no health without mental health - royal college of … print final.pdf6 no health without mental...
TRANSCRIPT

No HealtH witHout MeNtal HealtHtHe aleRt suMMaRy RepoRtJULY 2009

No HealtH witHout MeNtal HealtH
Copyright © Academy of Medical Royal Colleges 2009
Designed and Typeset byMillbank Media Ltd

No HealtH witHout MeNtal HealtH
1
CONTENTS
NOTES AbOuT ThE REpORT………………...........……………………..................................................................…………...…... .3
ExECuTivE SuMMARy..........………………...........……………………..................................................................…………...…... .5
1. introduction………………………………………………………………….............................................………………….................. 9
2. Recommendations..........................................................................................................................................……………...... 11
3. Awareness...............................................................................................................................................................……….....12
4. Liaison psychiatry Services.................................................................…....................................................................…......20
5. Engaging patients and Carers.................................................................................................................................………...30
6. Re-organisation of Services, Commissioning and Quality Standards..............................................................................34
7. Training and Education..........................................................................................................................................................38
8. Summary.................................................................................................................................................................................41
ACKNOWLEDGEMENTS............................................................................................................................................................42
REFERENCES AND FuRThER READiNG.................................................................................................................................44

2
No HealtH witHout MeNtal HealtH

No HealtH witHout MeNtal HealtH
3
• ThereportrefersprimarilytolegalframeworksandorganisationalstructuresinhealthcareservicesinEngland.However,thestatementoftheimportanceofrecognisingthelinkbetweenphysicalandmentalhealthandthecallforbetterservicesarelikelytoresonateacrossallcountriesoftheUnitedKingdom
• Whererelevant,guidanceprovidedbytheNationalInstituteofHealthandClinicalExcellence(NICE)andtheScottishIntercollegiateGuidelinesNetwork(SIGN)isreferredto.ForafullreportonthementalhealthcontentofNICEandSIGNguidelines,pleaseseewww.rcpsych.ac.uk/nohealth
NOTES AbOuT ThE REpORT

4
No HealtH witHout MeNtal HealtH

No HealtH witHout MeNtal HealtH
5
Thereisaclearlinkbetweenmentalandphysicalhealthandanurgentneedtostrengthenboththeprovisionofmentalhealthcaretopeoplewithphysicalillness andthequalityofphysicalhealthcareprovidedtopeoplewithmentalhealth problemsingeneralhospitalsandprimarycare.Thisreportprovidesaframework withafocusonimprovementwithinthegeneralhospital,whichcanbebrought aboutatrelativelylittleadditionalcostbyfocusingonfivepriorityareas:
Awareness of the link between physical and mental health
Liaison Mental health Services
Engaging patients and Carers
Re-organisation, Quality & Commissioning
Training and Education
ExECuTivE SuMMARy

6
No HealtH witHout MeNtal HealtH
Awareness
…of mental disorders in people with physical illness
Physicalillnesscanhaveprofoundsocialandemotionalconsequences.Asaresult,manypeoplewithphysicalillnesshavementalhealthproblems.Thisassociation istrueforchildrenandyoungpeopleandforolderpeople.Mentalhealthproblemscanimpederecoveryfromaphysicalillnessandincreasemortalityrates.Mentaldisordersoftengounrecognisedinpatientswithphysicalillness.Somepeoplehavephysicalsymptomswhichcannotbefullyexplained.Mentalhealthproblemsincreasethecostofphysicalhealthcare.
…of physical disorders in people with mental illness
Peoplewithmentalillnessaremorelikelytohavereducedlifeexpectancy,oftendue topoorphysicalhealth.Theincreasedmortalityisduetofactorsthatoftenoccurincombination.Theseinclude:socialdeprivation;lifestylefactors;adverseeffectsofmedicationandpooraccesstoservices.
…of physical disorders in people with learning disabilities
Thecausesoflearningdisabilitiescanpredisposethepersontocertainphysicalillnesses.Therearemanybarrierstomeetingthesephysicalhealthneeds.Theseinclude:difficultiesincommunication;diagnosticovershadowing;challengingbehaviour;attitudesamongprofessionalsandpoorlydevelopedlinksbetweenspecialistlearningdisabilityandgeneralhospitalservices.
Liaison Mental health Services
Admissiontohospitalcanbeadistressingexperience.Morethanonequarterofgeneralhospitalpatientshaveamentaldisorder.Mentaldisordermanifestsasa rangeofcommonpresentationsinthegeneralhospitalincluding:self-harm;alcoholproblems;dementia;deliriumanddisturbedbehaviour.Liaisonservicesimprove thecareofpatientswithsuchproblems.

No HealtH witHout MeNtal HealtH
7
Engaging patients and carers
Tobeactivelyinvolvedintheircare,patientsneedbetterinformation.Wellinformedpatientsexperiencelessanxietyandbetteroutcomes.Engagementincludesenquiringaboutmentaldistress.Patientscanbesupportedtoself-managelongtermdisease.Thereremainsastigmaaroundmentalillnessthatneedstobechallenged.Involvingpatientsinservicedevelopment,researchandauditcanimprovementalhealthcareintheacutesetting.Therearemanybarrierstoinvolvingpatientsinimprovingservicesbutthevalueofpatientexpertiseshouldnotbeunderestimated.
Re-organisation, Quality & Commissioning
Generalhospitalsneedflexibleandresponsiveliaisonpsychiatryservices.However,thereislittleincentivefortheNHStodevelopsuchservices.Therearedifferentmodelsofservice,butaliaisonpsychiatryteamrequiresadequatestaffingwitharangeofmulti-disciplinaryskills.Weneedqualitystandardsformentalhealthcare ingeneralhospitals,andthenationalPsychiatricLiaisonAccreditationNetworkwill helpsupporttheirimplementation.
Training and Education
Manyhealthcareprofessionalswouldwelcomebettermentalhealthtraining. Front-linestaffrecognisethisgapintheirknowledge.Doctorsneedbettertraining inthedetectionandtreatmentofmentalhealthproblemsinpatientswhoarephysicallyill.Competenciesneedtobecheckedandtraininginprimarycareneedstobeimproved.Trainingandnationalguidanceshouldensurethatmentalhealthissuesreceiveadequatefocus.

