case i - kvrwg.org · functional classification i. ordinary physical activity does not cause ii....
TRANSCRIPT
CASE I
C.C. : chest pain
D. : 6 months
P. I. : 본 74세 여환은 20 년 전부터 HTN 있어 local
에서 medication 중으로 내원 6 개월 전부터
exertional chest pain 있어 further evaluation 및
proper management 위해 내원함.
F/74 이 O 인 #4615763
Chest pain profile
Onset : 6개월전
Duration : 10 mins
Frequency : 1~2회/주
Character : squeezing
Location : substernum
Radiation : Lt. arm and neck
Associative Sx : none
Relieving Fx : rest
Aggravating Fx : exertion
Risk Fx : HTN, age
NTG response : no response
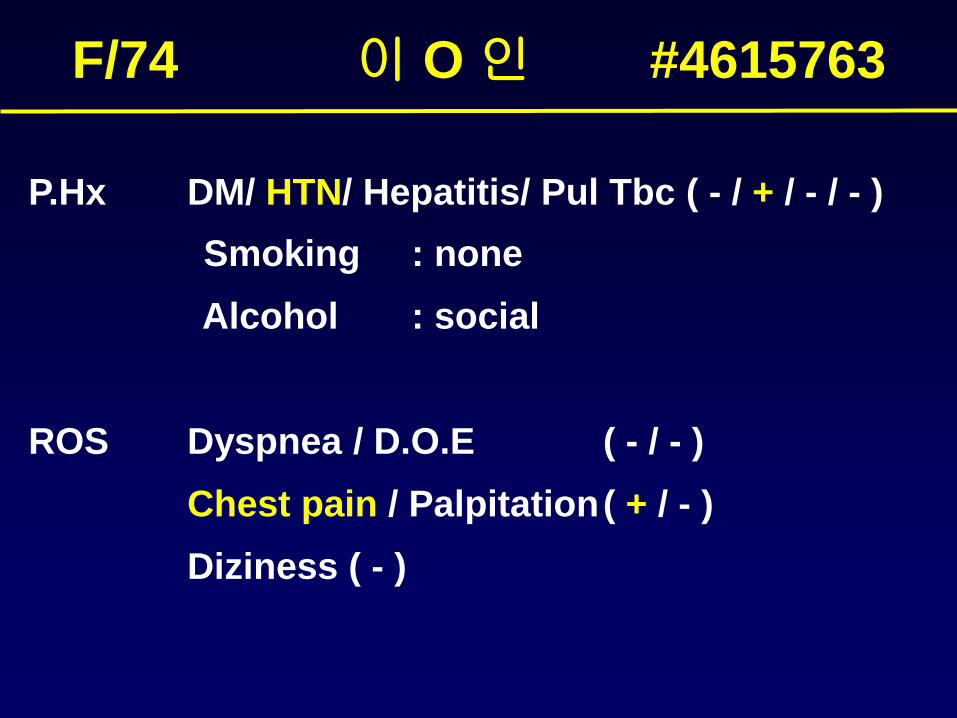
P.Hx DM/ HTN/ Hepatitis/ Pul Tbc ( - / + / - / - )
Smoking : none
Alcohol : social
ROS Dyspnea / D.O.E ( - / - )
Chest pain / Palpitation( + / - )
Diziness ( - )
F/74 이 O 인 #4615763
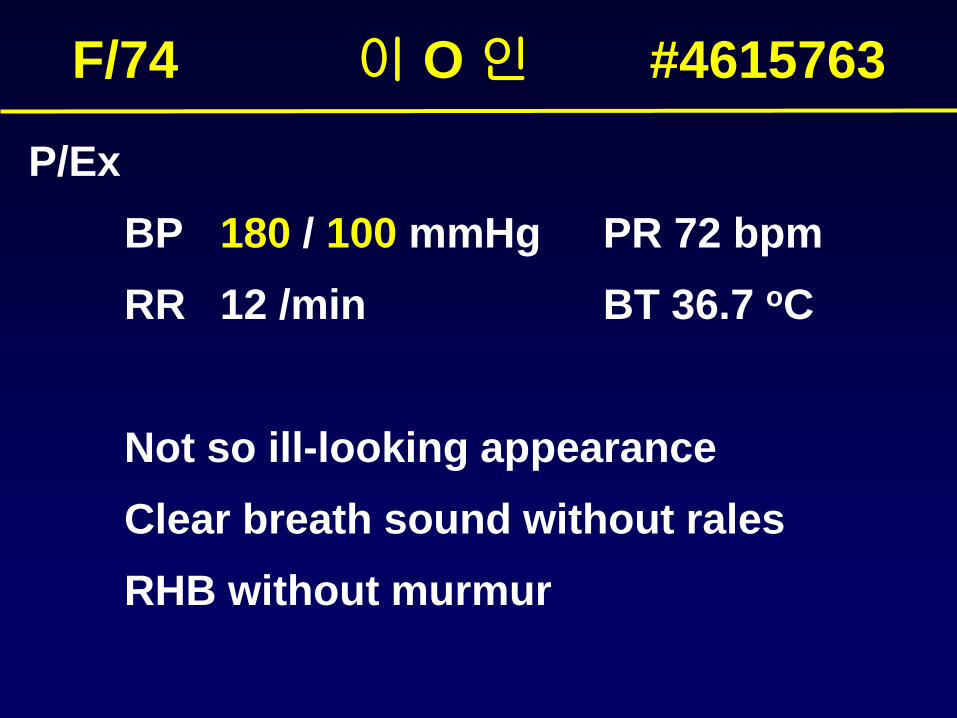
P/Ex
BP 180 / 100 mmHg PR 72 bpm
RR 12 /min BT 36.7 oC
Not so ill-looking appearance
Clear breath sound without rales
RHB without murmur
F/74 이 O 인 #4615763
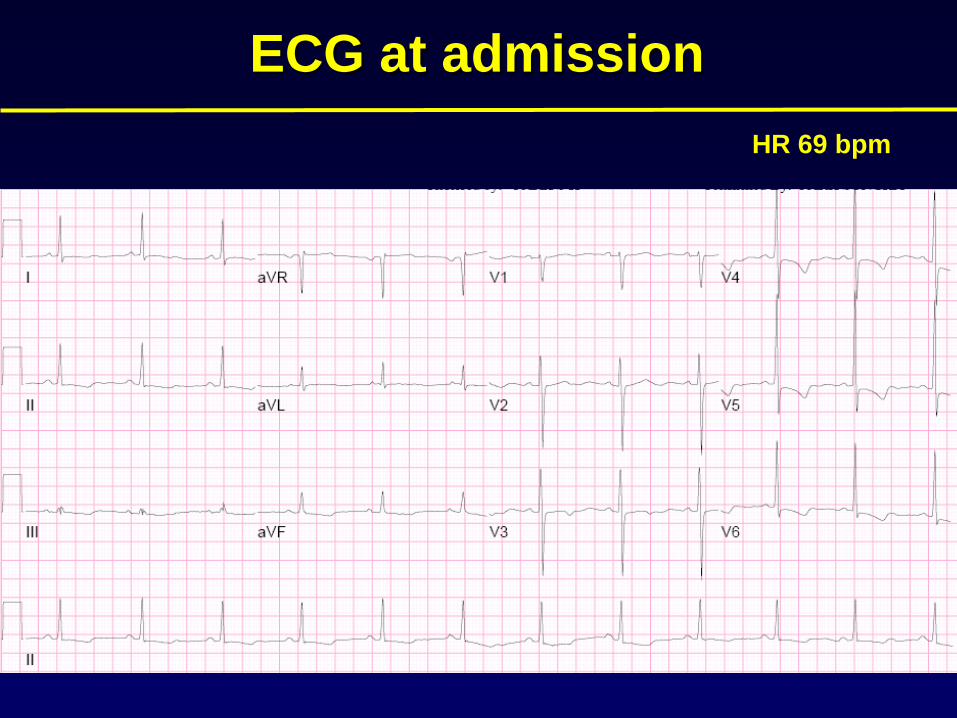
ECG at admission
HR 69 bpm
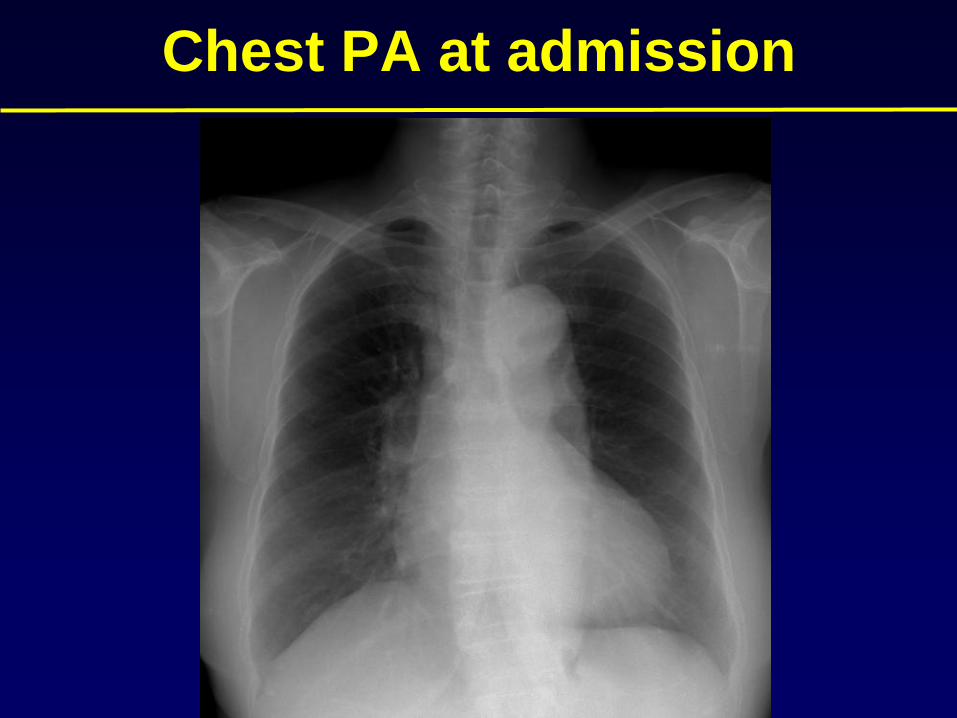
Chest PA at admission
Laboratory
CBC : 7610/14.6/221k
BUN/Cr : 24/0.8
T.chol/TG/HDL/LDL: 179/459/39/79
