Included24 Months
Not Included
24 Months
Universal Management Company|ER Paid STD Analysis53

Employee Lives 20Volume $4,200
Monthly Premium
W2 PreparationRate Guarantee| DurationMonthly Premium Information:
Pre-Existing Condition LimitationMaternity Benefit
FICA Match
Payment for Partial DisabilityAdditional Carrier Offerings:
Payment for Sickness (First Day)Benefit Duration (Weeks)
STD Plan Features:Payment for Accident (First Day)
Minimum Benefit AmountEarnings Definition
Percentage of BWEAmount up to
Class DescriptionSTD Benefit:
ER Paid STD Policy #
STD Employee Eligibility:
Proposed PlanRenewal Date: 9 / 1 / 2016
$167.16 $2,005.92 $195.72 $2,348.64 $222.60 $2,671.20 $294.00 $3,528.00
$4,200.00 $4,200.00
60%$200
24 MonthsVolume
Included
Rate per $10$4,200.00 $4,200.00
NoneIncluded
Not Included
13Included
13Included
18
$20Prior Year W2 Earnings
$200$200
Base SalaryNone
Base Salary
Included
$0.700
MetLife
All Active Full-Time Employees
Included
Volume
Rate per $10Rate per $10 Rate per $10
Included24 Months
Volume
Not Included
3/12
24 Months
Sun Life
All Active Full-Time Employees
None
1
Included
Unum
All Active Full-Time Employees
$0.530$0.466
60%
$25
$0.398
Volume
Included
Not Included
8
60%
Principal
All Active Full-Time Employees
60%
Treated as Any Other Disability
Included
None
IncludedIncluded
$200$15
Base Salary
18
13
88
12
24 Months
Universal Management Company|ER Paid STD Analysis54
1) Employee headcounts obtained from May 2016 census.2) Rates are contingent on a packaged sale.3) Some carriers offer multi-product discounts, if you move a line of coverage it may increase cost to other lines if this discount is in place.4) The benefits shown in this section are not an insurance contract. The information provided is for illustrative purposes only. Please refer to the contractfor the exact description and details.
STD Plan Disclaimers
Benefit Improvements Benefit Reductions
Universal Management Company |ER Paid STD Analysis55

LONG TERM DISABILITY PLAN OPTIONS
SMART BENEFIT SOLUTIONS
56
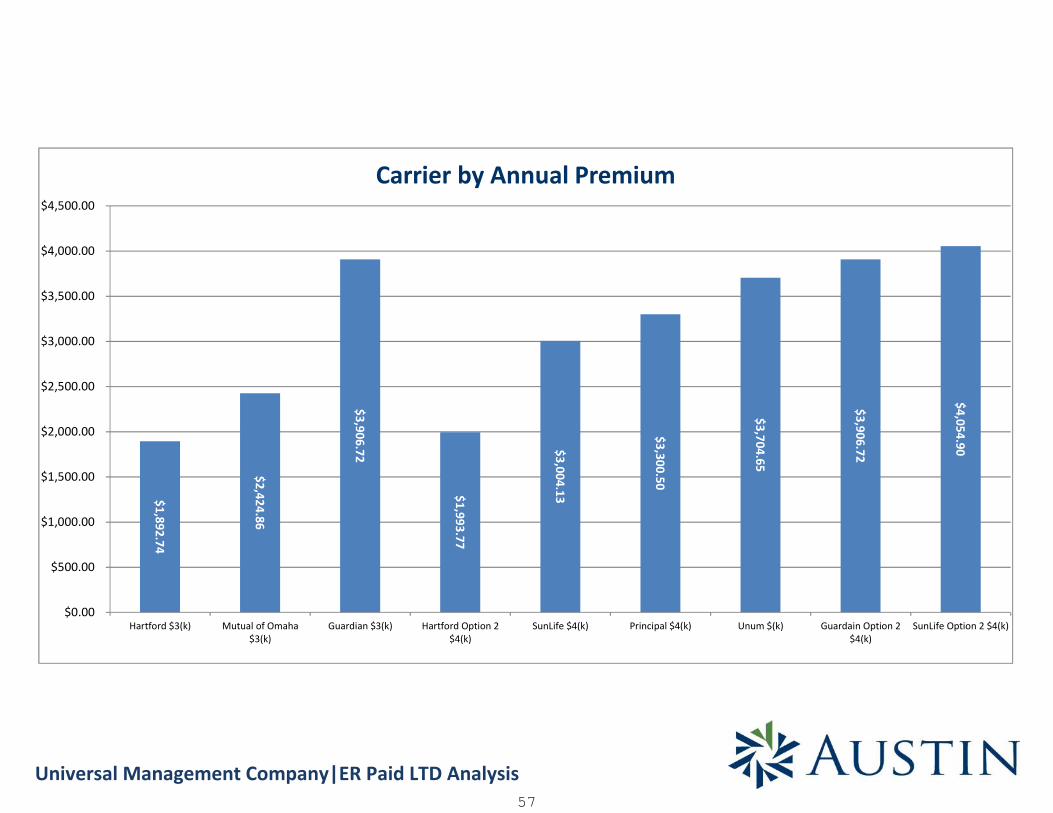
Universal Management Company|ER Paid LTD Analysis
$1,892.74
$2,424.86
