park sungha yonsei university college of medicine … · 2015-07-07 · 한국인의 혈압 조절...
TRANSCRIPT
한국인의 혈압 조절 및 혈관 건강 유지를 위해 어떤 약물이 효과적인가?
Park Sungha
Yonsei University College of Medicine
Cardiovascular Center
Division of Cardiology
한국인 고혈압의 특징은 무엇이며 어떤 약물을 사용하는 것이
효과적일까?
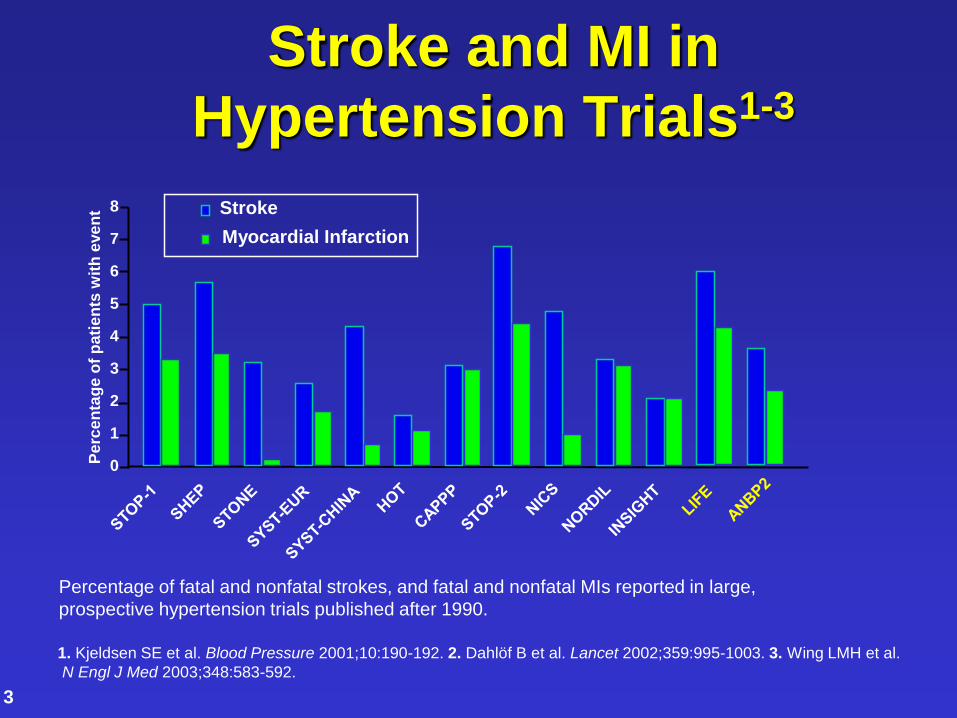
Stroke and MI in
Hypertension Trials1-3
1. Kjeldsen SE et al. Blood Pressure 2001;10:190-192. 2. Dahlöf B et al. Lancet 2002;359:995-1003. 3. Wing LMH et al.
N Engl J Med 2003;348:583-592.
3
0
1
2
3
4
5
6
7
8
Pe
rce
nta
ge o
f p
ati
en
ts w
ith
eve
nt Stroke
Myocardial Infarction
Percentage of fatal and nonfatal strokes, and fatal and nonfatal MIs reported in large,
prospective hypertension trials published after 1990.
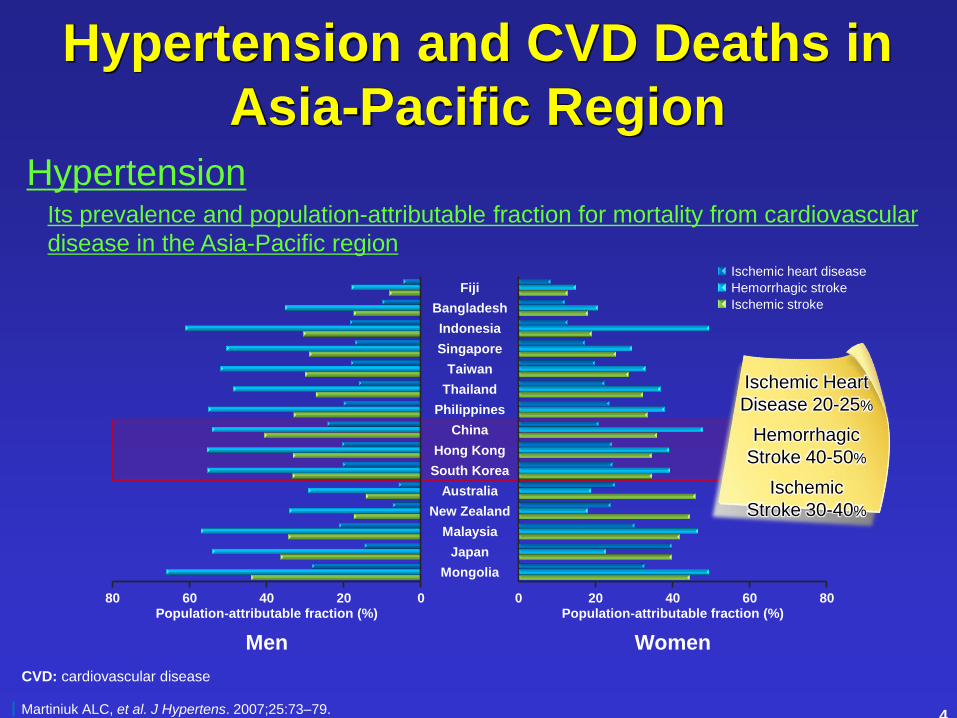
Hypertension and CVD Deaths in
Asia-Pacific Region
Its prevalence and population-attributable fraction for mortality from cardiovascular
disease in the Asia-Pacific region
Hypertension
Ischemic heart disease
Hemorrhagic stroke
Ischemic stroke
0
Fiji
Bangladesh
Indonesia
Singapore
Taiwan
Thailand
Philippines
China
Hong Kong
South Korea
Australia
New Zealand
Malaysia
Japan
Mongolia
20 40 60 Population-attributable fraction (%)
80
Men
0 20 40 60 Population-attributable fraction (%)
80
Women
Martiniuk ALC, et al. J Hypertens. 2007;25:73–79.
