alternate care site acs - minnesota department of health · how an alternate care site fits into...
TRANSCRIPT

Alternate Care Site
ACS
Role of Medical Reserve Corps
Objectives What is an Alternate Care Site is
Why an Alternate Care Site may be necessary
Plans in the metro areas that have been developed to open an Alternate Care Site
Possible role of Medical Reserve Corps Volunteers at an Alternate Care Site
How an Alternate Care Site fits into the “big picture” response to a health emergency
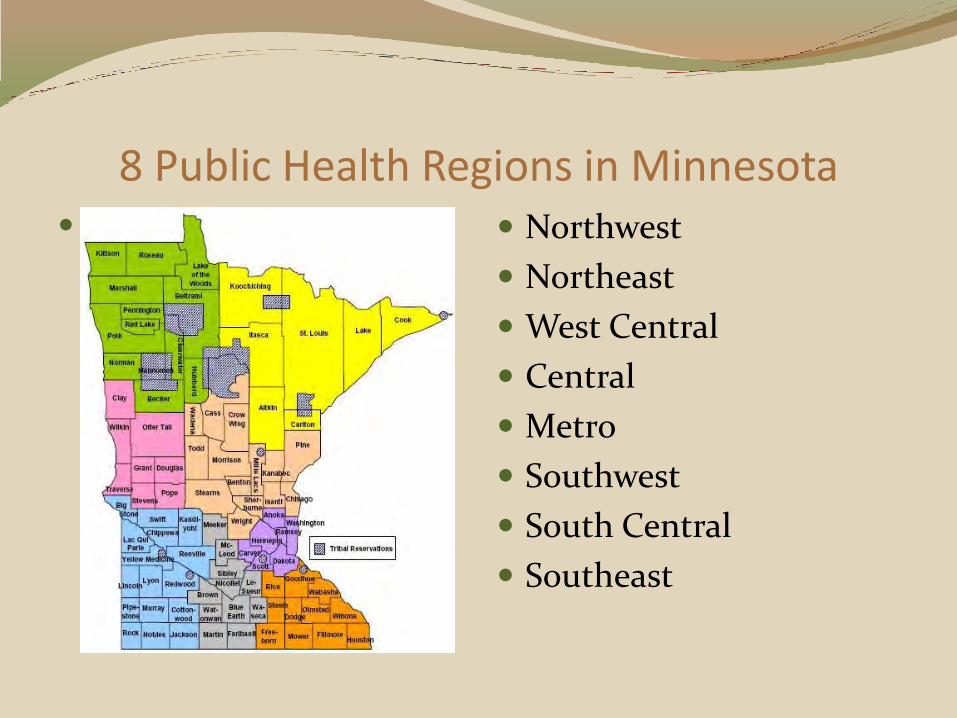
8 Public Health Regions in Minnesota
Northwest
Northeast
West Central
Central
Metro
Southwest
South Central
Southeast

Metropolitan Hospital Compact 29 Hospitals
7 County Metro Area
Agreements
Multidisciplinary Group
Hospitals
EMS
Public Health (state and local)
Every Public Health Region in State has a compact

Hospital Compact Work Groups Alternate Care Site (ACS)
Clinic Coordination
Long Term Care (LTC)
Behavioral Health (BH)
Laboratory
Emergency Medical Systems (EMS)
Regional Hospital Resource Center (RHRC)
Exercise
Steering Committees
Metro Pharmaceutical Cache
MNTrac

Alternate Care Site Work Group
One of the first work groups formed
Led by Pat Hadfield - HCMC
Hospital regulatory compliance – Joint Commission
All hospitals working together