8
No HealtH witHout MeNtal HealtH

No HealtH witHout MeNtal HealtH
9
In2008,theAcademyofMedicalRoyalCollegescommissionedtheRoyalCollegeofPsychiatriststowriteareportsummarisingthelinkbetweenphysicalandmentalhealth.Theaimwastodrawattentiontothementalhealthproblemsthatareassociatedwith,orarisefrom,physicalillnessandthephysicalhealthneedsofpeoplewithmentalillness.
TheRoyalCollegeofPsychiatrists’CentreforQualityImprovementworkedwiththeCollege’sFacultyofLiaisonPsychiatryandotherexpertstocollatetheevidenceandmakerecommendations.ThisispartoftheRoyalCollegeofPsychiatrists’FairDealcampaign:www.fairdeal4mentalhealth.co.uk.
FairDealisathreeyearcampaignfoundedontheviewsofpsychiatrists,serviceusersandcarers.OneofFairDeal'seightobjectivesisafundamentalshiftinunderstandingandpracticeamongallhealthprofessionalsabouttherelationshipbetweenmentalandphysicalhealth.
FairDealpromotesequalrightsandfairnessformentalhealthserviceusers,carers,andthoseworkingwiththem.Itchallengesustoaddressinequality,unfairnessanddiscriminationacrosseightkeyareas:
• Funding• AccesstoServices• In-patientServices• Recovery• DiscriminationandStigma• Engagementwithserviceusers/carers• Availabilityofpsychologicaltherapies• Linkingmentalandphysicalhealth.
Twodocumentshavebeenproduced;this‘ALERTsummaryreport’andamorein-depthreport‘NoHealthwithoutMentalHealth:theevidence’.Thelatterdescribesinmoredetailtheinterfacebetweenphysicalandmentalhealthinabroadrangeofpatientpopulationsanddifferentclinicalservices.Itunderpinsthefirst partoftheALERTreportwhichstatestheimportanceofawarenessofthelinkbetweenphysicalandmentalhealth.Toaccesstheevidencereport,pleasevisitwww.aomrc.ac.ukorwww.rcpsych.ac.uk/nohealth.
1. iNTRODuCTiON

10
No HealtH witHout MeNtal HealtH

No HealtH witHout MeNtal HealtH
11
Awareness
• Allnationalguidelinesaboutmedicalconditions–includingthoseissuedbyNICEandSIGN–shouldincludespecificadviceaboutthedetectionandtreatmentofmentalhealthproblemsassociatedwithmedicalconditions
• ScreeningfordepressioninspecificlongtermconditionsinprimarycareshouldbecontinuedandextendedundertheQualityandOutcomesFramework(QOF)
• Screeningfordepressionandothercommonmentalhealthproblemsshould beroutinelyintroducedintheacutehospitalsetting
• Peoplewithlearningdisabilitiesandpeoplewithseverementalillnessshouldreceiverelevantannualphysicalhealthchecks.
Liaison Mental health Services
• Eachgeneralhospitalshouldhaveanadequatelyfundedliaisonmentalhealthservicetoprovidementalhealthcarethroughouttheentirehospitaltoallwhoneedit,includingthosewithlearningdisabilities
• Liaisonservicesshouldincludespecifiedandappropriateprovisionforolderpeople,aswellaschildrenandyoungpeople
• Patientsingeneralhospitalswithmentalhealthproblemsshouldhavethesamelevelofaccesstoaconsultantpsychiatristastheywouldfromaconsultantspecialisinginphysicalhealthproblems.
Engagement with users and carers
• Informationandeducationshouldbedevelopedandprovidedinappropriatewaysforserviceusers,carersandthepublictodevelopcommunityawarenessofthepsychologicalaspectsofphysicalconditions
• Serviceusersandcarersshouldbeinvolvedindesigningandimprovingmentalhealthservicestogeneralhospitalsandprimarycaresettings,throughaudit,researchandtraining.Fullsupportshouldbeprovided.
Re-organisation, commissioning and quality • Liaisonmentalhealthservicesshouldbecommissionedandreviewedagainst
agreedspecificservicestandards,toensuretheyprovideeffective,evidencebasedinterventionstotreatmentalhealthproblemsinthegeneralhospital
• Allcarepathwaysfordeliveringphysicalhealthcareshouldhaveamentalhealthcomponent.Thereshouldbeacounterpartpathwayforcommissioningpracticetoensuretheservicesareinplacetodeliverthis.
Training
• Allhealthpractitionersshouldhavetraininginmentalhealth• Thecurriculaandassessmentofalldoctorsintrainingandthecontinuing
professionaldevelopmentofqualifieddoctorsshouldreflecttherelationshipbetweenmentalandphysicalhealth,bothingeneralandinspecificconditions
• Nationalguidanceshouldensurethatmentalhealthissuesreceive adequatefocus.
2. RECOMMENDATiONS