CVD: cardiovascular disease
Ischemic Heart
Disease 20-25%
Hemorrhagic
Stroke 40-50%
Ischemic
Stroke 30-40%
4
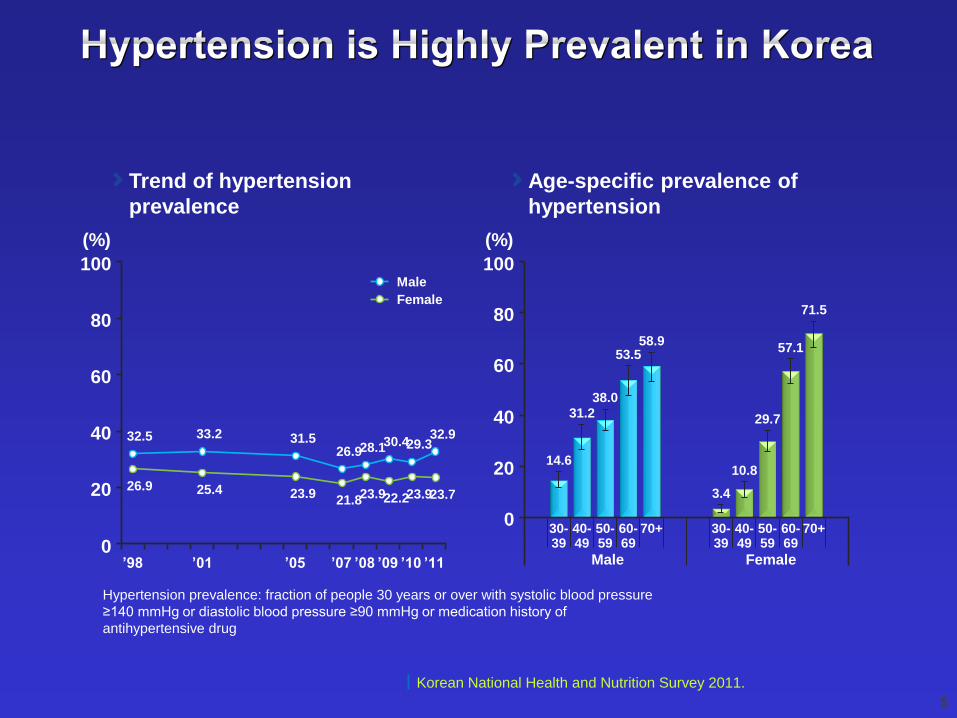
Hypertension prevalence: fraction of people 30 years or over with systolic blood pressure
≥140 mmHg or diastolic blood pressure ≥90 mmHg or medication history of
antihypertensive drug
100
0
80
40
’98
20
60
(%)
’01 ’05 ’07 ’08 ’09 ’10 ’11
32.5
26.9
33.2
25.4
31.5
23.9
26.9
21.8
28.1
23.9
29.3
23.9
32.9
23.7
30.4
22.2
Male
Female
100
0
80
40
20
60
(%)
14.6
Female Male
31.2 38.0
53.5 58.9
3.4
10.8
29.7
57.1
71.5
Korean National Health and Nutrition Survey 2011.
30- 39
40- 49
50- 59
60- 69
70+ 30- 39
40- 49
50- 59
60- 69
70+
Trend of hypertension
prevalence
Age-specific prevalence of
hypertension
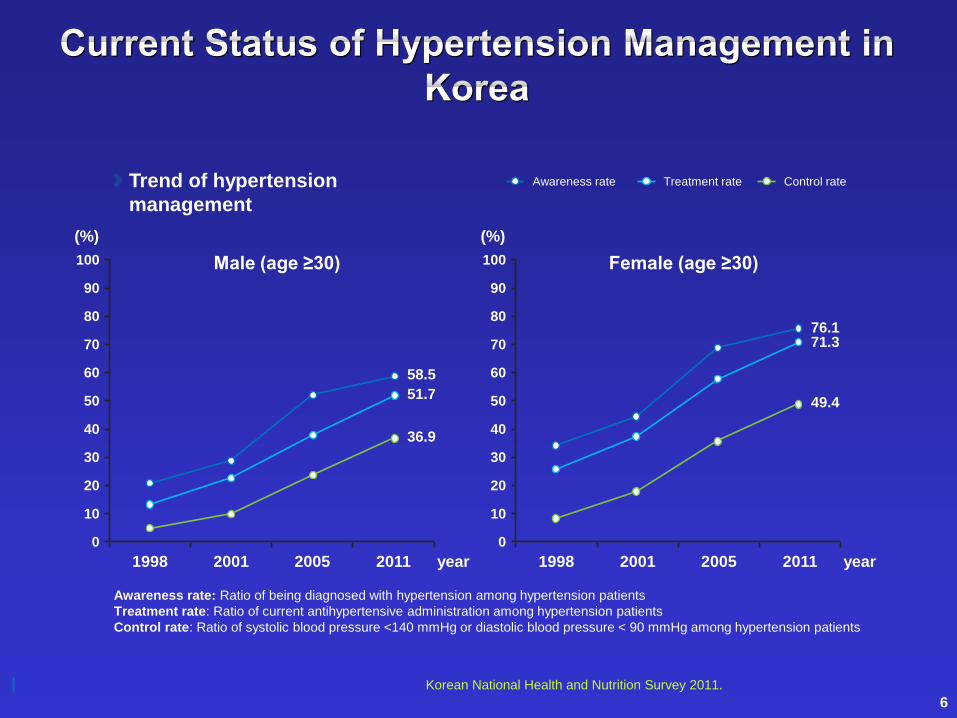
Awareness rate: Ratio of being diagnosed with hypertension among hypertension patients
Treatment rate: Ratio of current antihypertensive administration among hypertension patients
Control rate: Ratio of systolic blood pressure <140 mmHg or diastolic blood pressure < 90 mmHg among hypertension patients
100
0
80
30
1998
10
50
(%)
58.5
Male (age ≥30)
20
40
90
70
60
2001 2005 2011 year
Treatment rate Control rate Awareness rate
51.7
36.9
100
0
80
30
1998
10
50
(%)
Female (age ≥30)
20
40
90
70
60
2001 2005 2011 year
76.1 71.3
49.4
Korean National Health and Nutrition Survey 2011.