Random glucose : 111
Echocardiography
Normal global LV systolic function
(EF=60 %)
Borderline enlarged LA
(volume index : 28.2 ml/m2)
No RWMA
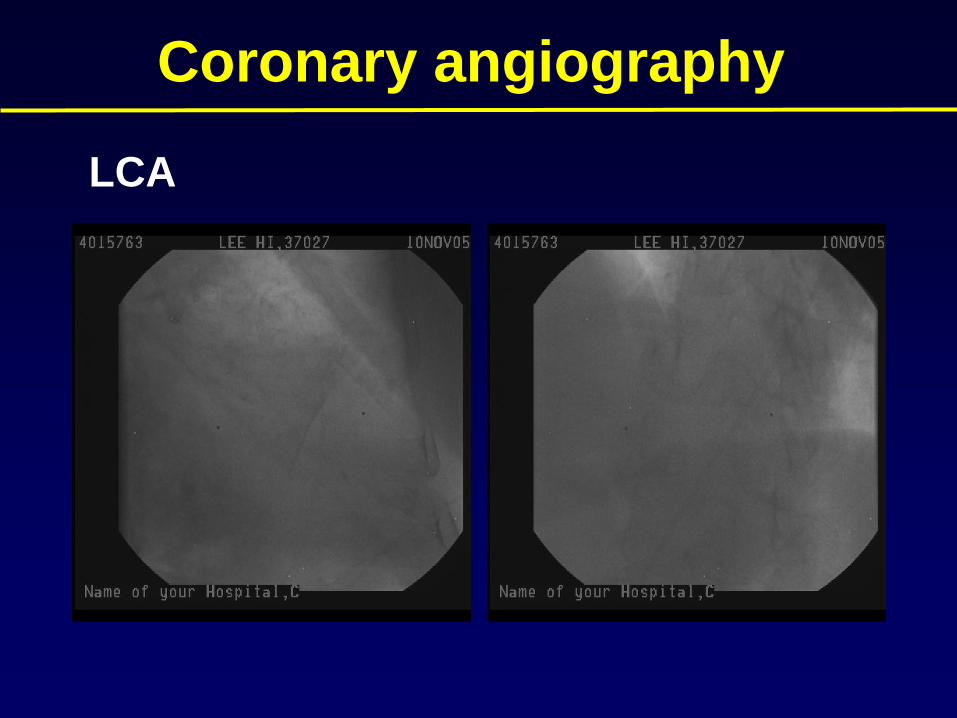
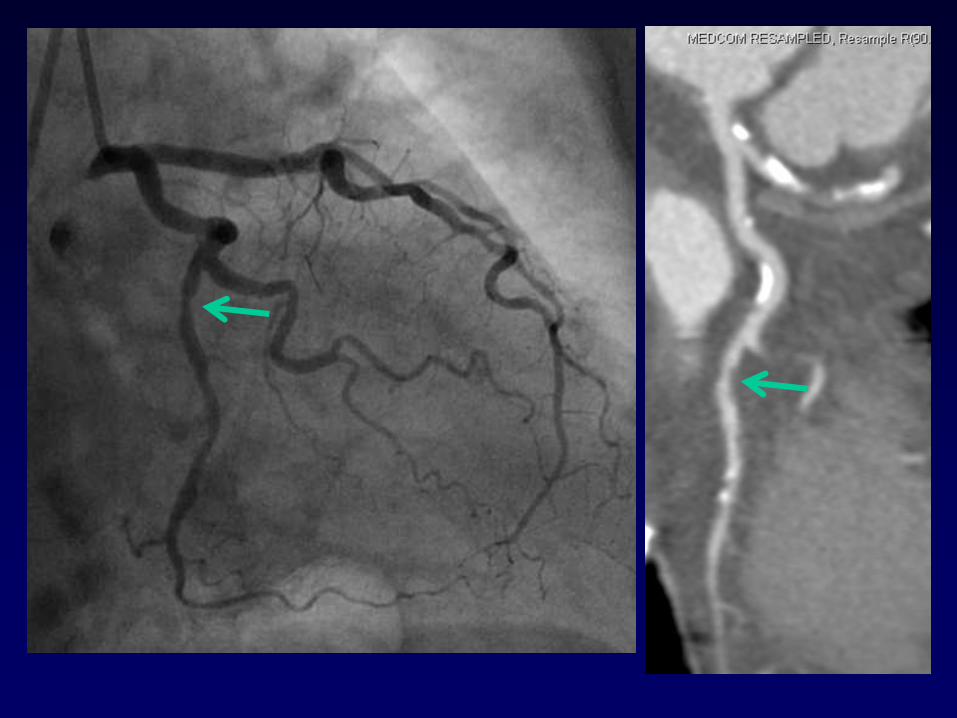
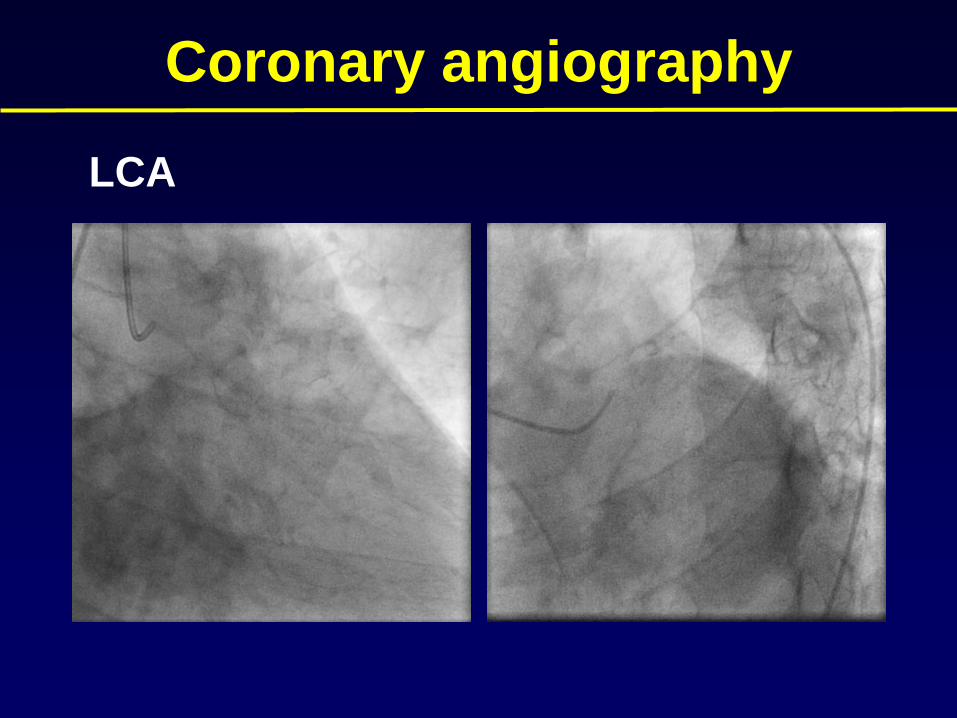
Coronary angiography
LCA
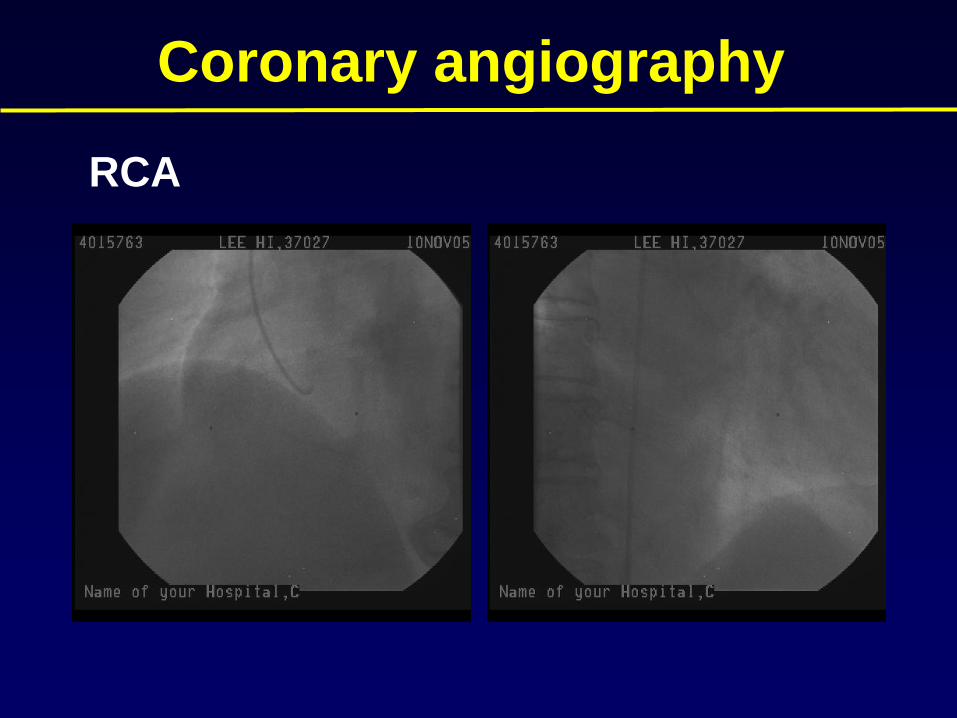
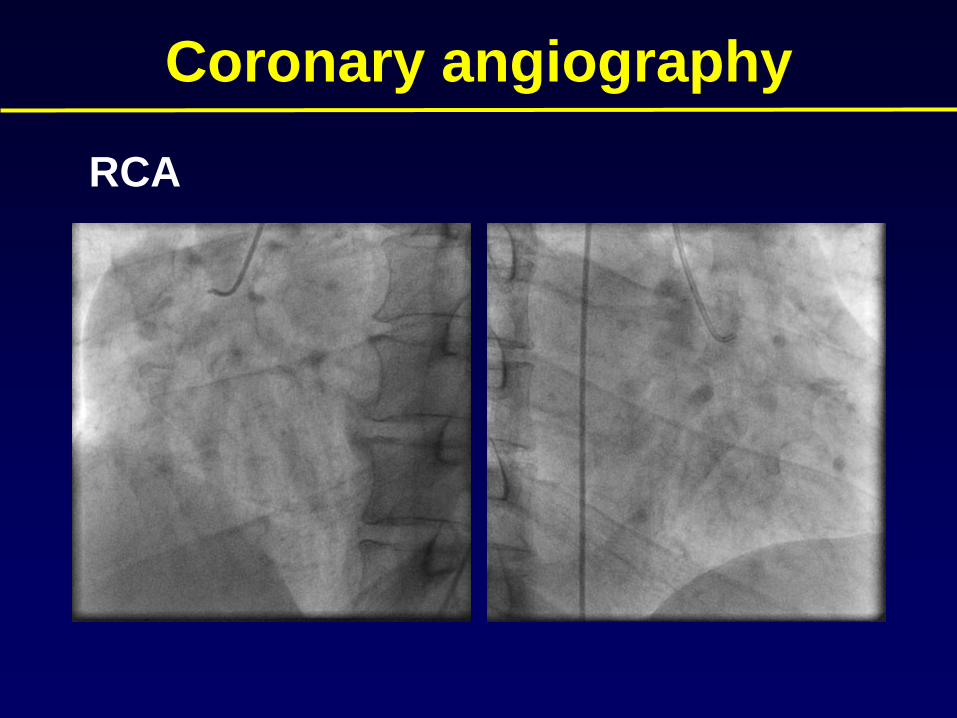
Coronary angiography
RCA
Treatment options for this patient
• Medical treatment
• PCI: but where?
• CABG: Poor anatomy and patient refusal
Optimal medical treatment is still a viable option
Grading of Angina Pectoris
Canadian Cardiovascular Society (CCS)
Functional Classification:
modification of the New York Heart Association (NYHA)
Functional Classification
I. Ordinary physical activity does not cause
II. Ordinary physical activity results in
III. Less than ordinary physical activity causes
IV. anginal syndrome may be present at rest
# Ordinary physical activity (undue fatigue) :
Walking one to two blocks or
climbing more than one flight
Risk Stratification
• The severity of angina:
also an important predictor of
outcome
• Normal resting ECG in stable angina
pectoris: well-preserved LV Fx. and
a favorable long-term prognosis.