12
No HealtH witHout MeNtal HealtH
3.1 Awareness of psychological disorders in people with physical illness
physical illness can have profound social and emotional consequences
Peoplewhohaveseverephysicalillnessoftenlosetheabilitytoperformarange ofactivitieswhichpreviouslymaintainedtheir‘senseofthemselves’ashumanbeings,whetherasaparent,providerorworker.1,2Thisisparticularlytrueforthosewithalongtermcondition.Oneexampleofthisisdiabetes.Althoughpeoplein theearlystagesoftreatedtype1diabetesmayfeelphysicallywell,theyhavetochangetheirnormallifestyle.Thismightincludelimitingtheirdietandhavingtocomplywithademandingtreatmentregime.Somefinditdifficulttoaccepttheserestrictions.Later,ascomplicationsdevelop,peoplewithdiabetesmayexperiencearangeofgradualorsuddendeteriorationsinhealth,includingimpairedvision, poorrenalfunction,andcardiovascularvasculardisease.Thelossofphysicalfunctioncanresultinunemployment,financialhardship,stresswithinthefamily,lossofsexualfunction,lossofsocialactivities,andthreattolife.Physicalillnessthereforecanhaveamajoradverseeffectonaperson’squalityoflife.3,4
Many people with physical illness have mental health problems
Patientswithanyformoflongtermphysicalillnesshaveanincreasedriskofdepression,5,6andthemorethreateningapatientperceivestheirphysicalillness tobe,themorelikelytheyaretobecomedepressed.7Thebiologicalfactorsassociatedwithsomephysicalillnessalsoincreasetheriskofdepression. Thesefactorsincludehormonal,nutritional,electrolyteorendocrine abnormalities,theeffectsofmedicationandthephysicalconsequencesof systemicand/orintracerebraldisease.
The association is also present for children and young people
Aswellashavingahigherincidenceofmentalhealthproblemsthanthegeneralpopulation,childrenandyoungpeoplewithphysicalillnessaremorelikelyto havelearninganddevelopmentandautisticspectrumdisorders.8 Disabled childrenaremoreatriskofexperiencingabuseandthisabusecanleavealegacy ofmentalillhealth.9,10
…and for older people
Thenumberofolderpeoplewithmentalhealthproblemswillincreasebyathirdoverthenext15yearsto4.3million,whichisoneinevery15olderperson.11Inthegeneralhospitalsettingtheprevalenceofmentalhealthproblemsinolderpeople isveryhigh:sixtypercentofpeopleovertheageof65whoareadmittedtoageneralhospitalhaveorwilldevelopamentaldisorderduringtheiradmission, themostcommonbeingthe‘threeDs’—dementia,deliriumanddepression.10 Particularattentionshouldbepaidtoolderpeoplewithaphysicalillnessbecausepoorphysicalhealthincreasestheriskofsuicide.12TheCareServicesImprovementPartnershiphasdevelopedatoolkitprimarilyaimedathealthcarestaffcaringforolderpeoplewithmentalhealthneedsinacutehospitals (www.olderpeoplesmentalhealth.csip.org.uk/lets-respect.html).
3. AWARENESS