Kittson Roseau
Lake
of the
WoodsMarshall
Polk
Pennington
Red Lake
Clearw
ater
Norman Hu
bb
ard
Becker
Koochiching
Itasca St. Louis Lake
Cook
Aitkin
Carlton
Cass
Wad
ena
Todd
Morrison
Mille L
acs
Kanabec
Pine
Stearns
Benton
Isanti Chisago
Wright
Clay
Otter TailWilkin
Grant Douglas
Traverse
Stevens Sher-
burne
Pope
Anoka
Hennepin
Washington
Carver
Dakota
Meeker
Mc-
Leod
Le-
SueurNicollet
Brown
Blue
Earth
Wa-
secaWat-
onwan
Faribault
GoodhueRice
Wabasha
SteeleOlmsted
Winona
Free-
bornMower Fillmore
Houston
Big
StoneSwift Kandi-
yohiChippewa
Lac Qui
ParleRenville
LincolnLyon
Redwood
Pipe-
stoneMurray Cotton-
wood
Rock Nobles Jackson
Sibley
Crow
Wing
Ramsey
Martin
Beltrami
Mahnomen
Yellow MedicineScott
Dodge
Tribal Reservations
Indicates Current ACS Sites

Mission of the ACS
To establish patient care facilities during an emergency/disaster if hospitals are taxed beyond capacity. This may be required for triage, screening, initial treatment or for an austere patient care site
Provide effective care to the greatest number of people with limited resources

Hospital Surge Capacity How many extra patients can a hospital take beyond their
normal capacity
MCI – public health event
Hospital plans satisfy grant deliverables & Joint Commission – surge to X% beyond normal capacity – strategies include
Cancelling elective surgeries
Make single rooms into doubles
Convert classrooms to wards with cots
Altered standards of care
Early discharges
Staff shift changes – 12 hour shifts

Role of RHRC/Metropolitan Hospital Compact in Surge Capacity Planning
As hospitals meet their individual surge capacity the RHRC and Metropolitan Hospital Compact can monitor and facilitate moving patients to other hospitals
MNTrac
As the metro hospitals all reach their surge capacities an Alternate Care Facility may be opened
Not for short term or limited time event
Not for events that affect one or two hospitals
Considered when resources are stretched to the max
Requires 72 hours to open
Activation of Alternate Care Site Hospitals
contact RHRC leadership
RHRC activated
MDH notified by RHRC
RHRC representative
to SEOC
ACS work group
activated

Decision to Open Alternate Care Site RHRC with input from other facilities will assess the
community
Local and jurisdictional Emergency Managers, in collaboration with the Local Public Health and the State Health Department will approve the activation of an ACS and assist with the resource requests.
Request for the use of a facility (ACS) is made via the local and/or jurisdictional Emergency Management agency or Multi-jurisdictional Incident Command
MDH designates Hennepin County Medical Center (RHRC) to assign an ACS Incident Commander that will oversee site operations.

Activation of Staff Who to activate – facilities in what order
Large hospitals paired with smaller hospitals - quadrants of metro area
Schedule of hospitals pre planned
How staff will be identified
Length of shifts (7a-7p & 7p-7a)
Transport & Parking - Metro Transit
Coordination of ACS Pre-established M.O.U.’s with many vendors
Metro Transit
Laundry
Food and supply vendors
West Metro (Mpls.)– HCMC
Minneapolis Convention Center (MCC)
Target Center
East Metro (STP)– Regions Hospital
River Center
Working with other agencies (local, county, cities, state, PHD, federal) as needed

Care at Alternate Care Site Austere care
Altered Standards of Care – hospitals and ACS
Greatest good for the greatest number
Services Basic laboratory samples
Basic medications
Basic x-ray service
? Oxygen
Behavioral Health
Protocols and Standing Orders

ACS set up at Minneapolis Convention Center
•All plans made for “pods” of 50 patients

Staffing
ACS staffing for each 50 patient pod
1 physician
1 PA/NP or 2nd physician
5 nurses and/or LPN’s, paramedics (at least 3 RN’s)
5 nursing assistants/EMT-B personnel
1 social worker/case manager
1 environmental service staff

Additional Staff Additional Support Personnel
1 charge RN/250 pts
1-2 unit secretaries/100 pts
1 respiratory therapist/ 100 pts
1 patient admissions clerk/100 pts
1 chaplain/100 pts
1 pharmacist (if hospital > 200 beds)
1 – 2 lab personnel
Food service workers
Security