Trend of hypertension
management
6
한국인에서 고혈압의 특징
염분섭취가 서양에 비해 높다 이뇨제와 CCB가 효과적일 가능성
뇌졸중이 보다 더 흔한 합병증이고 고혈압의 population attributable fraction은
뇌졸중과 더 강하게 연관되어 있다
CCB가 효과적일 가능성
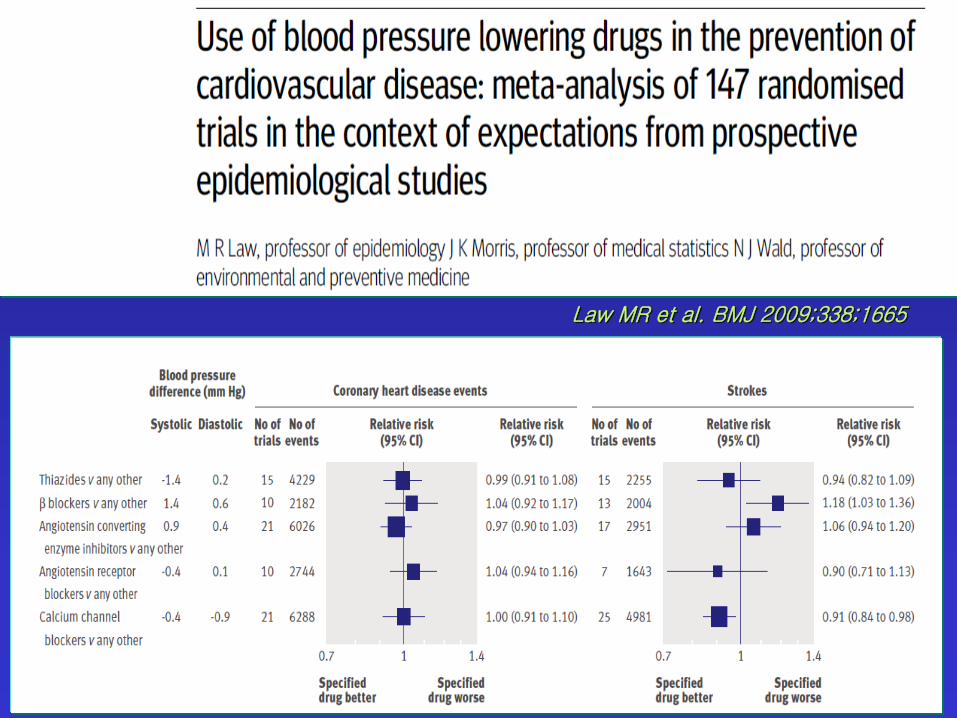
Law MR et al. BMJ 2009;338;1665
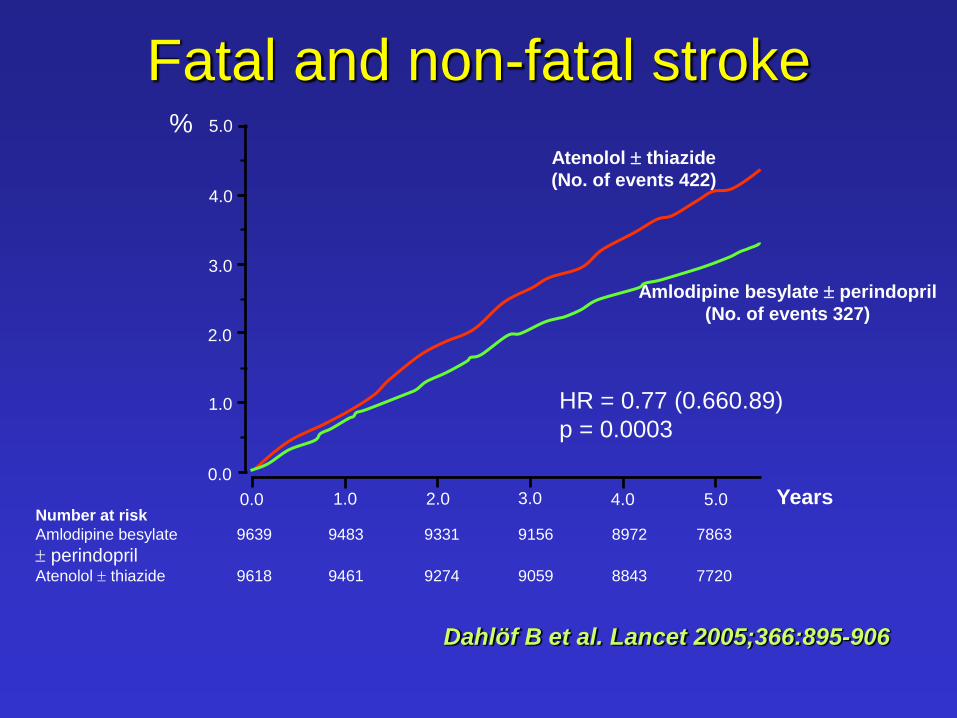
Fatal and non-fatal stroke
Number at risk
Amlodipine besylate 9639 9483 9331 9156 8972 7863
perindopril Atenolol thiazide 9618 9461 9274 9059 8843 7720
0.0 1.0 2.0 3.0 4.0 5.0 Years 0.0
1.0
2.0
3.0
4.0
5.0
Amlodipine besylate perindopril
(No. of events 327)
Atenolol thiazide
(No. of events 422)
HR = 0.77 (0.660.89)
p = 0.0003
%
Dahlö f B et al. Lancet 2005;366:895-906
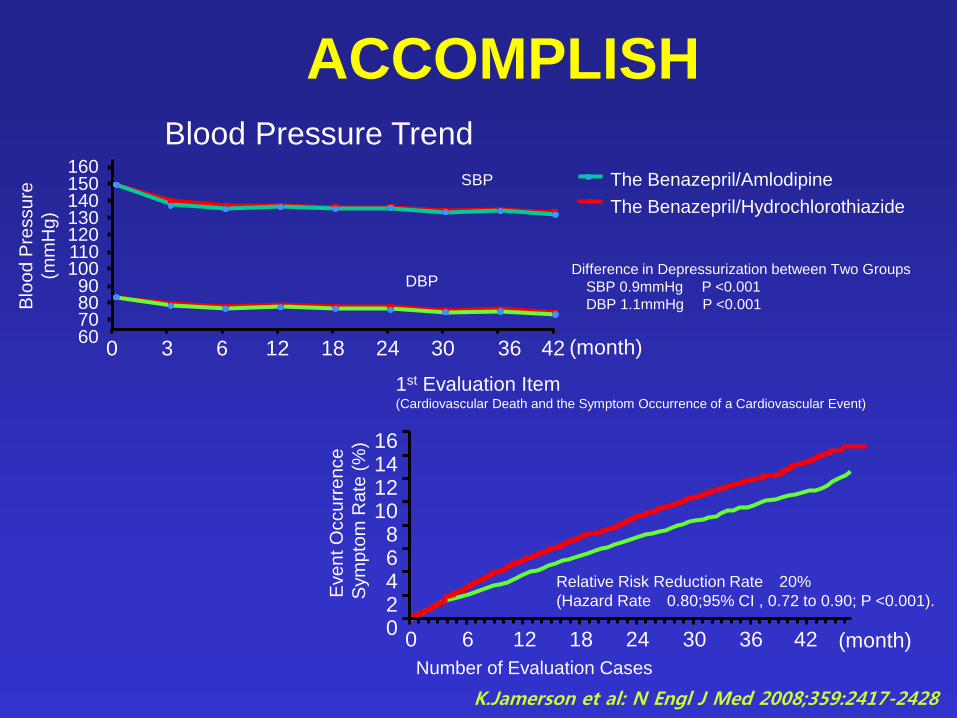
ACCOMPLISH
K.Jamerson et al: N Engl J Med 2008;359:2417-2428
Blood Pressure Trend
1st Evaluation Item (Cardiovascular Death and the Symptom Occurrence of a Cardiovascular Event)
Relative Risk Reduction Rate 20%
(Hazard Rate 0.80;95% CI , 0.72 to 0.90; P <0.001).