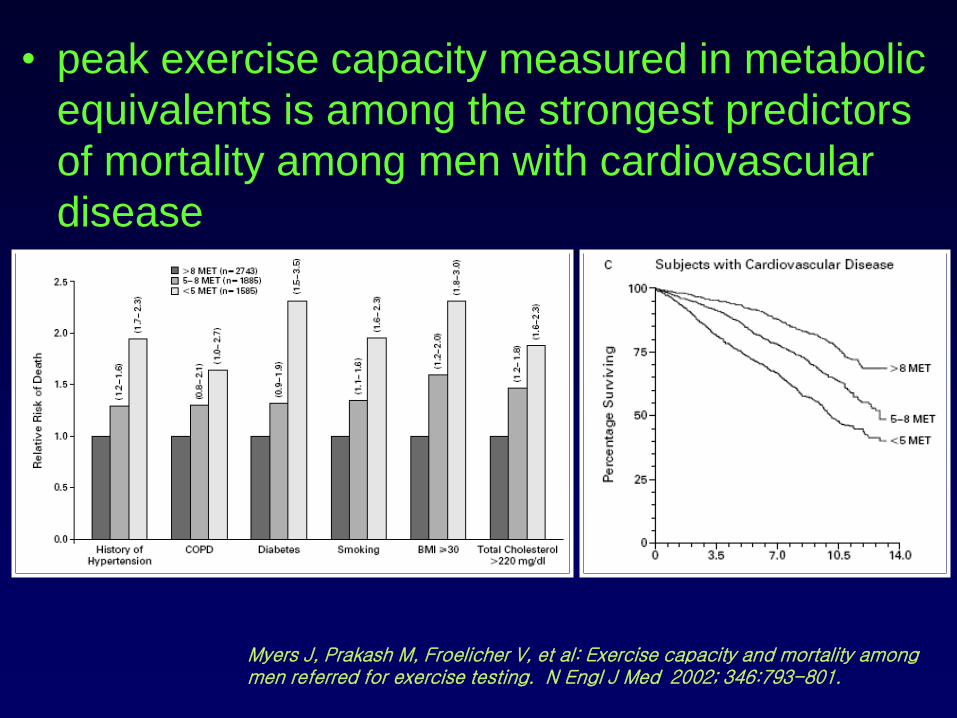
• peak exercise capacity measured in metabolic
equivalents is among the strongest predictors
of mortality among men with cardiovascular
disease
Myers J, Prakash M, Froelicher V, et al: Exercise capacity and mortality among men referred for exercise testing. N Engl J Med 2002; 346:793-801.
Risk Stratification Based on
Noninvasive Testing
High Risk (>3% annual mortality rate)
• Severe resting LV dysFx. (EF < 0.35)
• RWMA (involving > two segments)
• High-risk TMT result
• large perfusion defect
• multiple perfusion defect
• increased lung uptake (in thallium-201 scan)
Committee to update the 1999 guidelines for the management of patients with chronic stable angina). 2002 American College of Cardiology and American Heart Association
Meaning of These Feature
• Regardless of the severity of symptoms
• high likelihood of CAD
• risk for left main or triple-vessel CAD
impaired left ventricular function
• high risk for experiencing coronary events
↓
should undergo coronary arteriography
Comprehensive management of
Chronic Coronary Artery Disease
(1) Lifestyle modification for
reduction of coronary risk factors
(2) Treatment of associated diseases
that can precipitate or worsen angina
(3) Pharmacological management
(4) Revascularization (PCI or CABG)
PCI vs Medical
• Over 20,000 cases/year in Korea
Over 1,000,000 cases/year in US
Over 2,000,000 cases/year worldwide
• Superior control of angina
• Improved exercise capacity
• Improved quality of life
• No randomized trial has demonstrated a reduction
in death or MI with PCI compared to medical Tx.
for chronic stable angina
Class I indication
• Disabling chronic stable angina(CCS III or IV)
despite medical therapy
• High risk criteria on clinical assessment or
non invasive testing regardless of symptom
• Angina patients who survived sudden cardiac
death or serious ventricular arrhythmia
• Angina patients with CHF symptom and sign
Gibbons et al. 2002 ACC/AHA Practice Guidelines
• Randomized controlled trial:
Clinical Outcomes Utilizing Revascularization and
Aggressive druG Evaulation (COURAGE trial)
• 50 U.S. and Canadian Centers
• 2287 patients, 1999~2004
• Inclusion
CCS I~III stable angina stable post MI asymptomatic patients:angiographically documented CAD with at least 1 vessel
• Exclusion
persistent CCS IV refractory to medical Tx.Unstable anginaunstable post MILt.main > 50%LVEF < 30%markedly positive stress test
• Initial treatment Strategy randomization1138: optimal medical Tx.1149: PCI + optimal medical Tx.
• Optimal medical Tx:aspirin, clopidogrel, simvastatin, metoprolol and/or amlodipine, lisinopril or losartan, long-acting nitrates, as well as lifestyle change
• PCI:performed within 105 days of diagnostic angio
• Primary end point: Death / non fatal MI
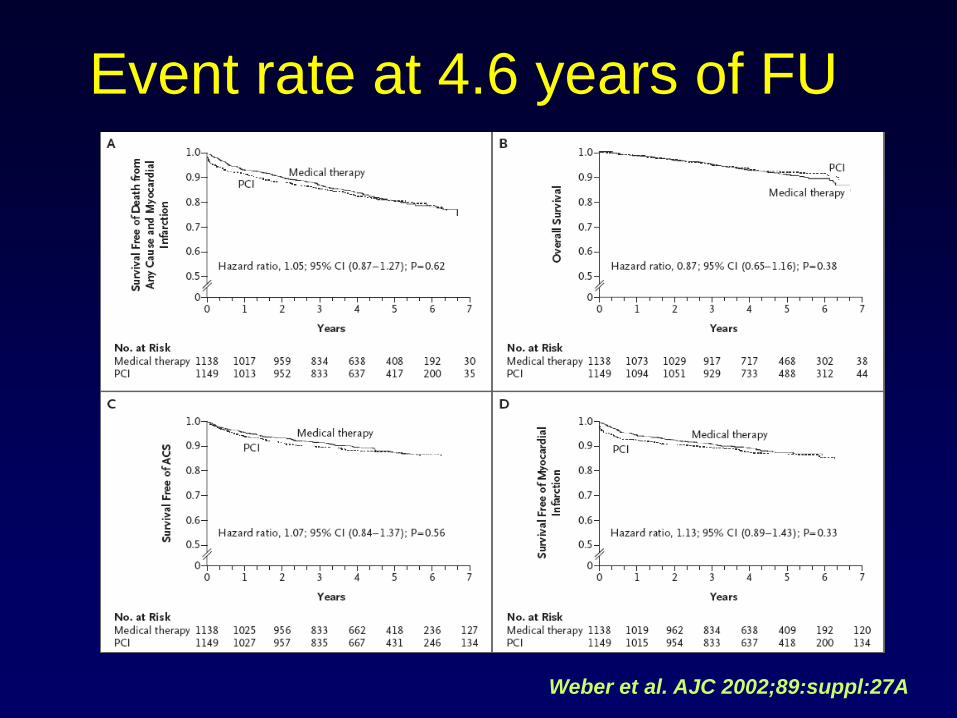
Event rate at 4.6 years of FU
Weber et al. AJC 2002;89:suppl:27A
1. Aspirin in the absence of contraindication
2. Beta-blockers as initial therapy in the absence of contraindications
3. ACE inhibitor in patients with CAD
who also have diabetes and/or
left ventricular systolic dysfunction.
4. Calcium antagonists and/or long acting nitrates
as initial therapy or reduction of symptoms
when beta blockers are contraindicated
or not successful or unacceptable side effects
5. Sublingual or spray of NTG
for immediate relief of angina
6. target LDL of less than 100 mg/dL.
Gibbons et al. ACC/AHA practice guideline 2002
Class I
1. Clopidogrel when aspirin is absolutely contraindicated
2. Calcium antagonists instead of beta blockers as initial
therapy
3. ACE inhibitor in all patients with CAD or other vascular
disease.
Gibbons et al. ACC/AHA practice guideline 2002
Class IIa
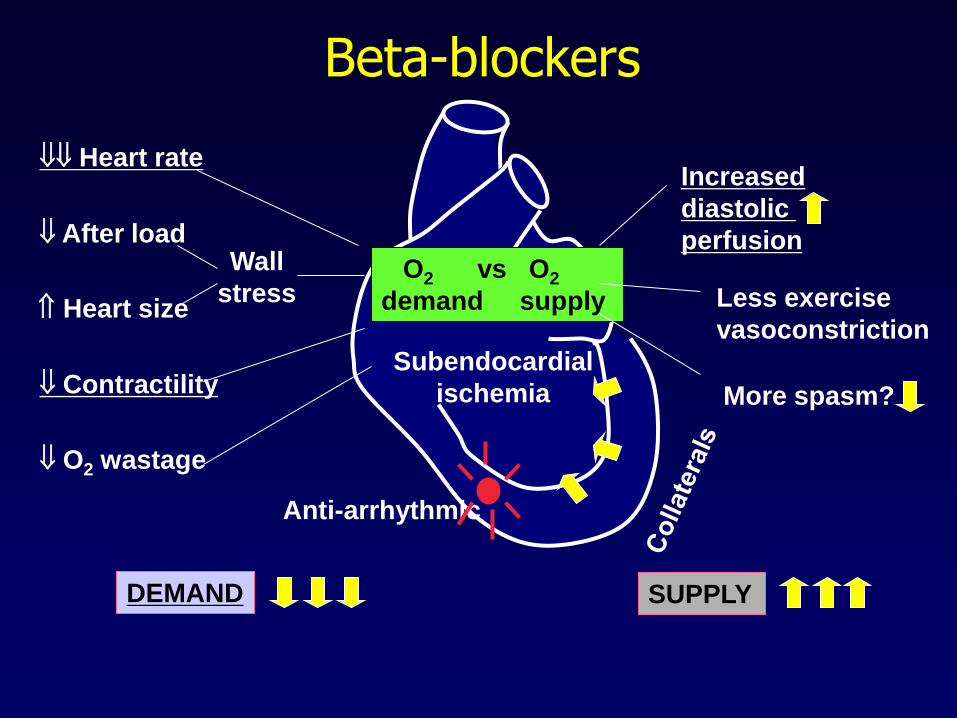
Beta-blockers
Increased
diastolic
perfusion
Less exercise
vasoconstriction
More spasm?
Heart rate
After load
Heart size
Contractility
O2 wastage
Anti-arrhythmic
DEMAND SUPPLY
Subendocardial
ischemia
O2 vs O2
demand supply
Wall
stress
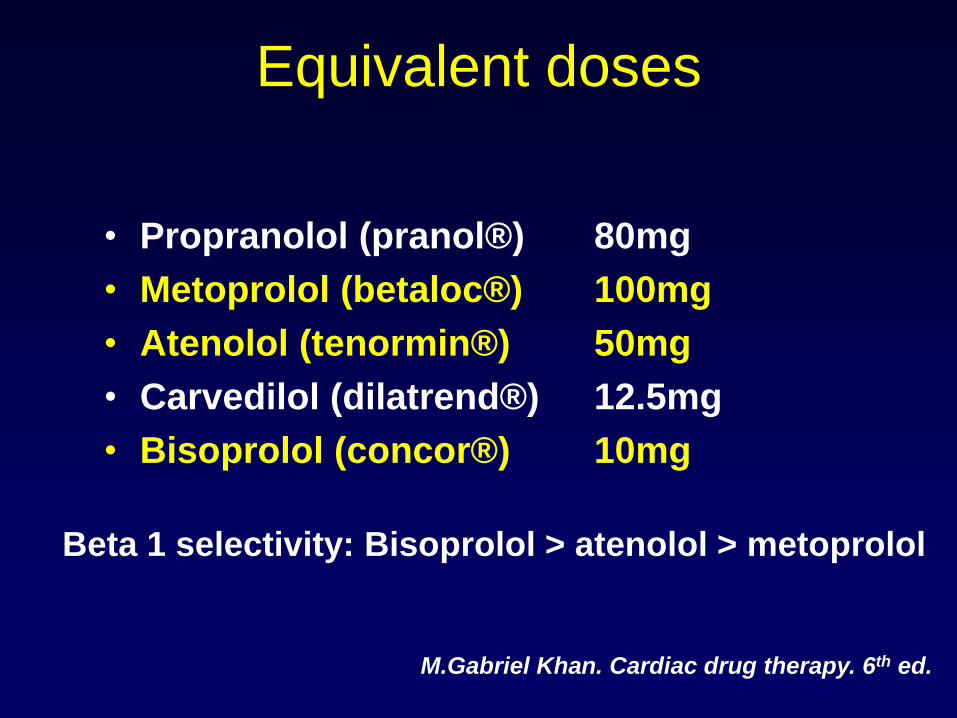
Equivalent doses
• Propranolol (pranol® )
• Metoprolol (betaloc® )
• Atenolol (tenormin® )
• Carvedilol (dilatrend® )
• Bisoprolol (concor® )
80mg
100mg
50mg
12.5mg
10mg
Beta 1 selectivity: Bisoprolol > atenolol > metoprolol
M.Gabriel Khan. Cardiac drug therapy. 6th ed.