No HealtH witHout MeNtal HealtH
13
Mental ill health impedes recovery from physical illness
Mentalhealthproblemscanaffectrecoveryfromeverykindofphysicalillness. Inextremecases,anindividualwithseveredepressionmaysimplygiveupontreatmentbecausetheybelievetheyareaburdenontheirfamilyorthehealthcaresystemandwouldbebetteroffdead.Evenrelativelymildmentalhealthproblems inpatientswithphysicalillnesscanhaveamajoreffectontheirphysicalcondition. Forexample,amildeatingdisorderinapatientwithdiabeteswillhavepotentiallyseriouslongtermconsequences,ofadisproportionatenaturetotheseverityoftheeatingdisorderitself.
Factorswhichpredisposeapersontomentalillness(childhoodadversity,maladaptivebehavioursandmaladaptivepatternsofattachment)increasethelikelihoodofpoorerself-careandincreaseduseofhealthservices.13Mentalhealthproblemscanalsoaffectaperson’sconfidenceinparticipatingincomplexcare orrehabilitationprogrammes.Poormentalhealthalsoaffectsaperson’sability torespondtopaincontrol.14
Forolderpeople,thepresenceofmentalillnessisanindependentpredictorof poorphysicalhealthoutcomes,suchasincreasedmortality,greaterlength ofstay,lossofindependentfunctionandhigherratesofinstitutionalisation.15
Mental disorders often go unrecognised in patients with physical illness
Overhalfofallcasesofdepressioninthegeneralhospitalsettinggounrecognisedbyphysiciansandnursingstaff20andtherearesimilarproblemswithdetectioninprimarycare.21,22,23Thismaybebecausehealthcareprofessionalsdonotthinktoenquireaboutpsychologicalsymptoms,orbecausetheyfeeluncomfortabledoingso.Evenifthesesymptomsarediscussed,practitionersmight,quitereasonably,regarddepressionandanxietyasanunderstandablereactiontobeingphysicallyunwell.Assuch,thepatient’ssymptomsarenormalised24andpractitionersmaynotrealisethatthementalillnesscouldbetreatable.
box 1: Mental disorders can increase mortality rates, for example:
• Theriskofdepressedpatientswithcoronaryheartdiseasedyingin thetwoyearsaftertheinitialassessmentistwiceashighasitisfor non-depressedpatients16
• PeoplewithChronicObstructivePulmonaryDisease(COPD)anddepressionhaveanincreasedrateofmortality17andwhenfacedwithend-of-lifedecisions,theyaremorelikelytooptfor‘donotresuscitate’18
• Depressioninstrokepatientsisassociatedwithincreaseddisability andmortality.19
14
No HealtH witHout MeNtal HealtH
General practitioners (Gps) have a key role in helping people cope
GPsareideallyplacedtofacilitateanaturalpsychologicaladjustmenttophysicalillnessintheirpatients.GPsalsoneedtorecognisewhenpatientswithphysicalillnessarebecomingdepressedandtreatthemaccordingly.Inprimarycare,briefscreeningfordepressionincertainchronicdiseasegroups(diabetesandcoronaryheartdisease)isestablishedundertheQualityandOutcomesFramework(QOF).25 Thechallengeinprimarycareistoextendsuchscreeningtoalllongterm conditionsandtoprovideorrefertoappropriateinterventionsforpeoplewhendepressionisdetected.
Briefmentalhealthassessmentsshouldalsobemaderoutineforpeopleadmittedtoacutehospitalbedstoidentifythosewithmentaldisordersorthoseathighrisk ofdevelopingthem.Careplanscouldthenincludestrategiesforpreventionandpromptmanagementoftheseconditions.
Some people have physical symptoms which cannot be fully explained
Medicallyunexplainedsymptoms(MUS)accountfor20%ofnewpresentationstoprimarycareandforupto30%-40%ofnewlyreferredmedicaloutpatients.26Oftenthepatientsconcernedexperienceahighdegreeofsuffering.Inmostcases,noobviousphysicalreasonisidentified,butasmallproportionofMUSareeventuallyfoundtohaveanunderlyingorganicdisorder.Psychologicalfactorsarecloselyassociatedwithmedicallyunexplainedsymptoms27andresearchsuggeststhat themorebodilycomplaintsreported,thegreatertheirdegreeofpsychologicaldistress.28Also,themorecomplaintsreported,thegreaterthedegreeofimpairmentandthemorefrequentuseofhealthcareservices.29Over40%ofoutpatientswithMUShaveananxietyordepressivedisorder.30
Mental health problems increase the cost of physical healthcare
Patientswithdepressivedisorderaretwiceaslikelytouseemergencydepartmentservicesasthosewithoutdepression.31Indiabetes,totalhealthexpenditureisfourandahalftimeshigherforindividualswithdepressionthanforthosewithoutdepression.32Inchronicheartdisease,depressedpatientshavehigherratesofcomplicationsandaremorelikelytoundergoinvasiveprocedures.33,34Peoplewithchronicobstructivepulmonarydisease(COPD)whoarealsodepressedhavelongerhospitalstaysandincreasedsymptomburden.35Thepresenceofdementiaanddeliriumincreasesthelengthofstayofolderpeopleingeneralhospitalsby uptotendays.36
box 2: Long term conditions are associated with a high emotional burden.32,40,50
For example in diabetes, depression is linked to:
• Poorselfmanagement• Poorqualityoflife• Poorcontrolofbloodglucoselevels• Morediabeticcomplications• Increasedriskofdying• Delayoravoidanceofdiabetestreatment• Increasedcosts.
No HealtH witHout MeNtal HealtH
15
3.2 Awareness of physical disorders in people with mental illness
people with mental illness have reduced life expectancy
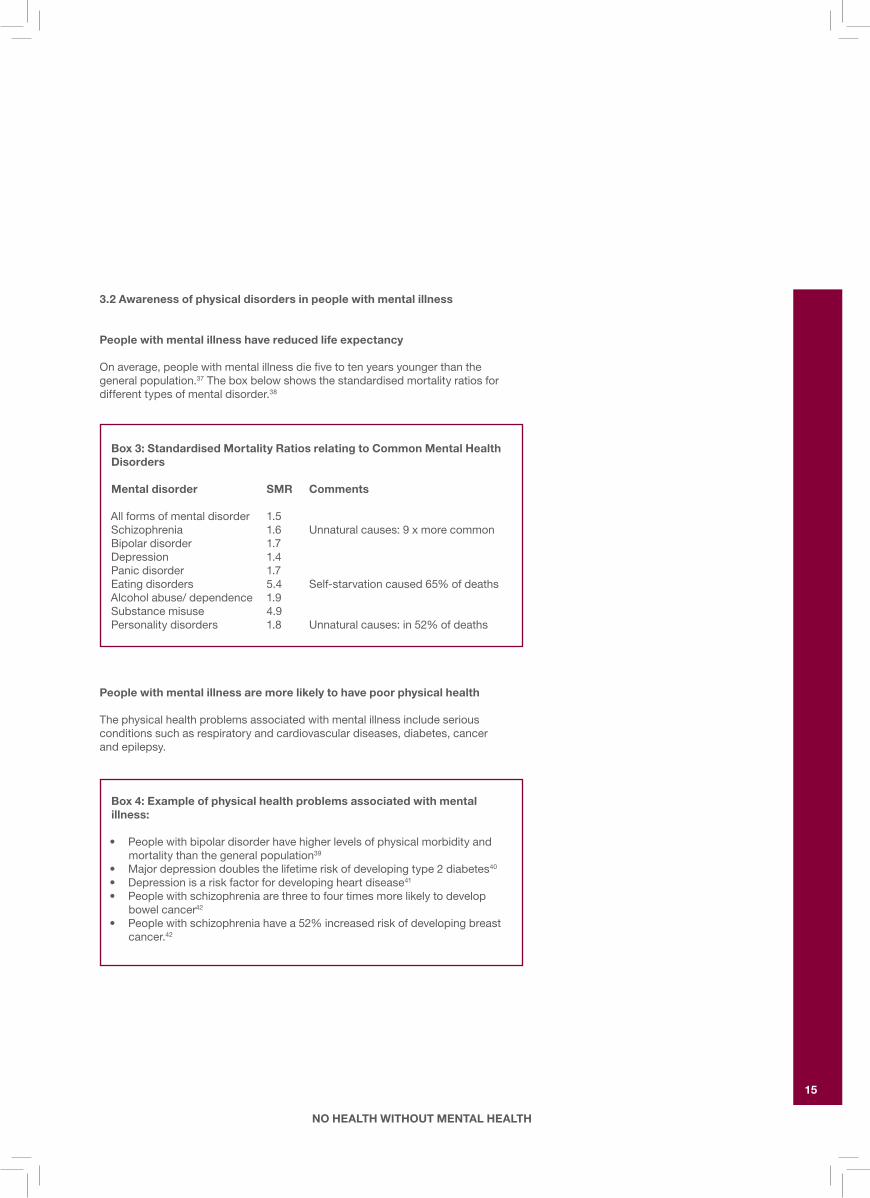
Onaverage,peoplewithmentalillnessdiefivetotenyearsyoungerthanthe generalpopulation.37Theboxbelowshowsthestandardisedmortalityratiosfordifferenttypesofmentaldisorder.38
people with mental illness are more likely to have poor physical health
Thephysicalhealthproblemsassociatedwithmentalillnessincludeseriousconditionssuchasrespiratoryandcardiovasculardiseases,diabetes,cancer andepilepsy.
box 3: Standardised Mortality Ratios relating to Common Mental health Disorders
Mental disorder SMR Comments
Allformsofmentaldisorder 1.5Schizophrenia 1.6 Unnaturalcauses:9xmorecommonBipolardisorder 1.7Depression 1.4Panicdisorder 1.7Eatingdisorders 5.4 Self-starvationcaused65%ofdeathsAlcoholabuse/dependence 1.9Substancemisuse 4.9Personalitydisorders 1.8 Unnaturalcauses:in52%ofdeaths
box 4: Example of physical health problems associated with mental illness:
• Peoplewithbipolardisorderhavehigherlevelsofphysicalmorbidityandmortalitythanthegeneralpopulation39
• Majordepressiondoublesthelifetimeriskofdevelopingtype2diabetes40
• Depressionisariskfactorfordevelopingheartdisease41 • Peoplewithschizophreniaarethreetofourtimesmorelikelytodevelop
bowelcancer42
• Peoplewithschizophreniahavea52%increasedriskofdevelopingbreastcancer.42