16 14 12 10 8 6 4 2 0
0 6 12 18 24 30 36 42 (month)
Eve
nt O
ccu
rre
nce
Sym
pto
m R
ate
(%
)
Number of Evaluation Cases
160 150 140 130 120 110 100 90 80 70 60
0 3 6 12 18 24 30 36 42 (month)
Blo
od
Pre
ssu
re
(mm
Hg
)
The Benazepril/Amlodipine
The Benazepril/Hydrochlorothiazide
SBP
DBP Difference in Depressurization between Two Groups
SBP 0.9mmHg P <0.001
DBP 1.1mmHg P <0.001
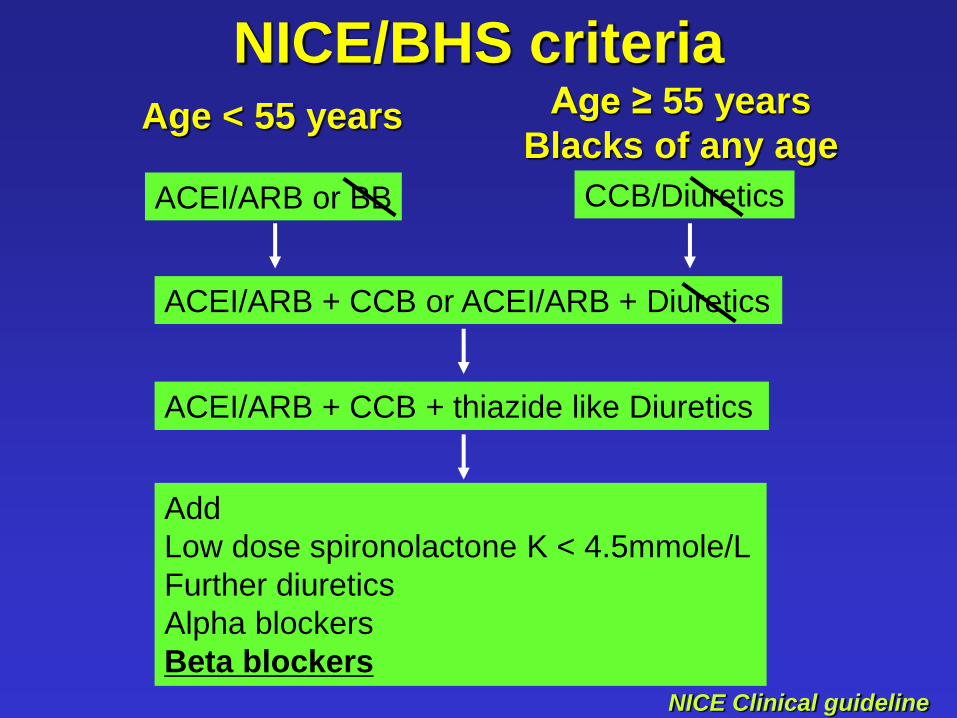
NICE/BHS criteria
ACEI/ARB or BB CCB/Diuretics
ACEI/ARB + CCB or ACEI/ARB + Diuretics
ACEI/ARB + CCB + thiazide like Diuretics
Add
Low dose spironolactone K < 4.5mmole/L
Further diuretics
Alpha blockers
Beta blockers
Age < 55 years Age ≥ 55 years
Blacks of any age
NICE Clinical guideline
그렇다면 혈관 건강 유지에는