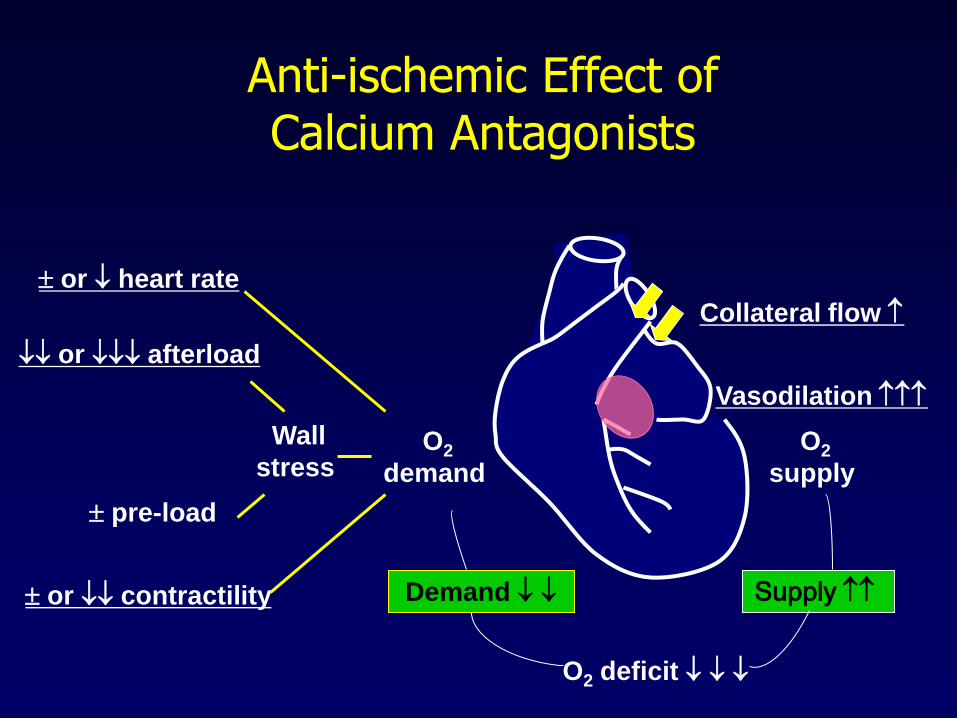
Supply
Anti-ischemic Effect of Calcium Antagonists
Collateral flow
Vasodilation
Demand
O2
demand
Wall
stress
pre-load
or contractility
or afterload
or heart rate
O2 deficit
O2
supply
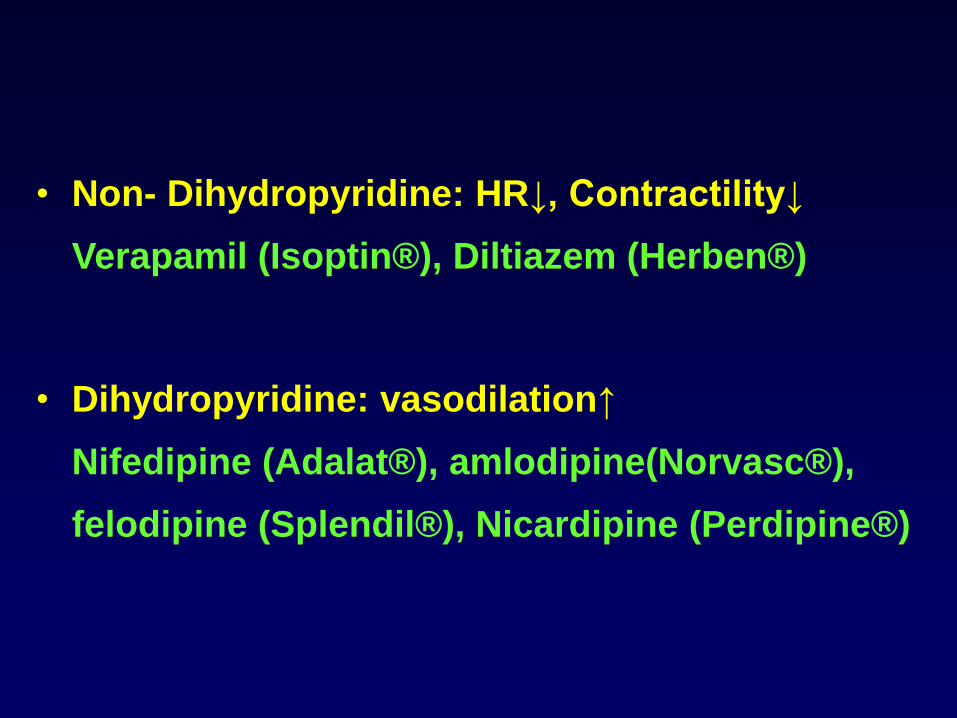
• Non- Dihydropyridine: HR↓, Contractility↓
Verapamil (Isoptin® ), Diltiazem (Herben® )
• Dihydropyridine: vasodilation↑
Nifedipine (Adalat® ), amlodipine(Norvasc® ),
felodipine (Splendil® ), Nicardipine (Perdipine® )
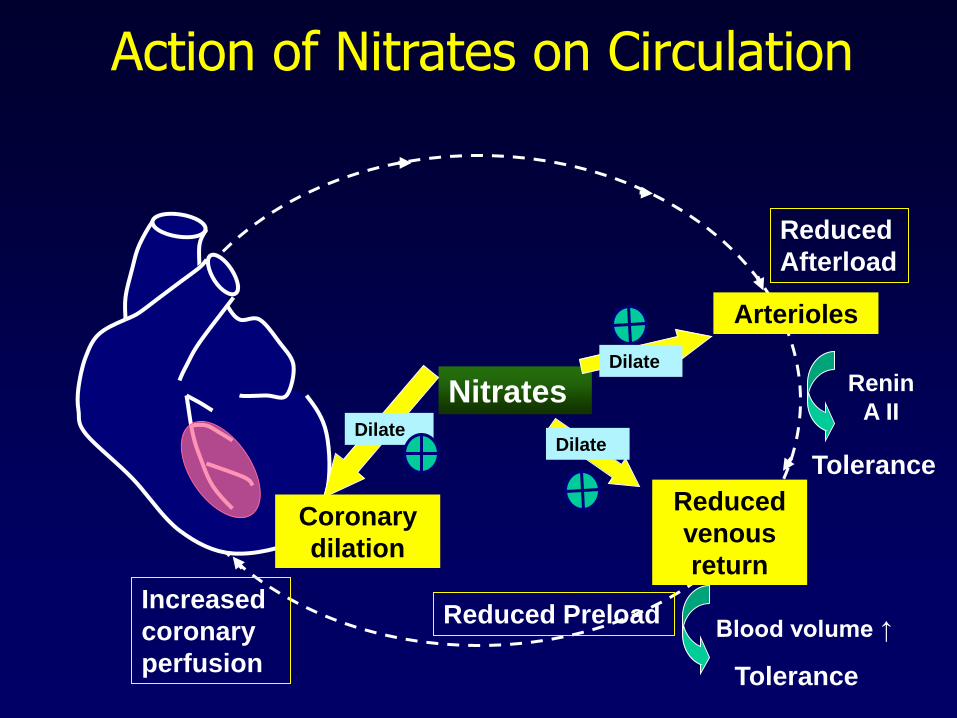
Reduced
venous
return
Arterioles
Reduced
Afterload
Reduced Preload
Nitrates
Action of Nitrates on Circulation
DilateDilate
Tolerance
Renin
A II
Dilate
Tolerance
Blood volume ↑
Coronary
dilation
Increased
coronary
perfusion
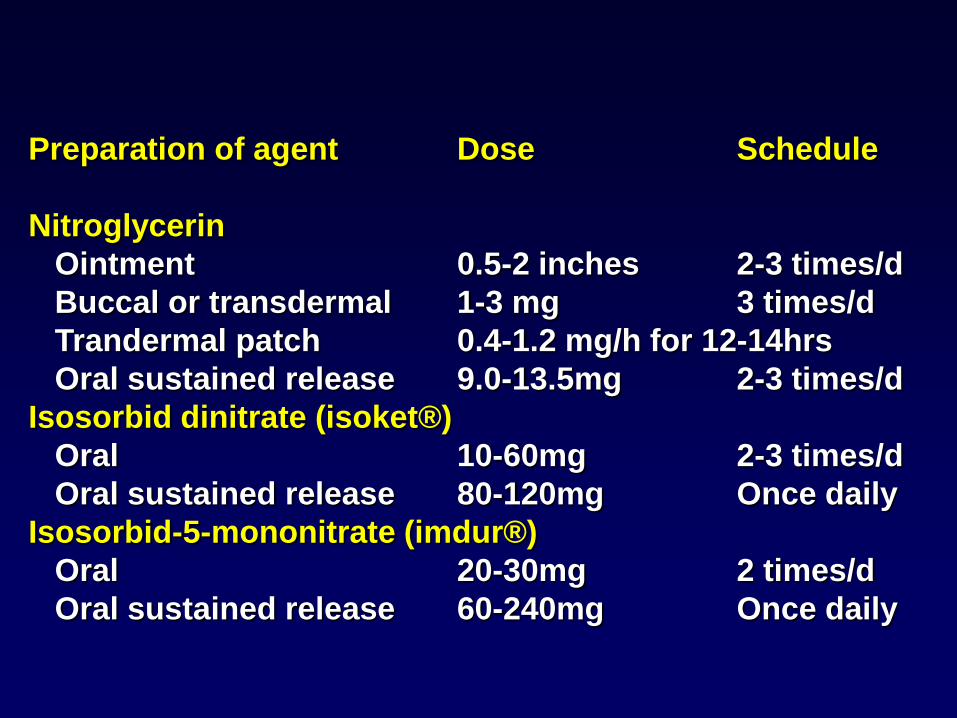
Preparation of agent Dose Schedule
Nitroglycerin
Ointment 0.5-2 inches 2-3 times/d
Buccal or transdermal 1-3 mg 3 times/d
Trandermal patch 0.4-1.2 mg/h for 12-14hrs
Oral sustained release 9.0-13.5mg 2-3 times/d
Isosorbid dinitrate (isoket® )
Oral 10-60mg 2-3 times/d
Oral sustained release 80-120mg Once daily
Isosorbid-5-mononitrate (imdur® )
Oral 20-30mg 2 times/d
Oral sustained release 60-240mg Once daily
Other Anti-angina drug
• Potassium channel opener
- Nicorandil : Sigmart®
• Direct NO donor
- Molsidomine : Molsiton®
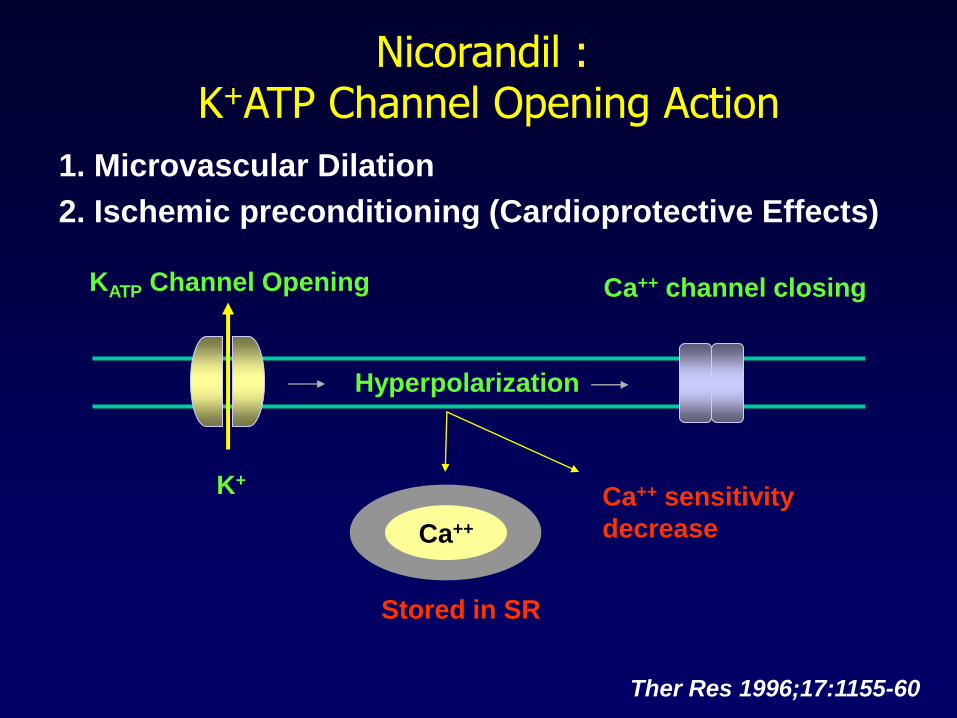
Nicorandil :K+ATP Channel Opening Action
1. Microvascular Dilation
2. Ischemic preconditioning (Cardioprotective Effects)