16
No HealtH witHout MeNtal HealtH
The increased morbidity is due to factors that often occur in combination…
Social deprivation
Peoplewithmentaldisordersaremorelikelytoliveinpoverty,beunemployed,havepoorhousing,tobehomelessortoliveinaninstitutionsuchasnursinghome,penalestablishment,orsecurepsychiatricfacilities.43,44,45Theyaremorelikelytodependonstatebenefitsforincome,andsocialisolationcompoundstheirdifficulties.45
Lifestyle factors
Comparedwiththegeneralpopulation,peoplewithamentalillnessaremorethantwiceaslikelytosmoketobacco,46eatlessfruit,arelesslikelytoexerciseregularly,47 havehigherratesofobesity(70%)andmoreoftendevelopthemetabolicsyndrome.48Somealsoarguethatpeoplewithmentalhealthproblemsaremorelikelytobecomephysicallydisabledasaresultofaccidentsorattemptedsuicide.49
Adverse effects of medication
Inparticular,thelongtermuseofantipsychoticdrugsincreasestheriskofdevelopingmetabolicsyndromewhichischaracterisedbyweightgain,highbloodlipidlevels,highbloodpressureandglucoseintolerancewhichcanleadtodiabetes.50Theriskofsuddendeathinschizophreniaincreasesincrementally witheachadditionalpsychotropicmedicationtaken.51
poor access to services
Peoplewithmentalhealthproblems,comparedtothosewithout,receivepoorerqualityhealthcare.37Theyarelesslikelytoseekmedicalhelpanddonotreceive thesamestandardofphysicalhealthcareineitherprimaryorsecondaryhealthservicesasthegeneralpopulation.TheymaynotregisterwithaGPordentist (ormaylosetheirregistration),andcanexperiencedifficultymakingandkeepingappointments.Peoplewithseverementalhealthproblemsarelesslikelytotake partinhealthscreeningsuchasmammographyandcervicalcytology.37Thepresenceofamentaldisordermay‘overshadow’therecognitionandtreatment ofphysicalhealthproblems.Thisovershadowingcanresultinareductioninthequalityofphysicalhealthcareprovidedbyhealthprofessionals.
box 5: patient viewpoint on taking medication for both physical and mental health problems:
‘Itakepsychotropicmedicationformentalhealthaswellasmedicationforphysicalhealth.Thiscanbeproblematicbecauseofthecontraindications– inmyexperience,neithergroupofspecialistscaredabout(orexplainedto me)theeffectsthesemedicationscanhaveoneachother.Ihadtoborrow aBNF[BritishNationalFormulary]andlookitupmyself.’
(Serviceuser,London,2008)