어떤 약물이 효과적일까?
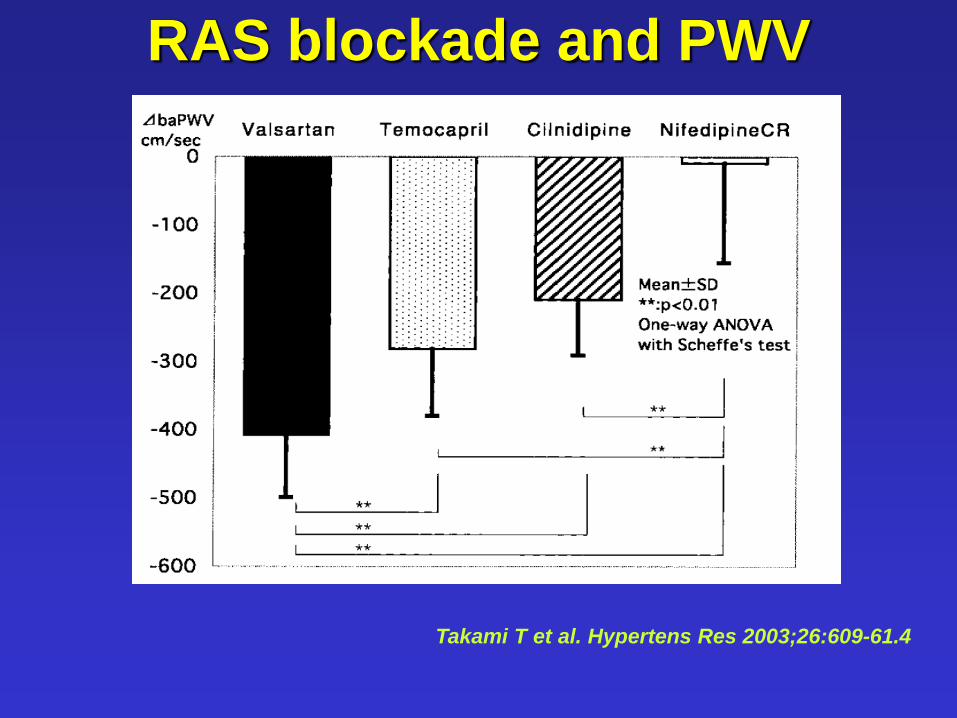
RAS blockade and PWV
Takami T et al. Hypertens Res 2003;26:609-61.4
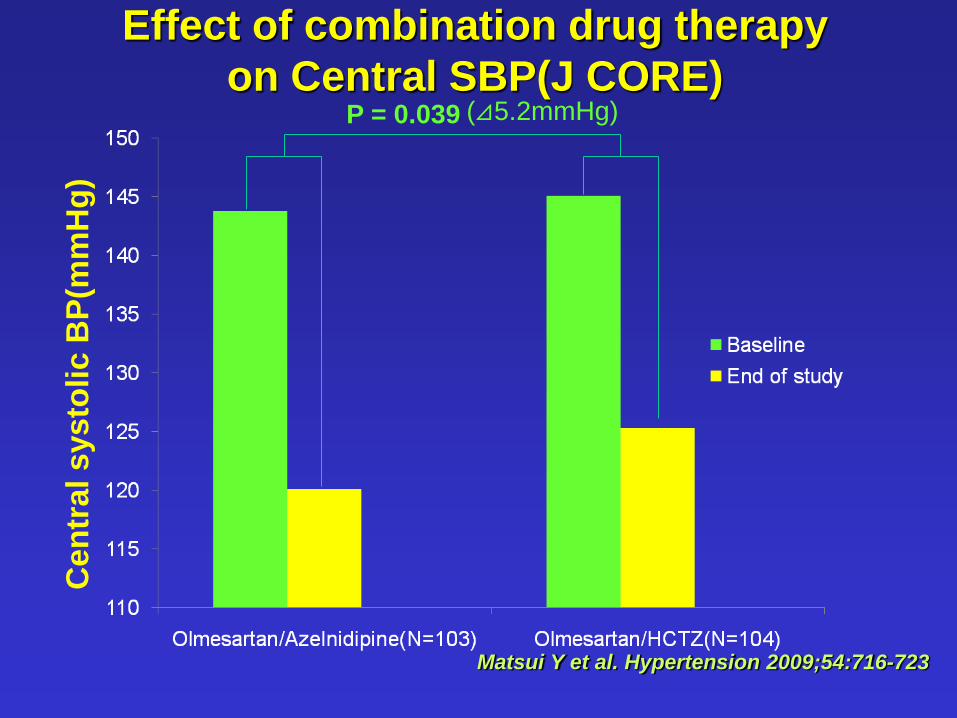
Effect of combination drug therapy
on Central SBP(J CORE) C
en
tral
systo
lic B
P(m
mH
g)
Matsui Y et al. Hypertension 2009;54:716-723
P = 0.039 (⊿5.2mmHg)
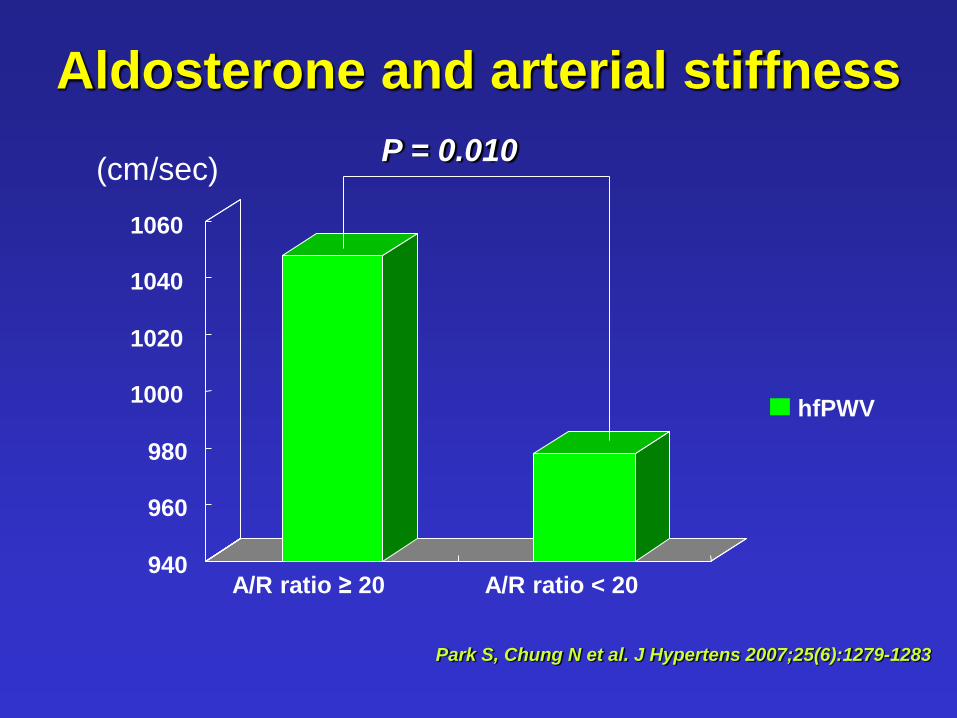
Aldosterone and arterial stiffness
940
960
980
1000
1020
1040
1060
A/R ratio ≥ 20 A/R ratio < 20
hfPWV
(cm/sec) P = 0.010
Park S, Chung N et al. J Hypertens 2007;25(6):1279-1283
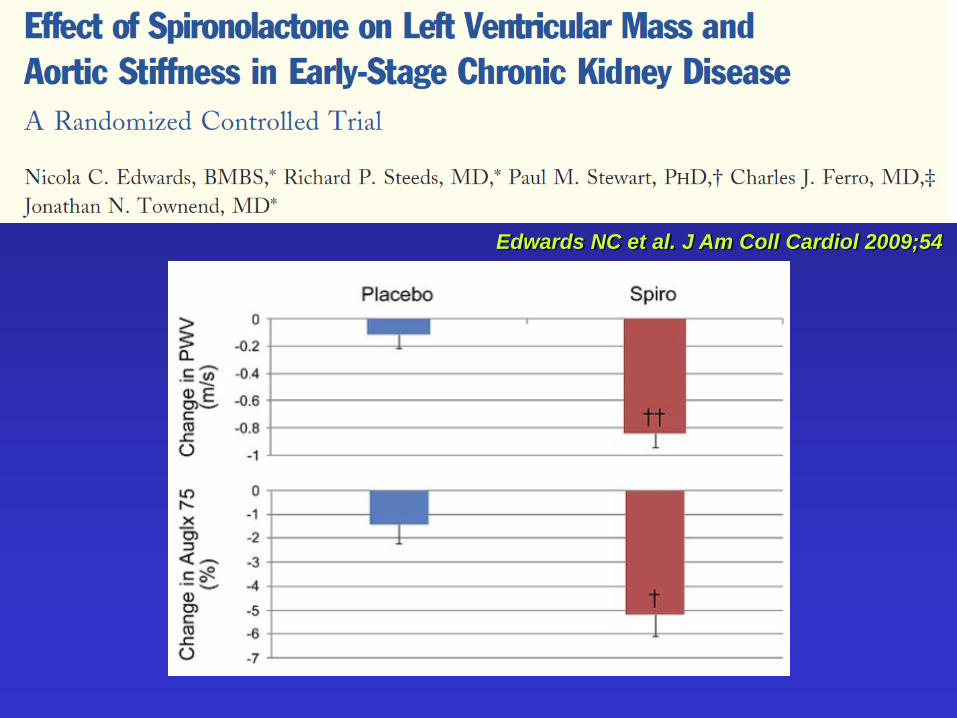
Edwards NC et al. J Am Coll Cardiol 2009;54
Should we discard beta
blockers as first line
agents in treatment of
Hypertension Not so
fast!