KATP Channel Opening
K+
Hyperpolarization
Ca++ channel closing
Ca++
Stored in SR
Ca++ sensitivity
decrease
Ther Res 1996;17:1155-60
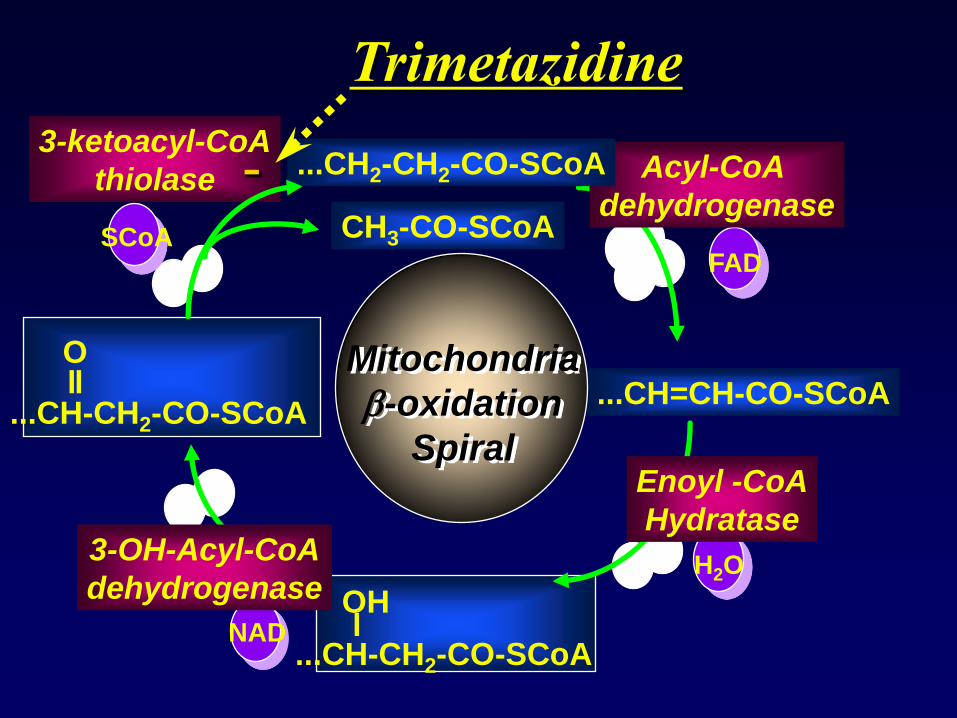
...CH=CH-CO-SCoA
3-ketoacyl-CoA
thiolase
...CH-CH2-CO-SCoA
Oll
...CH-CH2-CO-SCoA
OHl
H2O
NAD
SCoAFAD
Mitochondria
-oxidation
Spiral
CH3-CO-SCoA
Enoyl -CoA
Hydratase
Acyl-CoA
dehydrogenase
...CH2-CH2-CO-SCoA
3-OH-Acyl-CoA
dehydrogenase
-
Trimetazidine
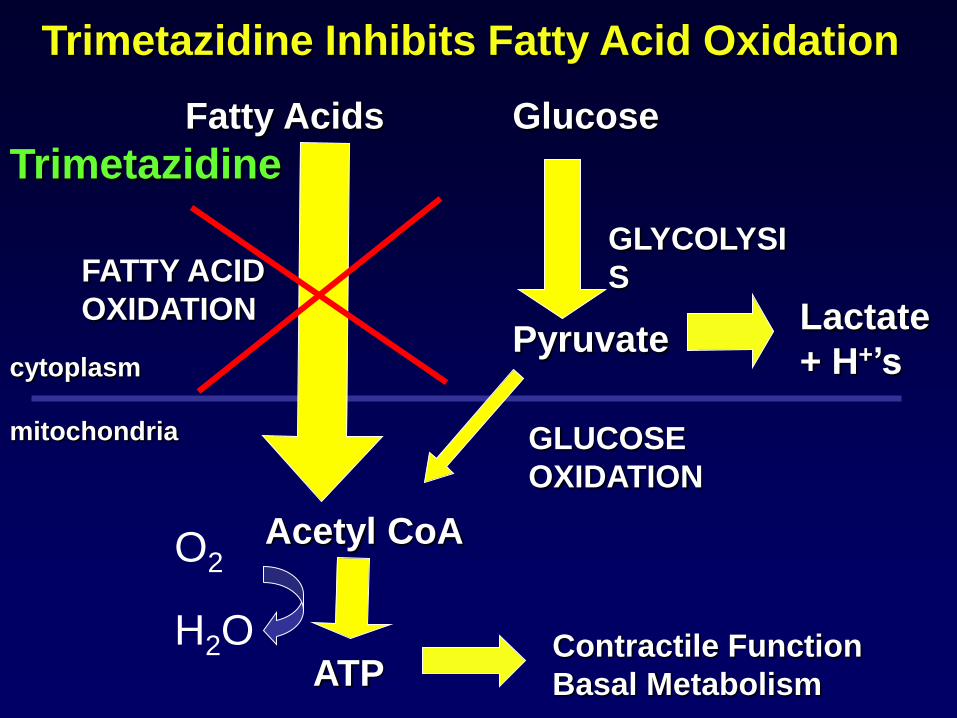
mitochondria
cytoplasm
FATTY ACID
OXIDATION
GLUCOSE
OXIDATION
GLYCOLYSI
S
Acetyl CoA
ATPContractile Function
Basal Metabolism
Pyruvate
Fatty Acids Glucose
Trimetazidine Inhibits Fatty Acid Oxidation
Lactate
+ H+’s
Trimetazidine
O2
H2O
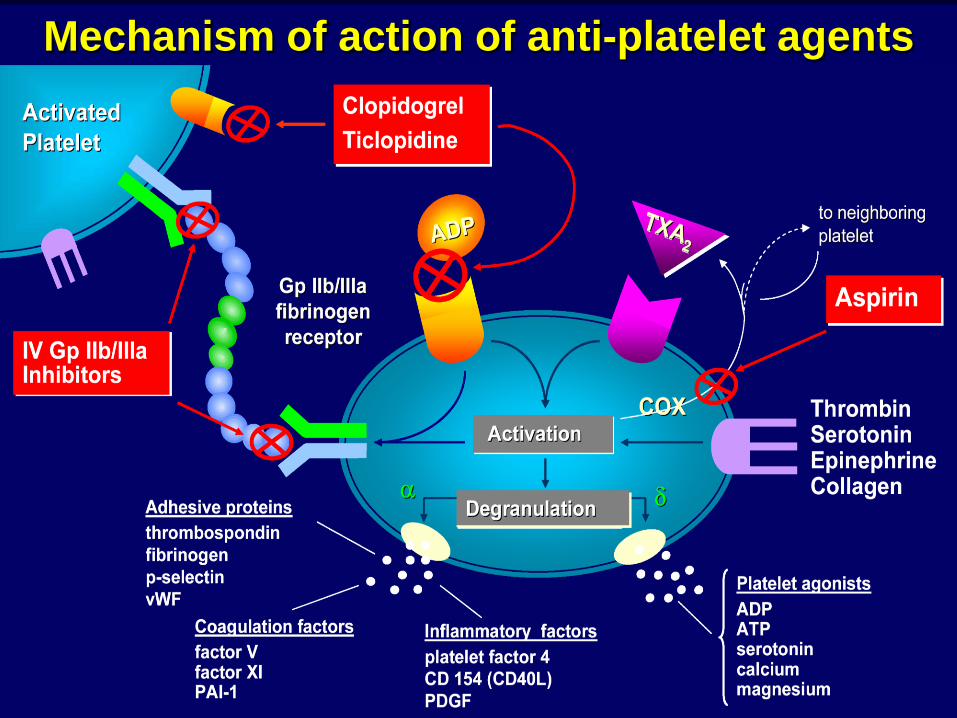
Mechanism of action of anti-platelet agents
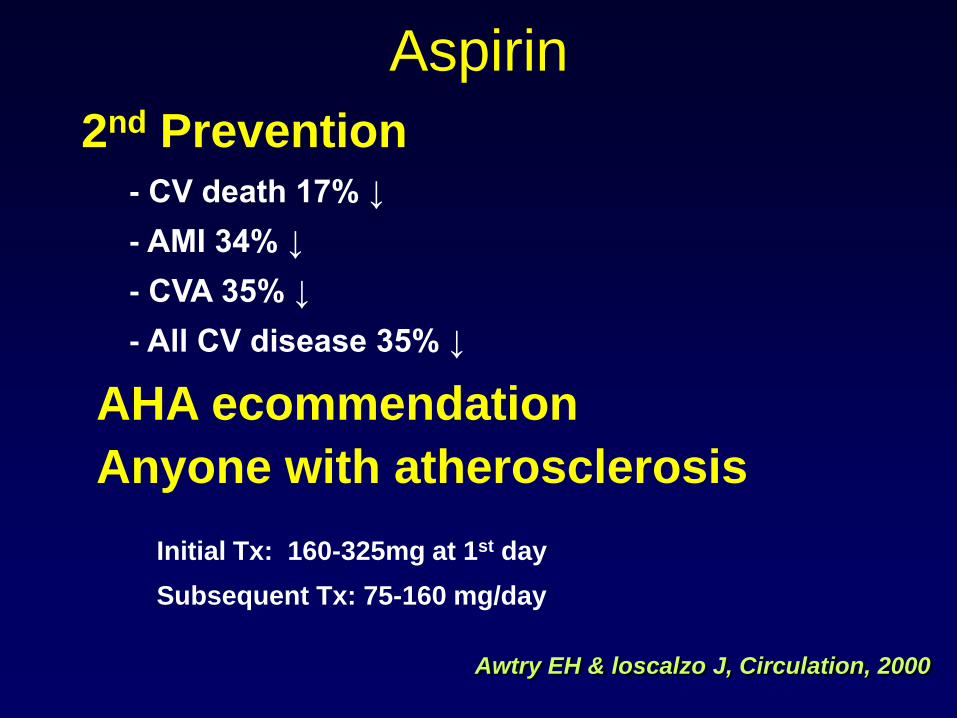
Aspirin
Awtry EH & loscalzo J, Circulation, 2000
2nd Prevention- CV death 17% ↓
- AMI 34% ↓
- CVA 35% ↓
- All CV disease 35% ↓
AHA ecommendation
Anyone with atherosclerosis
Initial Tx: 160-325mg at 1st day
Subsequent Tx: 75-160 mg/day
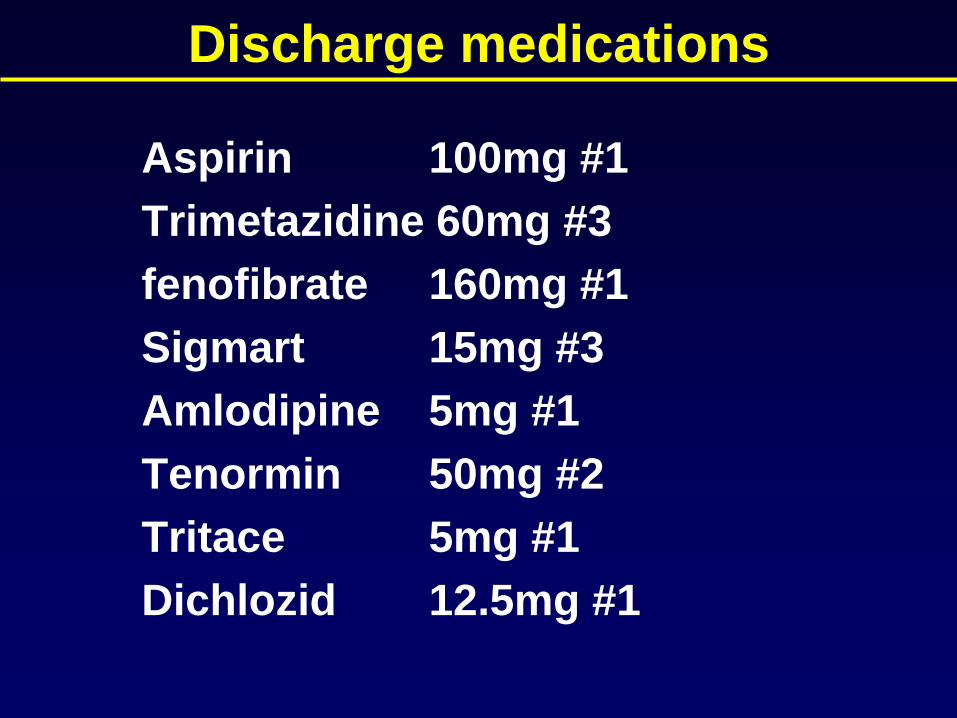
Discharge medications
Aspirin 100mg #1
Trimetazidine 60mg #3
fenofibrate 160mg #1
Sigmart 15mg #3
Amlodipine 5mg #1
Tenormin 50mg #2
Tritace 5mg #1
Dichlozid 12.5mg #1
CASE II
C.C. : chest pain
D. : 1 month
P. I. : 본 65세 남환은 2006년 본원에서 colon
polypectomy 시행 받은 Hx 외에는 특이 과거력 없는
분으로 내원 1 개월 동안의 chest pain 주소로
further evaluation and proper management 위해
내원함.