Patients/Staffing Patient care will consist of basic, austere care
Patient assignments will be greater than usual for all staff
Roles will be less distinctly delineated than during normal hospital functioning; all providers will be expected to fill any patient care need that they are licensed and credentialed to fill
Due to the limitations of the facility and number of care-givers, patient care needs may be prioritized

Admission to Alternate Care Site

Care Delivery Patients will receive ID band – admissions clerk
Basic paper admission sheet completed
Patient Care
Focused H&P within 4 hours of admission with medical plan of care
Standing orders – VS, I&O, nursing assessment - every 12 hours
Documentation on nursing flow sheet
Medical staff will assess patients as warranted
A patient log of admission time/date, location, disposition, and discharge time/date will be kept current by the admissions clerk/unit secretaries.
All providers will document significant events, changes in patient condition, and changes in plan of care on multidisciplinary progress notes.
Charting will be by exception

Admission Criteria Patients who have been decontaminated (as needed), triaged
and screened for admission by an existing healthcare facility, clinic, or ACS personnel and are
Patients requiring peripheral IV therapy for drug administration, rehydration, and/or palliative care – no IV pumps will be available
Patients requiring oxygen therapy delivered by nasal cannula, mask, or trach collar only (assuming O2 delivery is able to be set up)
Patients with communicable diseases who are able to cohort
The Metro Region RHRC is working with the state on a pediatric emergency plan that would be incorporated into the ACS

Ineligible Criteria Patients requiring mechanical ventilation, continuous ECG
monitoring, vasopressors, ACLS, ATLS, PALS, or NALS
Patients in active labor
Patients with existing diseases (cardiovascular disease, diabetes, cancer, etc) who are experiencing exacerbations of these diseases concomitant with injury or infection.
Patients requiring frequent and/or complex diagnostic testing (eg. Radiology, Lab Services, etc.)
Patients requiring blood transfusions
Patients requiring hemodialysis

Incident Command The ACS will operate
according the National Incident Management System/HICS
Command Staff
Incident Commander
PIO
Safety Officer
Liaison Officer
General Staff
Finance/ Administration
Logistics
Operations
Planning

Security Resources available to staff at site
Number of staff required
Entrances &/or sites to post
Vendor deliveries
All staff clearance process
at check-in
ID Badges
Vests
Armbands

Communications Primary and back up methods
Phones – lines and cell
Radios – 800 mHz and familiy – HAM radios
Speakers – Bullhorn
Computers
Will equipment work (site checks)?
Interpreter Services
Language Line

Equipment
Lab, X-ray, Pharmacy, Materials Management – protocols, forms, etc.
Plan for delivery, set up & maintenance
Long shelf life &/or rotation of items
Basic response list per 50 beds/cots Cot
IV pole as needed – no pumps
Clipboard for record
Lamp
Plastic tub for patient belongings

Supplies Some in storage with long
shelf life
Minneapolis Convention Center
River Centre
Allina Warehouse
Ask hospitals to contribute
Just in time ordering through MOUs with vendors
Pharmaceuticals Develop list of appropriate meds
Do any meds need refrigeration?
Distribution / method of delivery
Security issues
Patient Education / Teaching Sheets
Discharge needs

Lab Coordination of qualified staff will be done by the RHRC
with the Regional Laboratory Leads in the Metro area. Staff will complete lab testing
I-STAT and document results. A minimum number of tests will be able to be performed according to equipment available
A courier system with a nearby facility will need to be developed to assist additional tests if needed

Food Services
Patients and staff
Contract with vendors on site
MCC system
River Centre
Disposable plates, cups & utensils, etc.