$3,906.72
$1,993.77
$3,004.13
$3,300.50
$3,704.65
$3,906.72
$4,054.90
$0.00
$500.00
$1,000.00
$1,500.00
$2,000.00
$2,500.00
$3,000.00
$3,500.00
$4,000.00
$4,500.00
Hartford $3(k) Mutual of Omaha$3(k)
Guardian $3(k) Hartford Option 2$4(k)
SunLife $4(k) Principal $4(k) Unum $(k) Guardain Option 2$4(k)
SunLife Option 2 $4(k)
Carrier by Annual Premium
57

Proposed Plan
Class Description Class 1:
Contributory Status Class 1:
Definition of Dis. Class 1:
Earnings Test Class 1:
Employee Lives 20Volume $56,131
$157.73 $1,892.74 $202.07 $2,424.86 $325.56 $3,906.72
Rates Based on Package Sale
Direct / Family3x GMB
Rate per $1000.580%
24 Months LifetimeNone
24 Months
Not Included
6 / 24
110% for first 12 MonthsGreater of Direct Reduction or Proportionate Loss
Lesser of 10% or CPI
Yes, in Excess of 100%None
24 Months Lifetime
Not Included
$3(k)Base Salary
Tax Choice /100% Participation Required90
UnlimitedSSNRA
2 Year Own Occupation
80% / 80%
Guardian
All Full Time Active Employees Working 30
60%$3(k)
Not Included
None
None
Rate per $100
3x GMB
Rate per $100
None3 / 12
$3(k)
Full Family
180RBD to SSNRA
2 Year Own Occupation
99% / 85%
Guarantee Issue Amount $3(k) $3(k)
ER Paid LTD Policy #
LTD Employee Eligibility:
All Full Time Active Employees Working 30 All Full Time Active Employees Working 30
Percentage of BME
Tax Choice /100% Participation RequiredLTD Plan Features:
Earnings Definition Base Salary Base Salary
60% 60%$3(k)Amount up to
Tax Choice /100% Participation Required
Benefit Period90
LTD Benefit:
Elm. Period (# of Days) 180Accum. Period (# of Days)
90
2 Year Own Occupation
Not Included
24 Months Lifetime
Revenue Protection Benefit
ADEA 1 with SSNRA
Residuals after First 12 Mos.
Integration
Mutually Progressive Partial
Infectious / Contagious Rider Not Included
Rate Guarantee| Duration 24 Months 24 Months
Monthly Premium Info:
Monthly Premium0.28% 0.36%
Not Included
24 Months Lifetime
Direct / FamilySurvivor Benefit
Pre-Existing Condition Limit
Additional Carrier Offerings:
6 / 12
Dollar for Dollar
Drug / Alcohol Limit
Offsets for Individual DisabilityMental / Nervous Limit
NoneOffsets for Salary Cont.