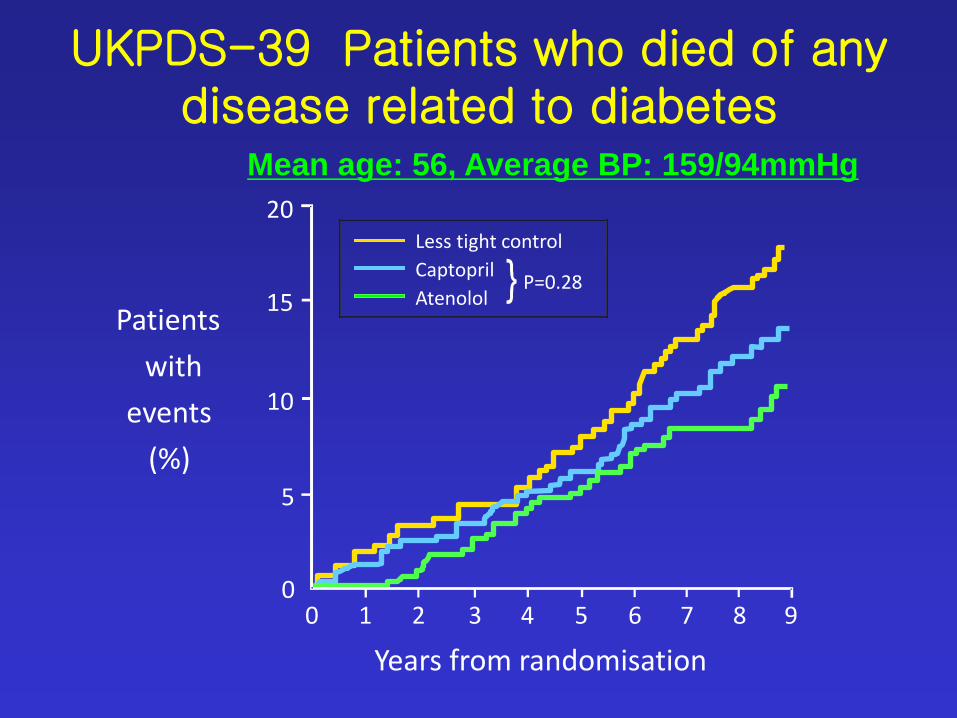
20
15
10
5
0 0 1 2 3 4 5 6 7 8 9
Years from randomisation
Patients
with
events
(%)
Less tight control
Captopril
Atenolol P=0.28
UKPDS-39 Patients who died of any disease related to diabetes
Mean age: 56, Average BP: 159/94mmHg
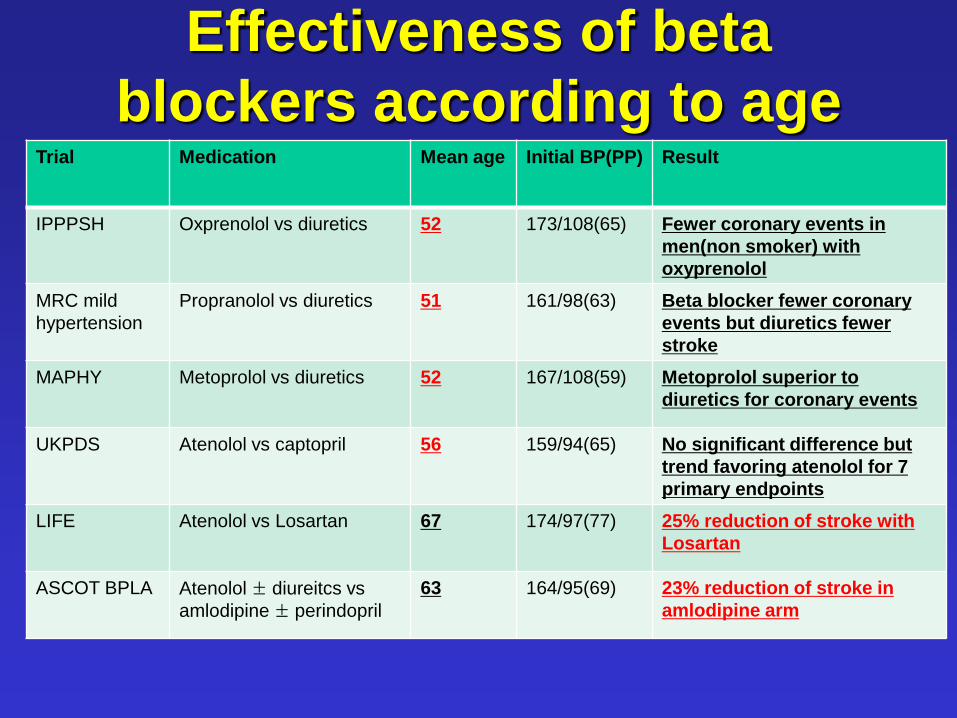
Effectiveness of beta
blockers according to age Trial Medication Mean age Initial BP(PP) Result
IPPPSH Oxprenolol vs diuretics 52 173/108(65) Fewer coronary events in
men(non smoker) with
oxyprenolol
MRC mild
hypertension
Propranolol vs diuretics 51 161/98(63) Beta blocker fewer coronary
events but diuretics fewer
stroke
MAPHY Metoprolol vs diuretics 52 167/108(59) Metoprolol superior to
diuretics for coronary events
UKPDS Atenolol vs captopril 56 159/94(65) No significant difference but
trend favoring atenolol for 7
primary endpoints
LIFE Atenolol vs Losartan 67 174/97(77) 25% reduction of stroke with
Losartan
ASCOT BPLA Atenolol ± diureitcs vs
amlodipine ± perindopril
63 164/95(69) 23% reduction of stroke in
amlodipine arm
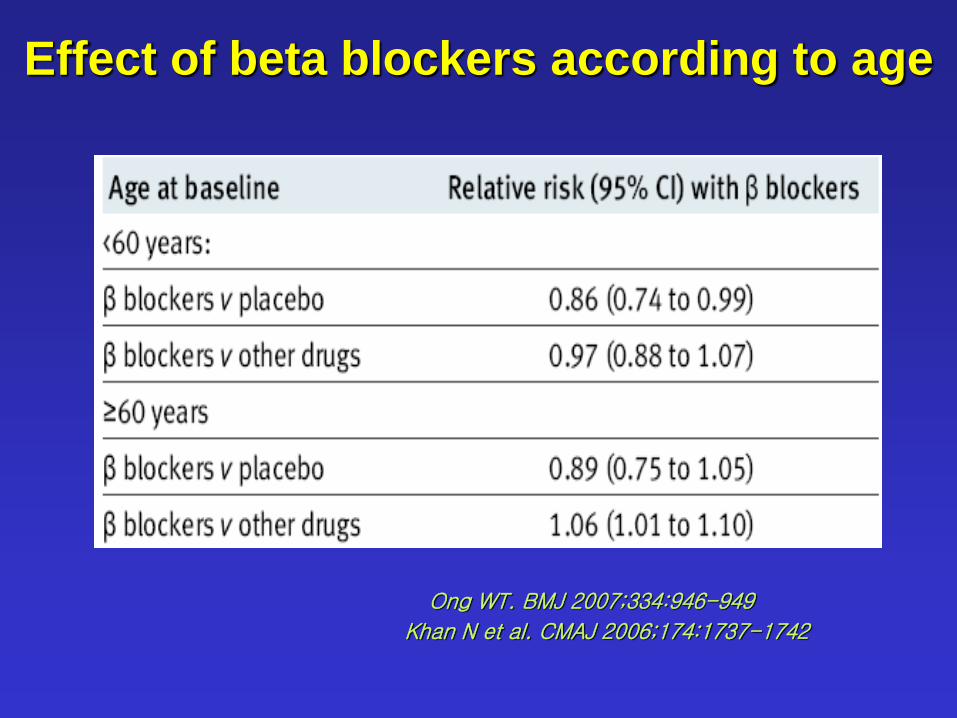
Effect of beta blockers according to age