Behavioral Health Center (BHC)
Multidisciplinary - Chaplains, Social Workers, Counselors, Therapists
Psychological First Aid (PFA)
Patients
Families
Staff
Bedside consults
Interpreters/Language Line
Support from the Community

Support Center
Family & friends, yet maintain security
Patients under 14yo (minors) regarding care
On-site or at a nearby church?
Staffing & support
Temporary Morgue Resources within the
community
Procurement of refrigerated trucks
How to process the bodies (ID tags, bags)
Whom to notify for tracking purposes…..
Disaster Mortuary Team (DMORT)

Sanitation Environmental Services (Clean/Dirty)
Receiving items, containers
Vendor for disposal of dirty or contaminated materials
Laundry
Sharps
Medical waste
Training needed
Confidentiality
Infection control – handling of medical waste

Volunteers Medical Reserve Corps (MRC) – Licensed Personnel
Community Emergency Response Team (CERT)
non medical tasks – set up, security
Disaster Medical Assistance Team (DMAT)
Pre credentialed
Clearing site in community separate from facility
Liability Coverage

You are activated!
•Process
•Notification
•Reporting
•Assignment

Activation of Volunteer Staff at ACS
Need for staff is identified by Operations Chief at ACS
Logistics Chief at ACS will send request to the SEOC or the Minnesota Duty Officer who will contact the MN Responds MRC Coordinator
The local MRC Coordinator will be notified and will send a “call out” for volunteers
When you respond to the call, you will be directed where to report and other specific instructions as needed

Arrival at Alternate Care Site Bring your photo ID badge
with credentials
Sign in at registration table you will be given further instructions and an arm band for ID
Report to assigned area for Orientation and Just In Time Training (JITT)

Training Pre-event
This training
U of M online training @ http://cpheo.sph.umn.edu/
Psychological First Aid
Incident Command Training
All MRC training
JITT
Agent/Event specific information
Orientation to Alternate Care Site
Job specific information
Job Action Sheets

Topic Time Specifics
Welcome and Introductions
Determined by HICS – flush out for more specifics
5 mns Thank you for coming – pre-credentialed, skill set, & expectations,
Introduce ICS staff – explain vests point to command center
of ACS – (decrease pressure on hospitals)
Brief overview as large group and more specific small group
What is Alternate Care Site
Put together folders for MERET education (? Not too specific in details)
5 mns Provide austere care for patients
Hospitals full beyond capacity – exceeding surge capacity
Types of patients we will see
Basic services provided
o Basic cares
o Simple IV fluids
o Limited meds
o Limited lab
o O2?
o Psychological Care
Staff
- Remind hospitals that concept exists & script basic statement & process for their Emergency Response plan.
- Remind to utilize the on-line MERET education
- Expectations that core staffing is w/ hospitals and assistance w/ MRC & other volunteers
10 mns Shift times – specific assignments by direct supervisor
Check in – Hospital or Organizational Photo ID required
o ID badges given at check in returned at check out
o Reimbursement to “home” facility
o Shift times
o Communication (phone, radio, fax)
o Message Board – family contact
o Parking /transportation
o Legal – liability coverage, change in level of care/standards; Pre-education repeated annually at Compact
meeting
o Establish expectations with all compact hospitals.
o 1st option is for hospital staff to volunteer before assigning. The contract has no binding language if hospital
can’t or won’t participate.
o Get as much orientation done ahead of time w/ the concept & key elements as possible.
Virtual Tour (map on slide or drawing)/Floor Plan 10 mns Orient to map and point out each departmental area
o Main patient area (where they enter and are)
o Break room (valuables)
o Bathrooms
o Materials Management - supplies
o Lab
o Pharmacy
o Behavioral Health
o Medical Records
o Morgue
o Security posts/Safety
Infection Control 5 mns Basics (depending on event) details per specific role
o Hand washing – hand sanitizer
o PPE (gloves, masks, gowns, etc)
Behavioral Health 10 mns ? Show PFA video
Brief description of services available (patients, families, staff)
Alternate Care Site – Orientation/Operational Briefing General: (All staff at ACS) TOTAL OF 60 MINUTES

Questions?

Sheri Fox RN
Saint Paul – Ramsey County Public Health
90 West Plato Blvd – Suite 200
St. Paul, Mn 55107 – (651)266-2592
Pat Hadfield, RN, MS
Hennepin County Medical Center (HCMC)
715 Park Ave. So., Mpls, MN 55415 ; (612) 873-2668