Proportionate LossIndexing Lesser of 10% or CPI
24 Months Lifetime
80% / 80%Return to Work Benefit
Renewal Date: 9 / 1 / 2016
Headcounts | Rates:
Hartford Mutual of Omaha
3x GMB
Yes, in Excess of 100%
100% for first 12 Months
LTD Plan Offsets & Limitations:
NoneSelf-Reported Symptoms Limit
100% to End of Max Benefit Period
24 Months Lifetime
Universal Management Company | LTD Analysis58
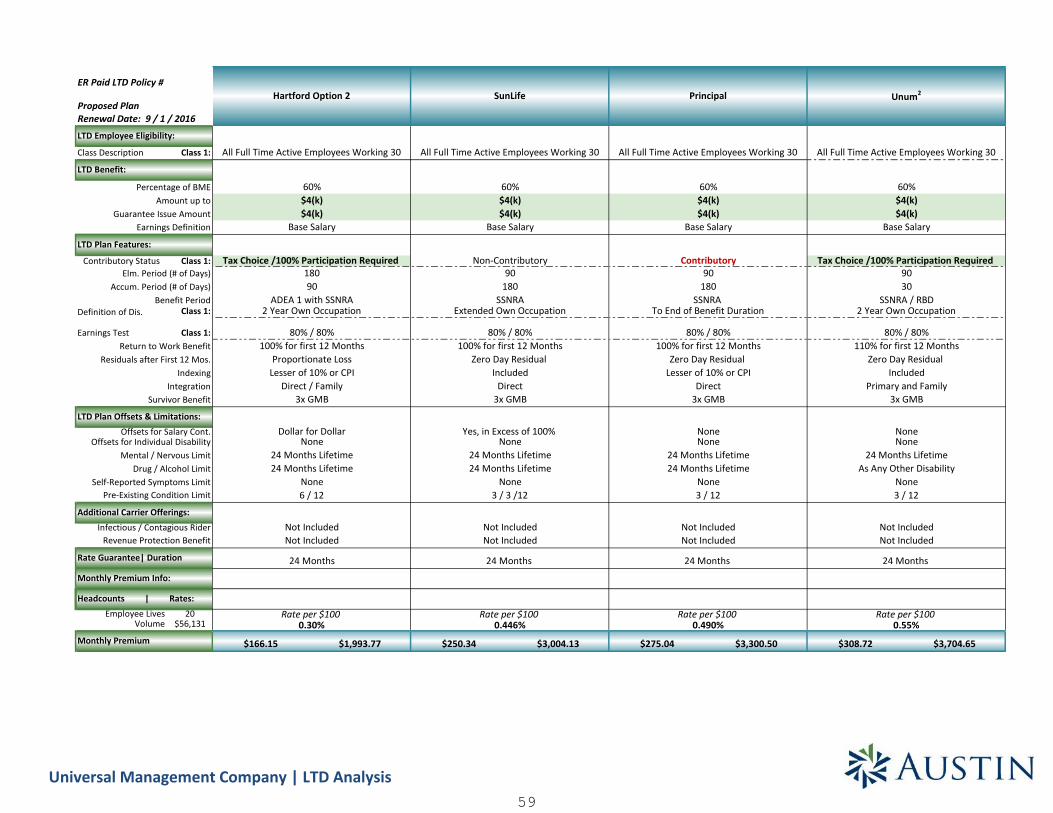
Proposed Plan
Class Description Class 1:
Contributory Status Class 1:
Definition of Dis. Class 1:
Earnings Test Class 1:
Employee Lives 20Volume $56,131
Guarantee Issue Amount
ER Paid LTD Policy #
LTD Employee Eligibility:
Percentage of BME
LTD Plan Features:
Earnings Definition
Amount up to
Benefit Period
LTD Benefit:
Elm. Period (# of Days)Accum. Period (# of Days)
Revenue Protection Benefit
Residuals after First 12 Mos.
Integration
Infectious / Contagious Rider
Rate Guarantee| Duration
Monthly Premium Info:
Monthly Premium
Survivor Benefit
Pre-Existing Condition Limit
Additional Carrier Offerings:
Drug / Alcohol Limit
Offsets for Individual DisabilityMental / Nervous Limit
Offsets for Salary Cont.