No HealtH witHout MeNtal HealtH
17
3.3 Awareness of physical disorders in people with learning disabilities
Ausefulmatrixofgeneticdisordersandthepotentialphysicalandpsychologicaldisorderslinkedtoeachdisorderisavailableonwww.rcpsych.ac.uk/nohealth
There are many barriers to meeting the health needs of people with learning disabilities
TheDisabilityRightsCommissioninvestigationofequaltreatment37confirmed majordeficitsinthephysicalhealthcareofpeoplewithalearningdisabilityandtheMencapreport ‘Death by Indifference’60highlightedthetragicissueofunnecessaryandavoidabledeathsresultingfromunacceptablecare.
Healthchecksforpeoplewithlearningdisabilityinvolvingsystematicquestioningandstructuredphysicalexaminationhavebeenshowntodiscoverhighlevelsofunmetneed135,136andthatthebenefitsofsuchinterventionsaresustained.137 Therecentintroductionofprimaryhealthcarechecksforpeoplewithalearningdisability,asadirectlyenhancedservice(DES)intheUnitedKingdomis,therefore, awelcomedevelopment.Specialistlearningdisabilityservicescanplayanimportantroleinfacilitatingthisprocess,includingtheprovisionofrelevanteducation,guidanceand,wherenecessary,practicalsupport.
box 6: Many of the causes of learning disabilities can predispose a person to physical health problems
Learningdisabilitiesarisefromarangeofgeneticconditionsaswellasadverseeventsinthepre-natal,peri-natalandpost-natalperiodsandcanpredispose thepersontoarangeofconcurrentphysicalhealthproblems.Forexample:
• PeoplewithDown’sSyndromehavehighratesofcongenitalheartdisease,thyroiddisorder,sensoryimpairmentsanddementia.52,53Asaresult,theyhave alifeexpectancywhichisshorterthanthatofthegeneralpopulation52
• ThefoodseekingbehaviourofpeoplewithPrader-WilliSyndromemeans thattheyareatagreaterriskofobesityandtype2Diabetes54
• Peoplewithcerebralpalsyexperiencearangeofmusculoskeletal deformitiesandhighratesofdysphagiaandassociatedrespiratoryproblems55
• Therateofepilepsyis20%inthelearningdisabilitypopulation,risingto 50%inthosewithmoreprofoundlearningdisabilities59
• Peoplewithlearningdisabilitieshavelowerbonedensitythantheaveragepopulation56
• Respiratorydiseaseisthemostcommoncauseofdeath(46%-52%)forpeoplewithlearningdisabilities57
• Unmetphysicaldisorderscancontributetochallengingbehaviours, especiallyinindividualswithmoreseverelearningdisabilities58
• Peoplewithlearningdisabilitiesaremorelikelythanthegeneralpopulation toexperiencementalhealthproblemsandtheassociatedrisks.59

18
No HealtH witHout MeNtal HealtH
Several factors can contribute to unequal access to healthcare, including:
Difficulties in communication
ThedeliveryofhealthcareintheUKlargelydependsonthepatientseekinghelp.Peoplewithlittleornomeansofverbalcommunicationoftencannotdothis.Eventhosewithmoremildorhiddenlearningdisabilitiesmaystruggletonegotiateasystemwhichassumescompetenceinareassuchasliteracy.Informationisrarelypresentedinaformthatistailoredtoindividualneeds,andindividualsmaybeunabletoprovideinformationintheformthathealthcareprofessionalsrequire.
Somepeoplewithlearningdisabilitiesmayalsohavesensoryimpairmentssuch asdeafness,andshouldnotbedeniedaccesstogoodqualitymentalhealth caresimplybecausethehealthserviceisillequippedtocommunicatewith them.Whenseekingorreceivinghealthcareinanysetting,deafpeoplehavetherighttobeassessedbyatrainedworkerwhohasdeaf/deafblindawareness andskillsinworkingwithpeoplewiththewholerangeofhearingrelated communicationneeds.61
Side effects of medication
Peoplewithlearningdisabilitiesareparticularlysusceptibletothephysicalandpsychologicalsideeffectsofmedication.Thiscanbefurthercompoundedbyatendencytoacquiesceandareducedcapacitytorecogniseandcommunicateproblemsrelatedtosideeffects.
Diagnostic overshadowing
Cliniciansmaydismissbehavioursthataremanifestationsofpainordeliriumasbeingintrinsictotheperson’slearningdisability.Similarly,hearingorvisionproblemsmaygoundetectedbecausehealthcareprofessionalswronglyattributelowlevelsoffunctioningtothelearningdisabilityitself.62
Carersmaybeunawareofthesignificanceofhealthdeficitsormayviewthem asanintrinsicaspectoftheindividual’scondition.Theymayalsoassumethat thehealthproblemisnotamenabletotreatment.
Challenging behaviour
Thismayresultfromthefactthatmanypeoplewithlearningdisabilitiesfindclinicalenvironmentsfrighteningandthreatening.Itisimportanttolookbeyondthepresentingproblemtoidentifypotentialphysical,psychologicalandenvironmentalcauses.Thesedifficultiescanthenbeminimisedthroughcarefulplanning andpreparation.63,64
Attitudes among professionals
Professionalswhoareunfamiliarwiththeneedsofpeoplewithlearningdisabilitiescanbeundulypessimistic,withinappropriatedecisionsbeingmadebaseduponill-foundedopinionsabouttheirqualityoflifeandvaluesascitizens.65