M/65 김 O 영 #5171606
Chest pain profile
Onset : 3개월전
Duration : several mins
Frequency : 2~3회/day
Character : 뜨금한 느낌
Location : substernum
Radiation : none
Associative Sx : sweating
Relieving Fx : resting
Aggravating Fx : exertion(Canadian class II)
Risk Fx : age
NTG response : not trial
P.Hx DM/ HTN/ Hepatitis/ Pul Tbc ( - / - / - / - )
Smoking : none
Alcohol : social
ROS Dyspnea / D.O.E ( - / - )
Chest pain / Palpitation( + / - )
Diziness / Headache ( - / - )
M/65 김 O 영 #5171606
P/Ex
BP 120 / 60 mmHg PR 88 bpm
RR 12 /min BT 36.7 oC
Not so ill-looking appearance
Clear breath sound without rales
RHB without murmur
M/65 김 O 영 #5171606
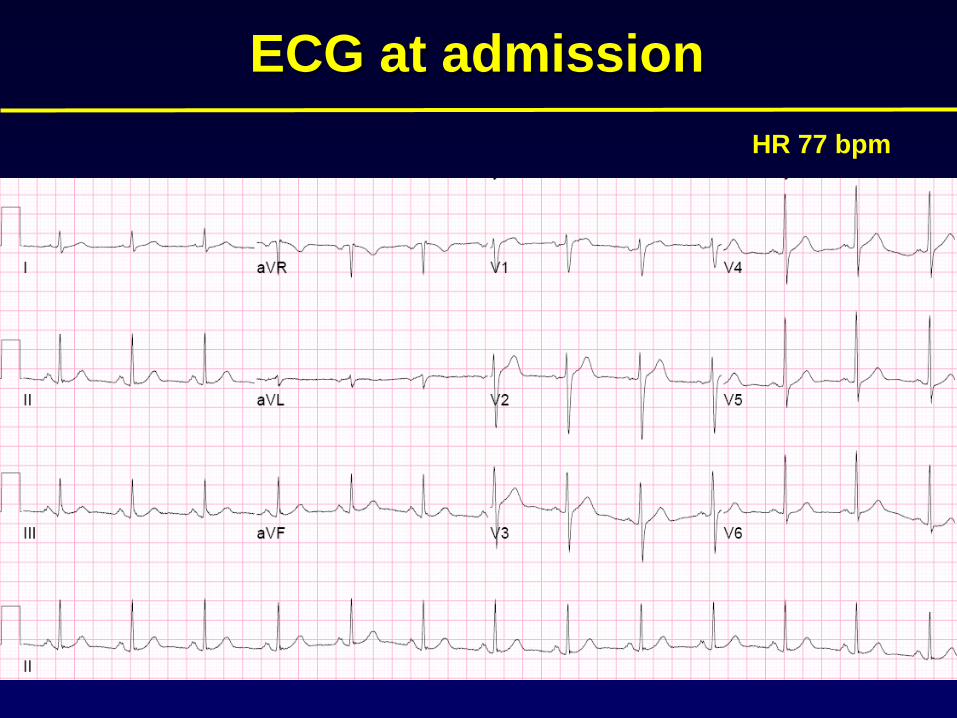
ECG at admission
HR 77 bpm
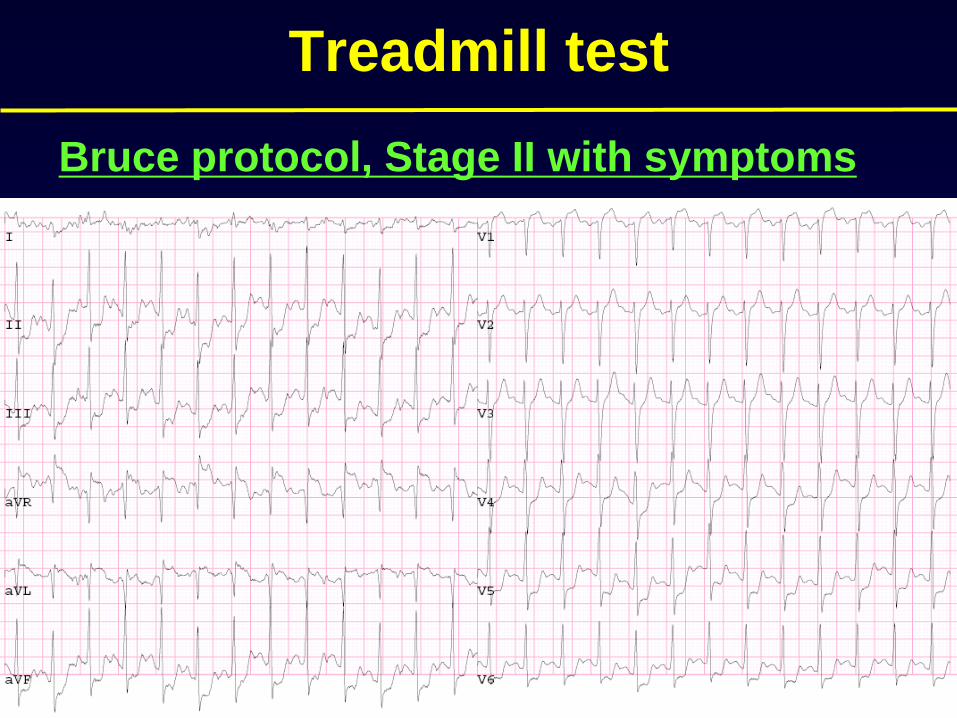
Treadmill test
Bruce protocol, Stage II with symptoms
Echocardiography
Normal global LV systolic function
(EF=76 %)
No RWMA
Coronary angiography
LCA
Coronary angiography
RCA
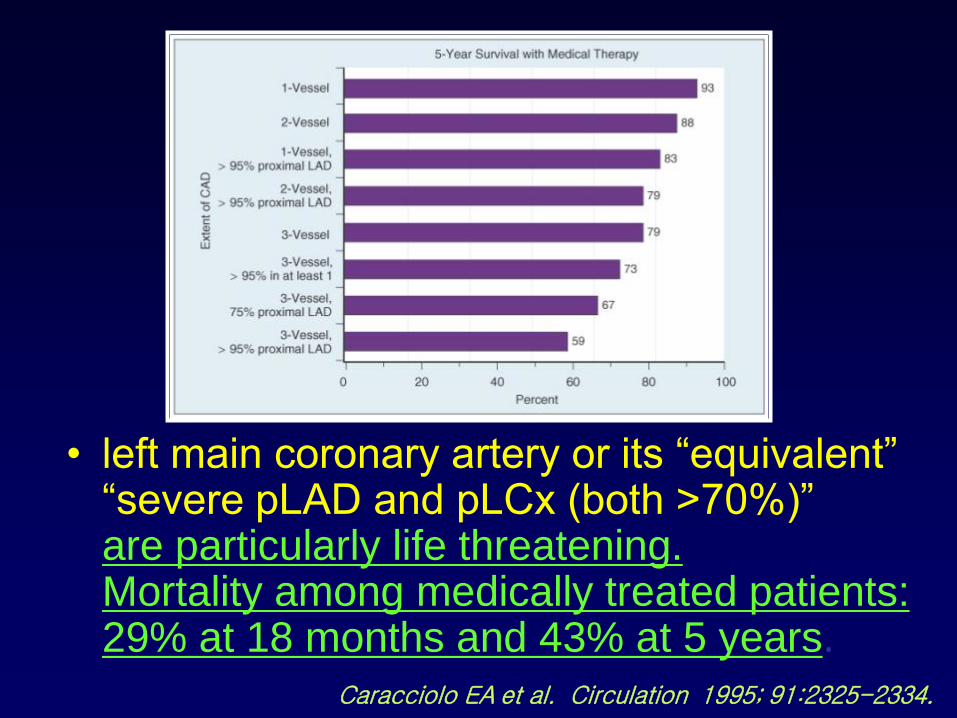
• left main coronary artery or its “equivalent” “severe pLAD and pLCx (both >70%)”are particularly life threatening.Mortality among medically treated patients:29% at 18 months and 43% at 5 years.
Caracciolo EA et al. Circulation 1995; 91:2325-2334.
CABG• Around 2500 cases/year in Korea (in 2002)
Around 350,000 cases/year in US
20% of CABG is off pump
• excellent short- and intermediate-term results
in the management of stable CAD
• 80% free of angina at 5 years
63% at 10 years, but only 15% after 15years
• long-term results are affected by failure of
venous grafts
Abu-Omar Y, Taggart DP: Off-pump coronary artery bypass grafting. Lancet 2002; 360:327-330
• CABG for Lt. main
• CABG for 3VD
• CABG for 2VD with significant pLAD with abnormal LV Fx.