Indexing
Return to Work Benefit
Renewal Date: 9 / 1 / 2016
Headcounts | Rates:
LTD Plan Offsets & Limitations:
Self-Reported Symptoms Limit
$166.15 $1,993.77 $250.34 $3,004.13 $275.04 $3,300.50 $308.72 $3,704.65
24 Months
Rate per $1000.30%
24 Months LifetimeNone6 / 12
Not IncludedNot Included
Direct / Family3x GMB
Dollar for DollarNone
24 Months Lifetime
ADEA 1 with SSNRA2 Year Own Occupation
80% / 80%100% for first 12 Months
Proportionate LossLesser of 10% or CPI
$4(k)Base Salary
Tax Choice /100% Participation Required18090
Hartford Option 2
All Full Time Active Employees Working 30
60%$4(k)
3 / 3 /12
Not Included
SunLife
60%$4(k)$4(k)
Rate per $1000.446%
All Full Time Active Employees Working 30
Not Included
24 Months
IncludedDirect
3x GMB
Base Salary
24 Months Lifetime
Non-Contributory90
180SSNRA
Extended Own Occupation
80% / 80%
Yes, in Excess of 100%
100% for first 12 Months
None
24 Months LifetimeNone
Zero Day Residual
Not IncludedNot Included
24 Months
Rate per $100
24 Months LifetimeAs Any Other Disability
None3 / 12
0.55%
IncludedPrimary and Family
3x GMB
NoneNone
SSNRA / RBD2 Year Own Occupation
80% / 80%110% for first 12 Months
Zero Day Residual
$4(k)Base Salary
Tax Choice /100% Participation Required9030
Unum2
60%$4(k)
All Full Time Active Employees Working 30
Principal
All Full Time Active Employees Working 30
60%
180SSNRA
To End of Benefit Duration
80% / 80%
$4(k)$4(k)
Base Salary
Contributory90
None3 / 12
100% for first 12 MonthsZero Day Residual
Lesser of 10% or CPIDirect
3x GMB
Not IncludedNot Included
24 Months
Rate per $1000.490%
NoneNone
24 Months Lifetime24 Months Lifetime
Universal Management Company | LTD Analysis59

Proposed Plan
Class Description Class 1:
Contributory Status Class 1:
Definition of Dis. Class 1:
Earnings Test Class 1:
Employee Lives 20Volume $56,131
Guarantee Issue Amount
ER Paid LTD Policy #
LTD Employee Eligibility:
Percentage of BME
LTD Plan Features:
Earnings Definition
Amount up to
Benefit Period
LTD Benefit:
Elm. Period (# of Days)Accum. Period (# of Days)
Revenue Protection Benefit
Residuals after First 12 Mos.
Integration
Infectious / Contagious Rider
Rate Guarantee| Duration
Monthly Premium Info:
Monthly Premium
Survivor Benefit
Pre-Existing Condition Limit
Additional Carrier Offerings:
Drug / Alcohol Limit
Offsets for Individual DisabilityMental / Nervous Limit
Offsets for Salary Cont.
Indexing
Return to Work Benefit
Renewal Date: 9 / 1 / 2016
Headcounts | Rates:
LTD Plan Offsets & Limitations:
Self-Reported Symptoms Limit
$325.56 $3,906.72 $337.91 $4,054.90
0.580%
Not IncludedNot Included
24 Months
Rates Based on Package SaleRate per $100
Yes, in Excess of 100%None
24 Months Lifetime24 Months Lifetime
None6 / 24
110% for first 12 MonthsGreater of Direct Reduction or Proportionate Loss
Lesser of 10% or CPIDirect / Family
3x GMB
Tax Choice /100% Participation Required90
UnlimitedSSNRA
2 Year Own Occupation
80% / 80%
Guardian Option 2
All Full Time Active Employees Working 30
60%$4(k)$4(k)
Base Salary
SunLife Option 2
All Full Time Active Employees Working 30
60%$4(k)$4(k)
Base Salary
Tax Choice /100% Participation Required90
180SSNRA
Extended Own Occupation
80% / 80%100% for first 12 Months
Zero Day ResidualIncluded
Direct3x GMB
Yes, in Excess of 100%None
24 Months Lifetime24 Months Lifetime
None3 / 3 /12
Not IncludedNot Included
24 Months
Rate per $1000.602%
Universal Management Company | LTD Analysis60

1) Employee headcounts obtained from May 2016 census.2) Rates are contingent on a packaged sale.3) Some carriers offer multi-product discounts, if you move a line of coverage it may increase cost to other lines if this discount is in place.4) The benefits shown in this section are not an insurance contract. The information provided is for illustrative purposes only. Please refer to the contractfor the exact description and details.
LTD Plan Disclaimers
Benefit Improvements Benefit Reductions
Universal Management Company| LTD Analysis61

SPECIALTY BENEFITS
SMART BENEFIT SOLUTIONS
62

Service
CancerInvasive Cancer
Carcinoma in SituBenign Brain Tumor
Skin Cancer
VascularHeart Attack
StrokeHeart Failure
Arteriosclerosis
OtherOrgan FailureKidney Failure
Group 2 Covered Conditions
Group 3 Childhood Covered Conditions
Cancer VaccinePre-Existing Conditions
Wellness Benefit
Dependent Age Limits
Benefit Reduction Schedule
Contribution / Participation
EE Critical Illness Benefit Amounts
Dependent Critical Illness Benefit Amount
Underwriting Requirements
2-24 Eligible Lives25 - 99 Eligible Lives Guarantee Issue
25 - 99 Lives Conditional Issue
Benefit Amounts Under 30 Ages 40 - 49 Ages 50 - 59 Ages 60 - 69$5,000 $7.38 $15.07 $25.42 $37.78
$10,000 $13.08 $28.22 $48.57 $72.88$15,000 $18.78 $41.37 $71.72 $107.98$20,000 $24.48 $54.52 $94.87 $143.08$25,000 $30.18 $67.67 $118.02 $178.18
Benefit Amounts Under 30 Ages 40 - 49 Ages 50 - 59 Ages 60 - 69$2,500 $4.53 $8.50 $13.85 $20.23$5,000 $7.38 $15.07 $25.42 $37.78$7,500 $10.23 $21.65 $37.00 $55.33
$10,000 $13.08 $28.22 $48.57 $72.88$12,500 $15.93 $34.80 $60.15 $90.43
1) The Critical Illness plan is Voluntary.