No HealtH witHout MeNtal HealtH
19
poorly developed links
Peoplewithlearningdisabilityhaveequalrightstoaccessgenerichealthcareservices.Thismayrequireadditionalinputfromspecialistlearningdisabilityservicestofacilitatethisprocess.However,thelinksbetweenthesespecialistservicesandgeneralhospitalservicesareoftenpoorlydeveloped.Somerecentlydevelopednetworksintheformofliaisonlearningdisabilityserviceshaveshownpromisingresults.66
The importance of making reasonable adjustments
Itisimportanttoallowthetimerequiredtospeaktotheindividual.Aneffectiveconsultationdependsonanumberoffactorsincluding:
• Providingaccessibleinformationinastylethatsuitstheindividual (thismayincludetheuseofcommunicationaids)
• Checkingforunderstanding• Offeringappropriatesupport• Seekingbackgroundinformationfromsomeonewhoknowsthepatientwell• Assessingthepersoninanoptimumenvironment• Preparingtheindividualforanyassociatedphysicalexamination• Establishinganeffectivetherapeuticalliance.
For further advice, please see the ‘Top Ten Tips on Effective Consultation’, at http://www.intellectualdisability.info/values/top_ten_tips.htm. This checklist has been written primarily for GPs but can be usefully applied to a general hospital setting.67

20
No HealtH witHout MeNtal HealtH
Thissectionwillexploretherolethatliaisonpsychiatrycanplayinbridgingthegapbetweenphysicalandmentalhealthinthegeneralhospital.
Admission to hospital can be a distressing experience
Inadditiontothedistressarisingdirectlyfromtheirphysicalillness,peopleadmittedtohospitalenteranunfamiliar,stressfulenvironment.Manyolderpeople,whoareorientatedintheirownhomemaybecomeconfusedwhenplacedinanewandstrangeenvironment.Thisiscompoundedifpatientsaremovedfromoneclinicalareatoanother.Patientsoftensharetoiletandbedroomfacilitieswithstrangers,giveuptheirnormalclothesandpersonalbelongings,anddressinnightclothes.Theyhavetointeractwithmanydifferentnurses,doctorsandotherhealthprofessionals.Atthesametimetheiraccesstorelativesandlovedonesisrestricted.Thosewhosmokeheavilyordrinkalcoholmightfindtherestrictionsimposedbyhospitaladmissionparticularlydifficult.
hospital clinicians may find it difficult to deal with fear, worry and other strong emotions in a hospital setting
Nursesanddoctorsinhospitalsareoftenwhollyoccupiedbythephysicalillnessandmightnothavetimetoenquireaboutemotionaldistress.Theymightalsofeeluncertainabouthowtomanagedistressifpatientsbecomeupset.68Notallhospitalwardshaveinterviewroomswherepatientsandtheirfamiliescanbeseeninprivateandpersonalconversationsoftentakeplacebehindacurtaindrawnaroundthepatient’sbed.
There are many different kinds of mental health problems in the general hospital setting
Self-harm
Self-harmisoneofthemostcommonreasonsforadmissiontoanacutemedicalbedandaquarterofpeoplewhoself-harmandattendemergencydepartmentsreportexperiencingnegativeattitudesfromstaff.71NICErecommendsthatpeoplewhoself-harmshouldreceivethesamestandardofcareasotherpatientsandthat adetailedpsychosocialriskassessmentbeundertaken.72Thisisimportantbecausepeoplewholeavetheemergencydepartmentorhospitalwithoutanadequatepsychosocialassessmentarelesslikelytobeofferedfollowup73andmaybemorelikelytorepeatself-harm.74Despitethis,notallpatientsarecurrentlyoffereda
4. LiAiSON pSyChiATRy SERviCES
box 7: More than one-quarter of general hospital patients have a mental disorder
• Twenty-eightpercentofconsecutivepatientsadmittedtoanacutemedicalsettingwerefoundtohaveapsychiatricdisorderthatmetdiagnosticcriteriaandafurther41%hadsub-clinicalsymptomsofpsychologicaldistress.69
• Depressiveandanxietydisordersaretwiceascommoninhospitalpatients astheyareinthegeneralpopulation70
• Thefiguresareevenhigherforolderpeople,whooccupytwo-thirdsofNHSbeds.Sixtypercentofpeopleovertheageof65whoareadmittedtoageneralhospitalhaveorwilldevelopamentaldisorderduringtheiradmission.Upto40%havedementia,53%depressionand60%havedelirium.15

No HealtH witHout MeNtal HealtH
21
psychosocialassessmentandevenwhentheyare,somepatientsreportdissatisfactionwiththis.71Manygeneralhospitalprofessionalsreportalackoftraining,supportandsupervisionregardingworkingwithpeoplewhoself-harm.129
Alcohol
Alcoholisresponsibleforabout10%ofunselectedattendancesatemergencydepartments,andahigherpercentageofattendanceswithtrauma.75Whilstmanypatientsattendtheemergencydepartmentasadirectandobviousresultofalcohol(forexampleafteradrinkingbinge,orinastateofwithdrawal),approximately 20%ofpatientsadmittedtohospitalforillnessesunrelatedtoalcoholareregularlyconsumingunsafelevelsofalcohol,representing‘the future burden of alcohol misuse on hospital services.75Alcoholproblemsoftengounrecognised,76althoughthereisgoodevidencethatforpeoplewhoaredrinkingabovesafelimits,detectionfollowedbyabriefalcoholinterventionresultsinsignificantreductionsinalcoholconsumptionpostdischarge.77
Disturbed behaviour
Thisisdefinedasbehaviourthatinterfereswithaperson’scareorsafety,orthe careandsafetyofothers.About4%ofgeneralhospitalpatientsdisplaydisturbedbehaviour,anditismorecommoninmalesthanfemales.78Inmostcasesaggressivebehaviourisdirectedtowardsstaffratherthanotherpatients.Althoughanuncommonoccurrence,disturbedbehaviouronageneralhospitalwardcanconsumeadisproportionateamountofresources,particularlystafftime.78There areproventechniquesinpreventing,de-escalatingandmanagingdisturbedbehaviour;79theuseofsedativemedicationinphysicallyunwellpeopleisriskyandrequiresexpertise.
Dementia
Dementiaaffectsapproximately30%ofelderlypeopleadmittedtoanacutegeneralward.15Patientswithdementiaareparticularlyvulnerableingeneralhospitals.Theyarehighlysusceptibletoenvironmentalchangeandmayfinditdifficulttocommunicatetheirneeds,forexampleregardingtoiletingorpainrelief.Bettermanagementofdementiainhospitalcanresultinimprovedfunctionanddecreasedlengthofstay.80
Delirium
Deliriumoccursin15-20%ofallgeneralhospitaladmissionsandratesareconsiderablyhigherinelderlypatients(upto60%)especiallythosewithdementia.15 Thesedisordersoftengoundetectedinthegeneralhospital;forexample,acutestaffmaynotrecognisedeliriumin50%ofcases.81Verylittleisknownatpresentabouthowtoidentifypatientsathighriskofdevelopingdelirium,althoughthosepatientswiththreeormoreriskfactorsareninetimesmorelikelytodevelopdeliriumduringtheirhospitalstaythanpatientswithout.15Havingdementiaincreasestheriskofdeliriumfivefold.15