Khan N et al. CMAJ 2006;174:1737-1742
Ong WT. BMJ 2007;334:946-949
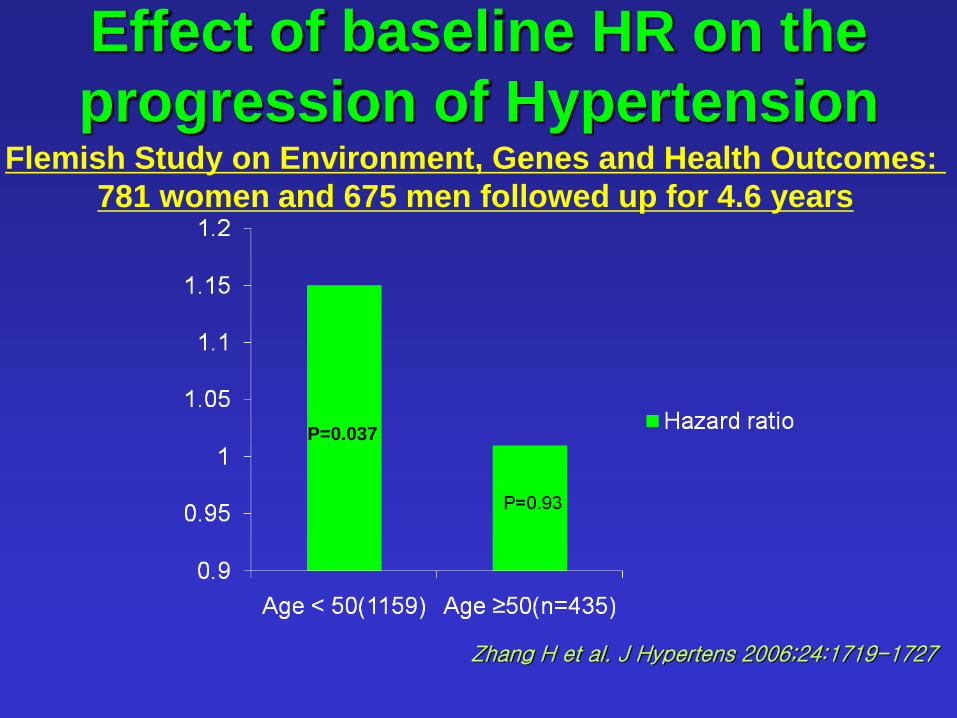
Effect of baseline HR on the
progression of Hypertension Flemish Study on Environment, Genes and Health Outcomes:
781 women and 675 men followed up for 4.6 years
P=0.037
Zhang H et al. J Hypertens 2006;24:1719-1727
160
150
140
130
120
110
100
90
80
70
60
BP
(mmHg)
and
Heart Rate
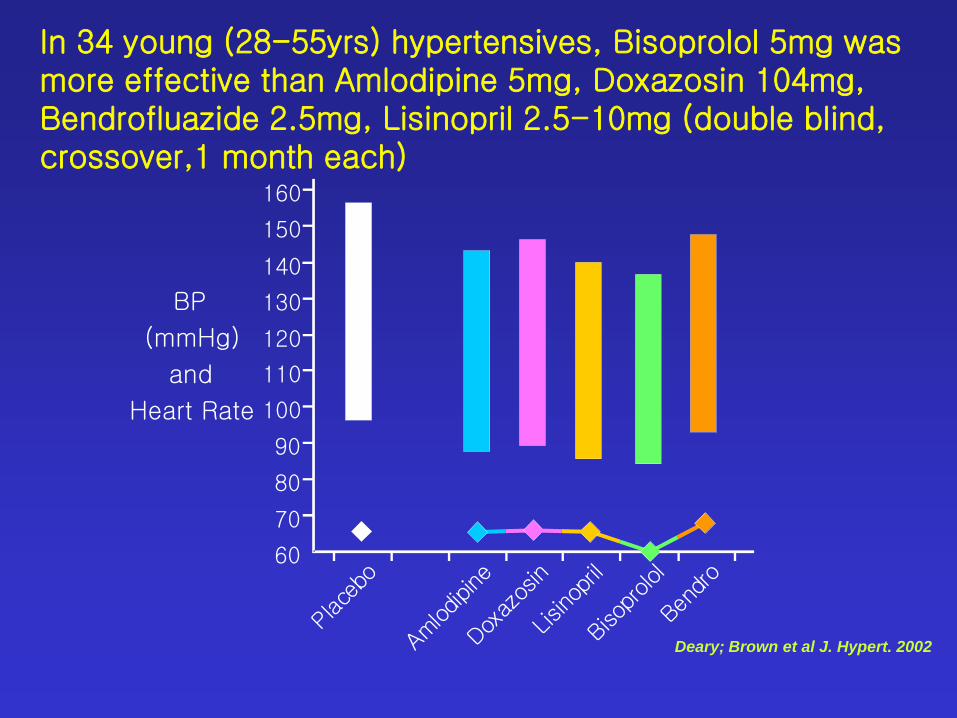
In 34 young (28-55yrs) hypertensives, Bisoprolol 5mg was more effective than Amlodipine 5mg, Doxazosin 104mg, Bendrofluazide 2.5mg, Lisinopril 2.5-10mg (double blind, crossover,1 month each)
Deary; Brown et al J. Hypert. 2002
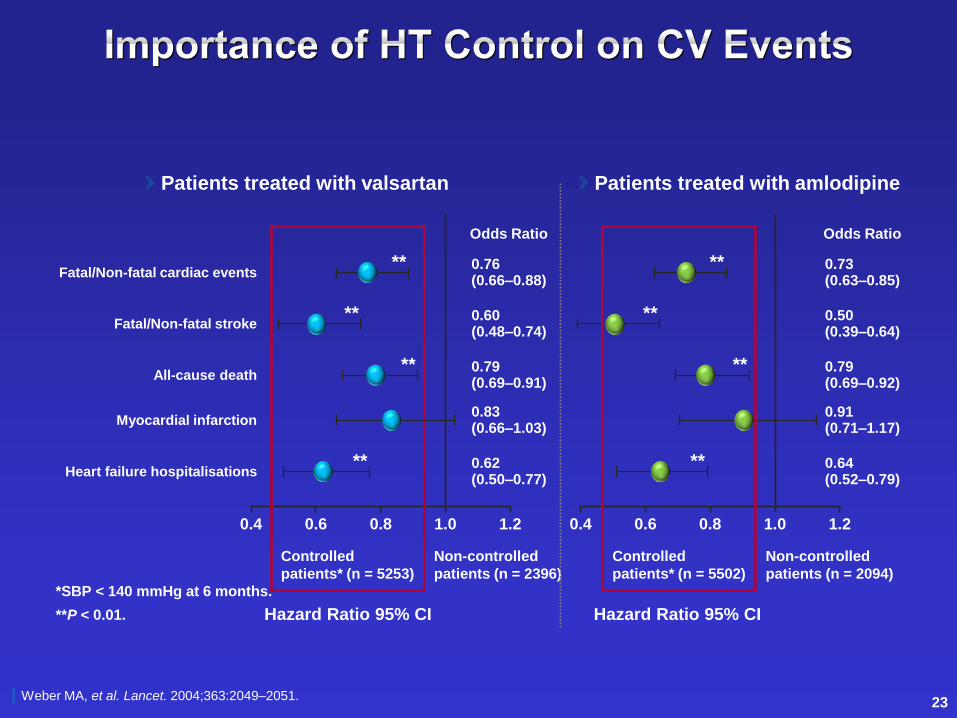
0.4 0.6 0.8 1.0 1.2
Odds Ratio
Controlled
patients* (n = 5253)
Non-controlled
patients (n = 2396)
Hazard Ratio 95% CI
0.4 0.6 0.8 1.0 1.2
Odds Ratio
Fatal/Non-fatal cardiac events ** 0.76
(0.66–0.88) ** 0.73
(0.63–0.85)
Fatal/Non-fatal stroke ** 0.60
(0.48–0.74) ** 0.50
(0.39–0.64)
All-cause death ** 0.79
(0.69–0.91) ** 0.79
(0.69–0.92)
Myocardial infarction 0.83 (0.66–1.03)
0.91 (0.71–1.17)