2) Premiums Listed are for Issue Age and will not increase due to Insured's Age. Child Cost is Included with Employee Elections
3) Spouse Rate is Based on employee's age bracket
4) 2 Year Rate Guarantee
5) Not Available for All Industries
2016 Critical Illness
$31.74$39.24
$70.92$138.52$206.12
Employee May Choose a lump sum benefit of $5(k) to $25(k) In increments of $5(k)
Ages 70 +Ages 30 - 39
Spouse: Up to 50% of EE Benefit Child: 25% of EE Benefit
$16.74$24.24
$250 per Lifetime
Employee < 70 Spouse < 70 Child
Health Questions Required on All Amounts
All Amounts Guaranteed
100%30%
50%
First Occurrence of these additional illnesses: Addison's Disease 30%, ALS (Lou Gehrig's Disease) 100%, Alzheimer's Disease 50%, Coma 100%, Huntington'sDisease 30%, Multiple Sclerosis 30%, Loss of Speech, Sight or Hearing 100%, Parkinson's Disease 100%, Permanent Paralysis 50% for 1 limb, 100% for 2 Limbs,
Severe Burns 100%100% of Child Benefit for the First Occurrence of Cerebral Palsy, Cleft Lip/palate, Club Foot, Cystic Fibrosis, Down's Syndrome, Muscular Dystrophy, Spina Bifida,
Type 1 Diabetes
Groups 2 - 99 Employees
First Occurrence Second Occurrence
Covered Conditions(Lump Sum Payments)
100%30%75%
50%100%100%
50%0%0%
Not Included
50%
Plan # 1
0%50%50%
100%100%
$50 per lifetime for receiving Cancer Vaccine3 Months Look Back Period, 12 Month Exclusion Period
Provides a per year benefit for completing certain routine wellness screenings or procedures (refer to plan highlights for listing)Employee $50; Spouse $50; Child $50
Child Birth to 26 years
50% at 70(If Actively at Work)
Ages 30 - 39 Ages 70 +
Voluntary - 2 - 9 Eligible Employees Must Have a Minimum of 2 Enrolled, 10 - 24 Eligible Employees Must Have a Minimum of 5 Enrolled, 25+ Eligible Employees Must Have Greater of10 Enrolled or 15%
Employee & Spouse Ages 70 +
Health Questions Required
$5.49 $37.12
Employee
Spouse
$273.72
$2,500 GI
Health Questions Required on All Amounts Above Guarantee Issue
$5(k) GI
$341.32
$9.24
$20.49 $172.32
$9.24 $70.92$12.99 $104.72$16.74 $138.52
This outline is intended only as a source of reference. Official benefits, conditions, limitations and exclusions are documented in plan contracts .63

GuardianValue Plan
GuardianAdvantage Plan
GuardianPremier Plan
$150(Accident Emergency Treatment)
$175(Accident Emergency Treatment)
$200(Accident Emergency Treatment)
$25 up to 6 Treatments(Doctor Visit)
$50 up to 6 Treatments(Doctor Visit)
$75 up to 6 Treatments(Doctor Visit)
Ground: $100Air: $500
Ground: $150Air: $1(k)
Ground: $200Air: $1,500
Hospital Admission: $750Hospital Confinement: $175 / Day, up to 1 Year
ICU Admission: $1,500ICU Confinement: $350 / Day, up to 15 Days
Hospital Admission: $1(k)Hospital Confinement: $225 / Day, up to 1 Year
ICU Admission: $2(k)ICU Confinement: $450 / Day, up to 15 Days
Hospital Admission: $1,250Hospital Confinement: $250 / Day, up to 1 Year
ICU Admission: $2,500ICU Confinement: $500 / Day, up to 15 Days
Employee: $10(k)Spouse / Child: $5(k)
(As a Result of Accidental Death) ;
Percentage of Benefit is Paid for Dismemberment orLoss of Sight, Speech, Hearing, & Cognitive Function
due to Accidental Injury
Employee: $25(k)Spouse: $12,500
Child: $5(k)(As a Result of Accidental Death) ;
Percentage of Benefit is Paid for Dismemberment orLoss of Sight, Speech, Hearing, & Cognitive Function
due to Accidental Injury
Employee: $50(k)Spouse: $25(k)
Child: $5(k)(As a Result of Accidental Death) ;