• PCI for 2 or 3VD with significant pLADwith suitable anatomy and normal LV Fx and no DM
- recurrent angina, repeat revascularization due to
incomplete revascularization and restenosis of PCI
- survival benefit from CABG in left ventricular dysfunction,
proximal LAD stenosis, DM
PCI vs CABG
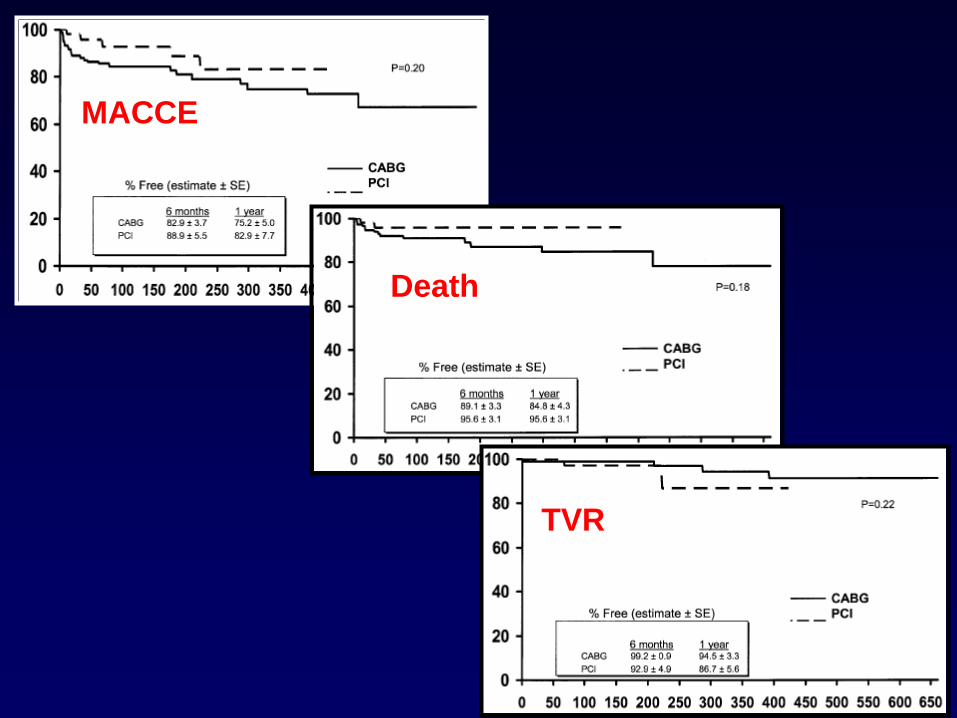
MACCE
Death
TVR
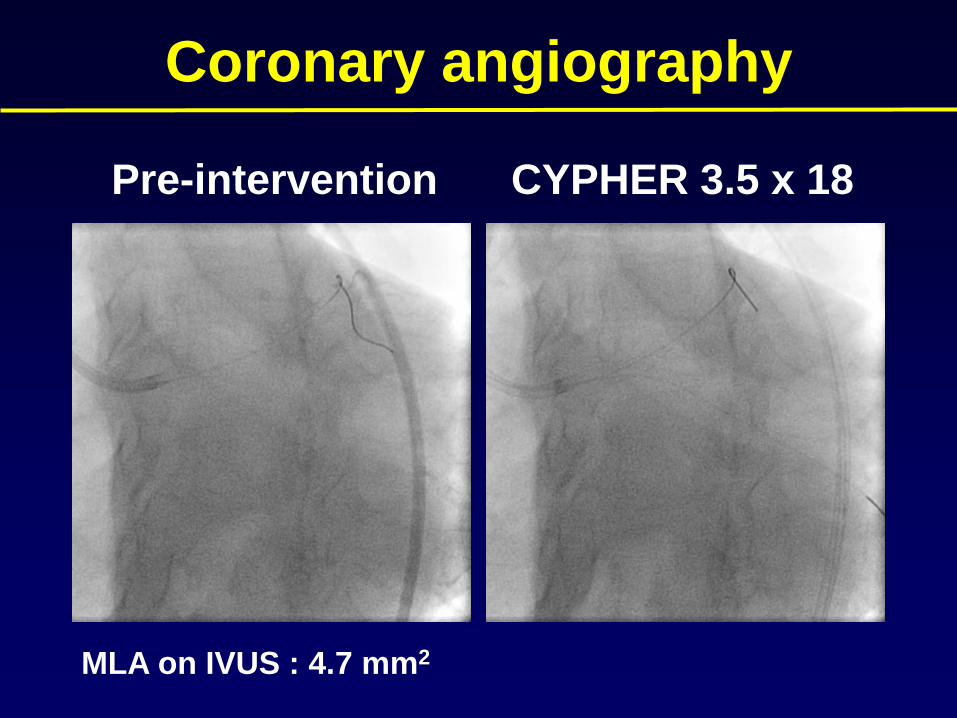
Coronary angiography
Pre-intervention CYPHER 3.5 x 18
MLA on IVUS : 4.7 mm2
Discharge medications
Aspirin 100mg #1
Plavix 75mg #1
Pletaal 200mg #2
Lipitor 40mg #1
Sigmart 10mg #2
Tenormin 50mg #1
Capril 18.75mg #3
CASE III
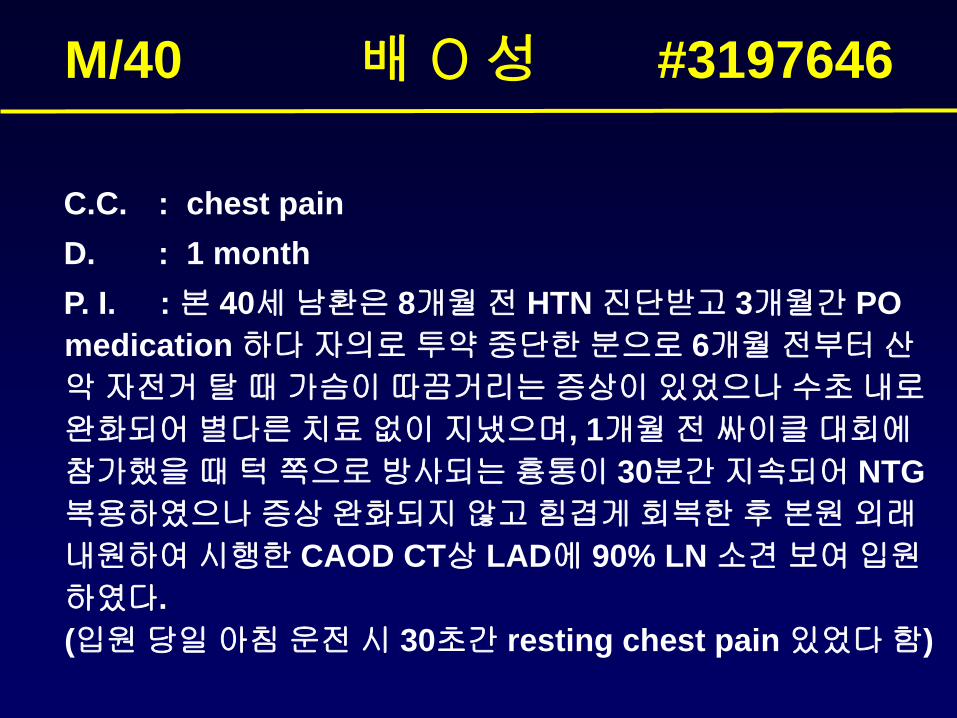
C.C. : chest pain
D. : 1 month
P. I. : 본 40세 남환은 8개월 전 HTN 진단받고 3개월간 PO
medication 하다 자의로 투약 중단한 분으로 6개월 전부터 산
악 자전거 탈 때 가슴이 따끔거리는 증상이 있었으나 수초 내로
완화되어 별다른 치료 없이 지냈으며, 1개월 전 싸이클 대회에
참가했을 때 턱 쪽으로 방사되는 흉통이 30분간 지속되어 NTG
복용하였으나 증상 완화되지 않고 힘겹게 회복한 후 본원 외래
내원하여 시행한 CAOD CT상 LAD에 90% LN 소견 보여 입원
하였다.
(입원 당일 아침 운전 시 30초간 resting chest pain 있었다 함)
M/40 배 O 성 #3197646
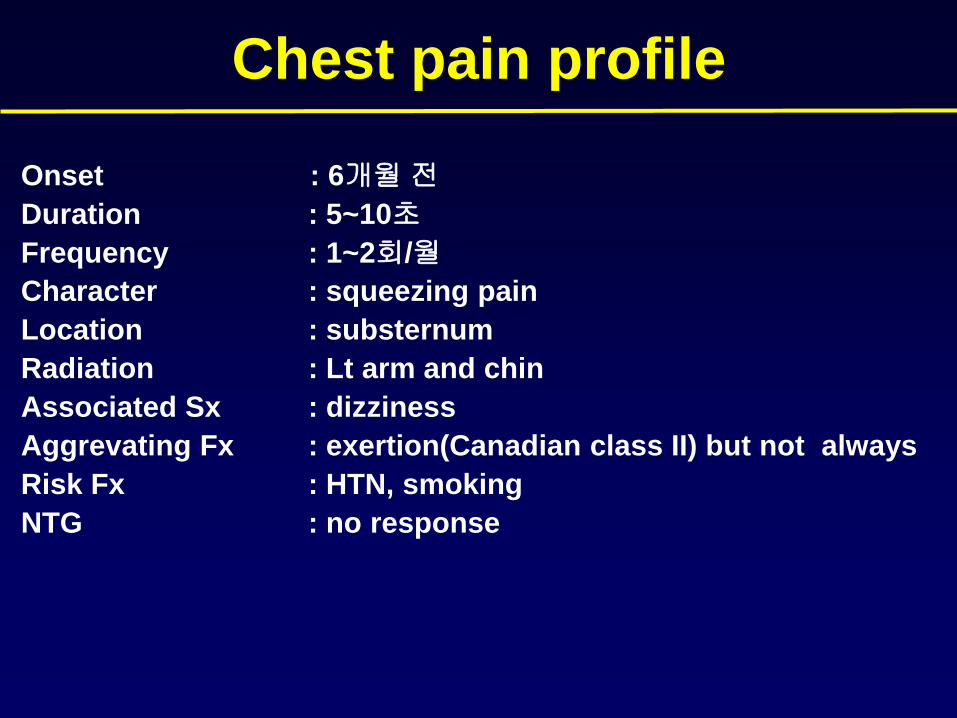
Chest pain profile
Onset : 6개월 전
Duration : 5~10초
Frequency : 1~2회/월
Character : squeezing pain
Location : substernum
Radiation : Lt arm and chin
Associated Sx : dizziness
Aggrevating Fx : exertion(Canadian class II) but not always
Risk Fx : HTN, smoking
NTG : no response
P.Hx DM/ HTN/ Hepatitis/ Pul Tbc ( - / + / - / )
Smoking : 40PYRs, current smoker
Alcohol : social
Hyperthyroidism
ROS Dyspnea / DOE ( - / - )
Chest pain / Palpitation ( + / - )
Diziness/ Headache ( - / - )
Nausea/ Vomiting ( - / - )
M/40 배 O 성 #3197646
P/Ex
BP 145 / 90 mmHg PR 70 bpm
RR 16 /min BT 36.7 oC
Clear breath sound without rales
RHB without murmur
M/40 배 O 성 #3197646
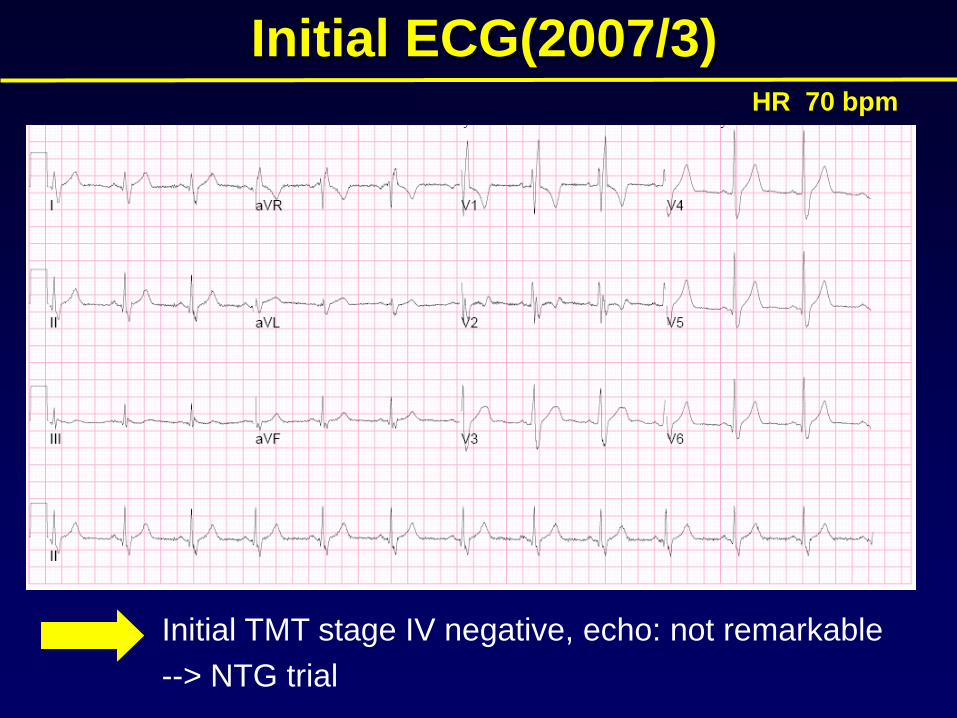
Initial ECG(2007/3)HR 70 bpm
Initial TMT stage IV negative, echo: not remarkable
--> NTG trial
1 month later…..