Heart failure hospitalisations ** 0.62
(0.50–0.77) ** 0.64
(0.52–0.79)
Controlled
patients* (n = 5502)
Non-controlled
patients (n = 2094)
Hazard Ratio 95% CI
Weber MA, et al. Lancet. 2004;363:2049–2051.
*SBP < 140 mmHg at 6 months.
**P < 0.01.
Patients treated with valsartan Patients treated with amlodipine
23
약도 중요하지만 혈압이 얼마나
잘 조절되냐가 가장 중요하다.
70%의 고혈압은 2제 이상을 사용해야 조절이 되면 적절한 조합을 잘 사용하는 것이 중요하다.
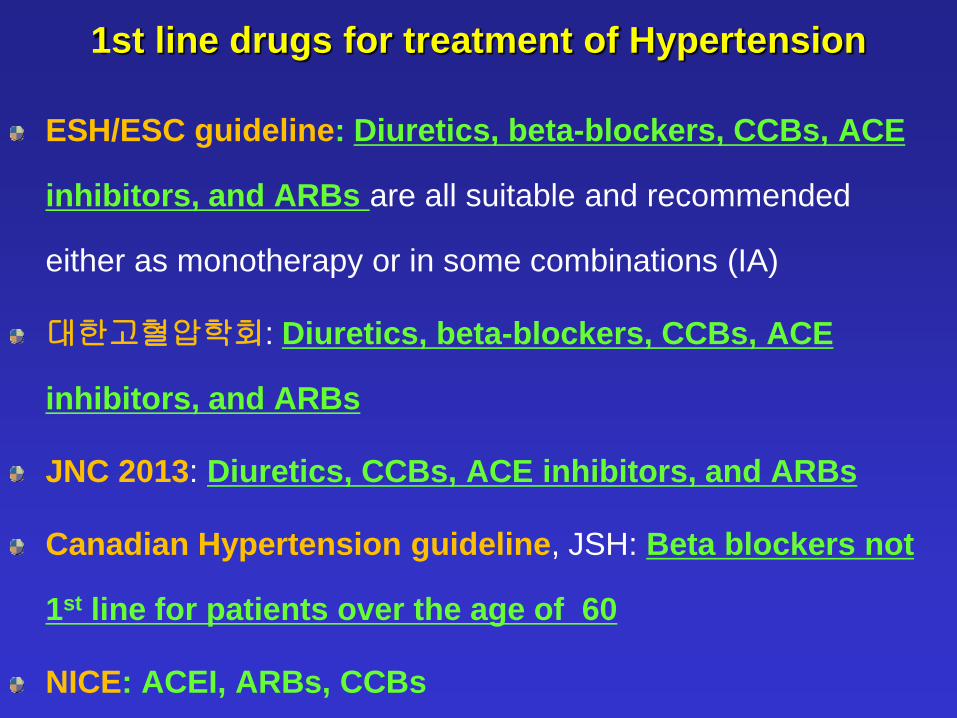
ESH/ESC guideline: Diuretics, beta-blockers, CCBs, ACE
inhibitors, and ARBs are all suitable and recommended
either as monotherapy or in some combinations (IA)
대한고혈압학회: Diuretics, beta-blockers, CCBs, ACE
inhibitors, and ARBs
JNC 2013: Diuretics, CCBs, ACE inhibitors, and ARBs
Canadian Hypertension guideline, JSH: Beta blockers not
1st line for patients over the age of 60
NICE: ACEI, ARBs, CCBs
1st line drugs for treatment of Hypertension
Conclusion
한국인에서 혈압조절 및 혈관건강을 호전시키는데 특별히 효과적인 약물이 있는가? 임상연구를 통한 증거는 없지만 이론적으로
calcium channel blocker, 이뇨제, RAS
inhibitor가 효과적일 가능성이 많다
고혈압의 예후와 가장 밀접하게 연관된 것은
목표혈압 이하로 혈압을 조절하는 것이며 그런 측면에서 봤을 때 젊은 고혈압에서는 beta
blocker도 중요한 1차 약제로 생각된다.