Percentage of Benefit is Paid for Dismemberment orLoss of Sight, Speech, Hearing, & Cognitive Function
due to Accidental Injury
$50 $75 $100
$1,500/$750/$750 $2,500/$1,250/$1,250 $3,500/$1,750/$1,750
$150 $250 $350
$25 / Day for up to 10 Days $25 / Day for up to 10 Days $35 / Day for up to 10 Days
$150 / Day for up to 15 Days $150 / Day for up to 15 Days $150 / Day for up to 15 Days
$100 $125 $125
1: $5002 or More: $1(k)
1: $5002 or More: $1(k)
1: $7502 or More: $1,500
$300 $300 $300
$400(3 Times per Accident)
$500(3 Times per Accident)
$600(3 Times per Accident)
$100 / Day for up to 30 Days $125 / Day for up to 30 Days $150 / Day for up to 30 Days
$13.35 $17.28 $21.30$22.86 $29.24 $35.72$23.30 $29.42 $35.39$32.81 $41.38 $49.81
1) Accident Coverage is Off-the-Job.2) Accident Coverage is Voluntary.
4) 2 Year Rate Guarantee5) Portability Included without EOI
3) Guardian's Accident Coverage also includes benefits for Catastrophic Loss, Common Carrier, Common Disaster, Seatbelt / Airbag Use, Reasonable Accommodation to Home / Vehicle, Burns, ChildOrganized Sports, Chiropractic Visits, Coma, Concussions, Dislocations, Major Diagnostic Exams, Emergency Dental Work, Epidurals, Eye Injury, Family Care, Fractures, Initial Office / UC Treatment, KneeCartilage, Hip/Knee/Shoulder Joint Replacement, Laceration, Surgical Repair for Ruptured Disc, Cranial/Open Abdominal/Thoracic/Exploratory/Arthroscopic Surgery, Tendon/Ligament/Rotator Cuff, and X-Rays
EmployeeEE & Spouse
EE & Child(ren)Family
Surgery - Exploratory or Arthroscopic
Monthly Premium
Prosthesis Benefit
Occupational / Physical Therapy Benefit
Minimum Participation 2 - 9 Eligible Lives Minimum 2 Enrolled / 10 - 999 Eligible Lives Minimum 5 Enrolled Employees
Provides a $50 per year benefit for completing certain routine wellness screenings or procedures (refer to plan highlights for listing)
Hospital / ICU
AD&D Death Benefit
Initial Physicians Office / Urgent Care FacilityTreatment
Blood / Plasma / Platelets Benefit
Transportation Benefit
Wellness benefit
Appliances Benefit
Universal Management Company2016 Accident Coverage Comparison
Rehabilitation Unit Confinement Benefit
Joint Replacement(Hip/Knee/Shoulder)
Family Lodging Benefit
Service
Accident Medical Expense
Accident Follow Up Treatment
Ambulance Benefit
This outline is intended only as a source of reference. Official benefits, conditions, limitations and exclusions are documented in plan contracts.64

DISCLOSUREThe material contained herein includes a descriptive summary of current and / orproposed benefit plans and estimated associated costs. The benefit plandescription should not be construed as a substitution for the insurance policy butas a synopsis thereof. Costs are based upon available census data and may vary atplan implementation in accordance with the actual enrollment.
IMPORTANT NOTICE:All employees must be “ACTIVELY-AT-WORK” and dependents not disabled onthe effective date to be eligible for coverage.
The Austin Benefits Group may not bind coverage. Existing coverage should notbe canceled until written confirmation of coverage from the new insurancecompany is received. Written confirmation will generally be received in two tothree weeks following the application to the insurance company.
AUSTIN BENEFITS GROUP
65

38500 Woodward Ave., Suite 360, Bloomfield Hills, MI 48304 Phone: 248.594.5550 Fax: 248.594.5533 www.austinbenefits.com
66