• 4/30 싸이클 대회에 참여하여 턱쪽으로방사되는 흉 통이 30분간 지속되어 NTG
복용하였으나 증상 완화되지 않고 갑자기 심장이 덜컥하는 느낌이 들면서 의식이 흐려지다 회복됨 OPD로 내원
What would be the diagnostic
evaluation of choice in this patient
• Repeat TMT and echo
• Take the patient directly to cath lab
• Refer the patient for Head up tilt test to rule out
vasovagal syncope
• How about a Coronary CT angiography?
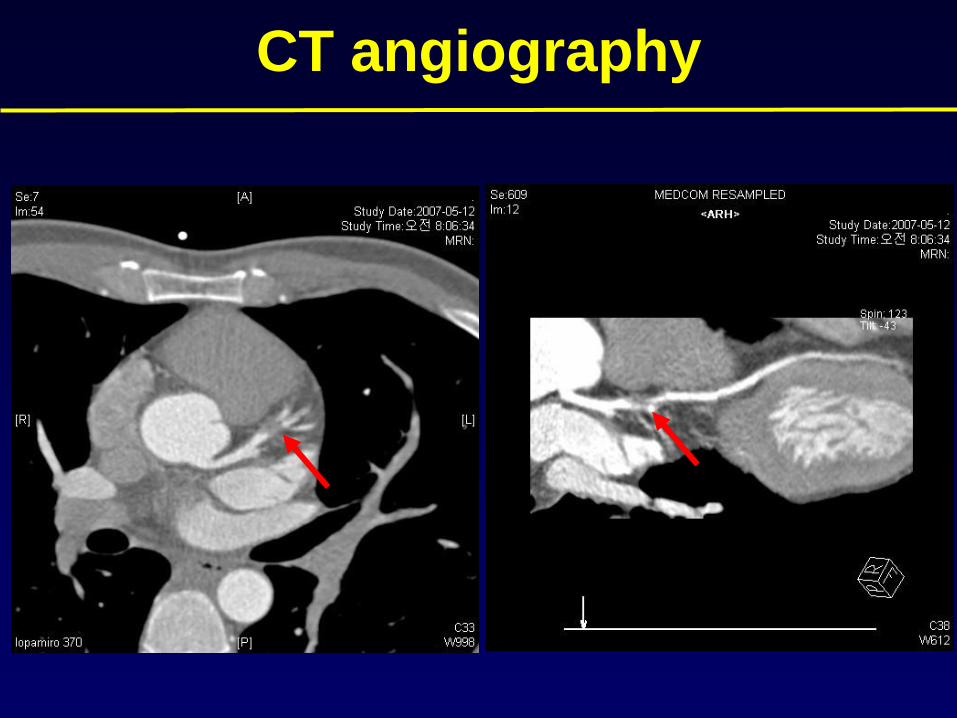
CT angiography
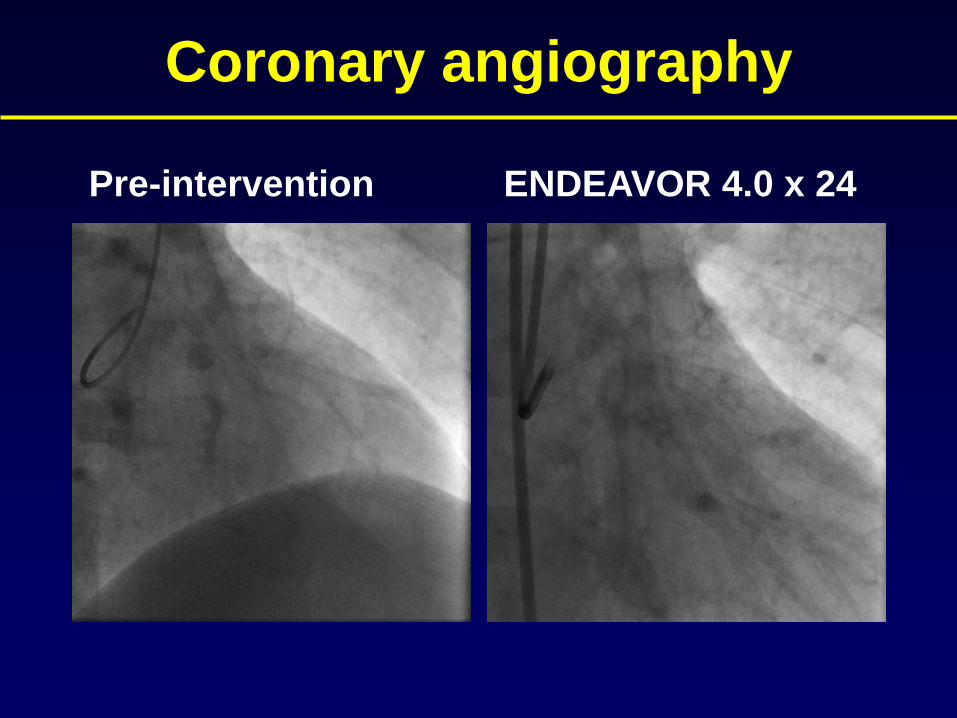
Coronary angiography
Pre-intervention ENDEAVOR 4.0 x 24
Discharge medications
Aspirin 100mg #1
Plavix 75mg #1
Lipitor 10mg #1
Sigmart 10mg #2
Pranol 60mg #3
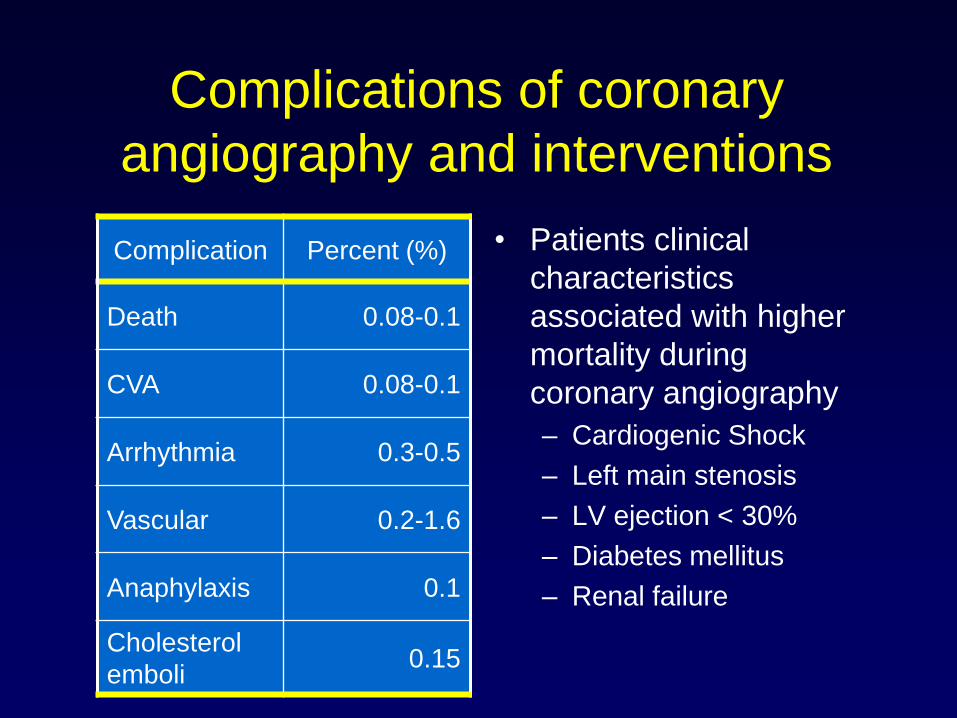
Complications of coronary
angiography and interventions
• Patients clinical
characteristics
associated with higher
mortality during
coronary angiography
– Cardiogenic Shock
– Left main stenosis
– LV ejection < 30%
– Diabetes mellitus
– Renal failure
Complication Percent (%)
Death 0.08-0.1
CVA 0.08-0.1
Arrhythmia 0.3-0.5
Vascular 0.2-1.6
Anaphylaxis 0.1
Cholesterol
emboli0.15
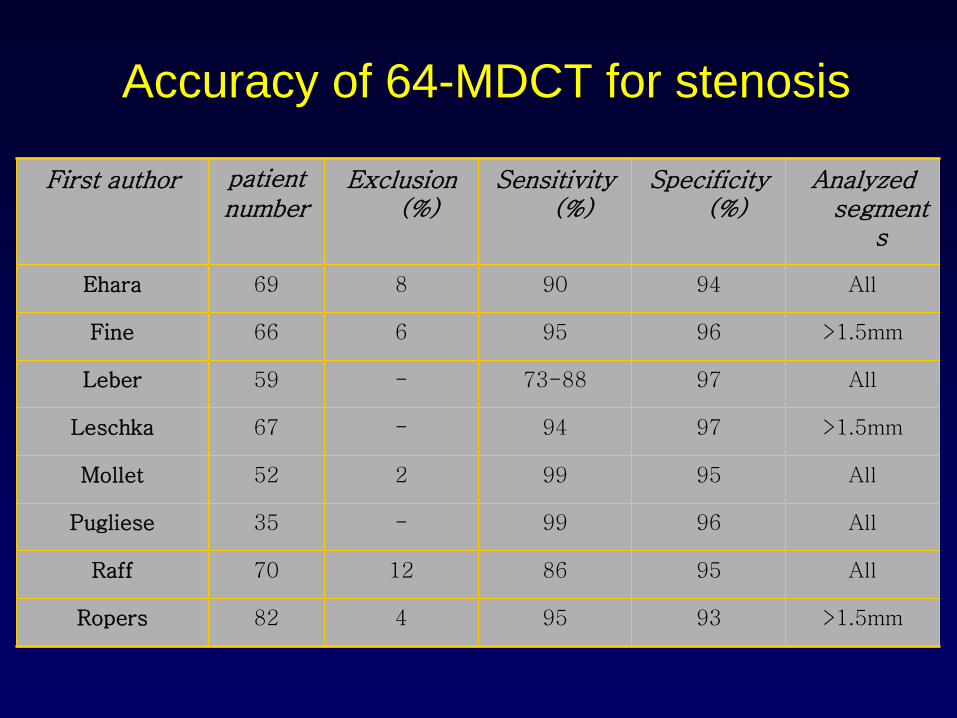
Accuracy of 64-MDCT for stenosis
>1.5mm9395482Ropers
All95861270Raff
All9699-35Pugliese
All9599252Mollet
>1.5mm9794-67Leschka
All9773-88-59Leber
>1.5mm9695666Fine
All9490869Ehara
Analyzed segment
s
Specificity (%)
Sensitivity (%)
Exclusion (%)
patientnumber
First author