22
No HealtH witHout MeNtal HealtH
Liaison psychiatry services improve the care of patients with such problems
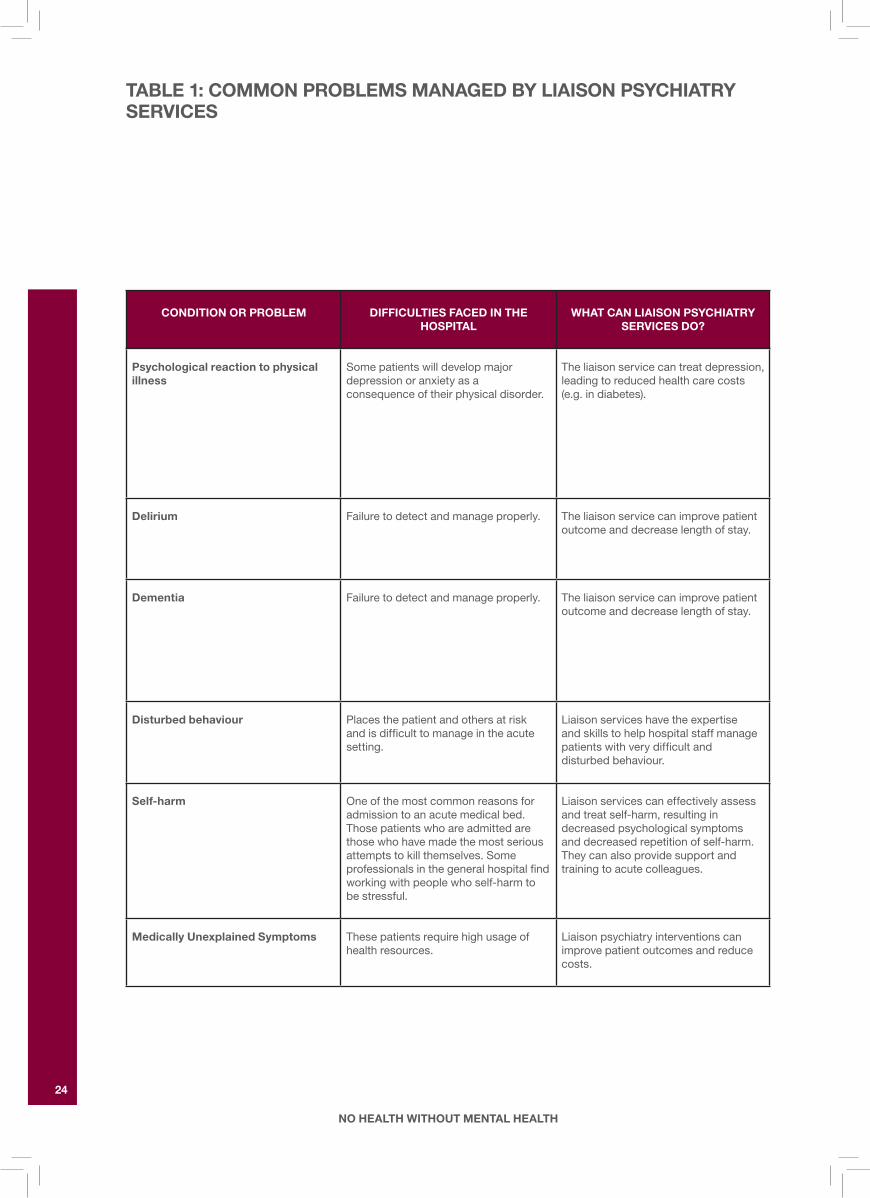
Table1summarisesthewaysinwhichliaisonmentalhealthservicescanhelpwithsomeofthecommonproblemsassociatedwithmentaldisorderamongpatientsinthegeneralhospital.Manyliaisonmentalhealthteamsincludepsychologistsornurseswithexpertiseincognitivetherapyandotherpsychologicaltherapies.Aswellasprovidingdirectpatientcare,liaisonstafftrainandsupportgeneralhospitalstaffinthebetterdetectionandtreatmentofmentalhealthproblems.Thiscanresultinmorepositiveattitudestowardsmentalillhealthandgreaterconfidenceinaddressingemotionaldistressexpressedbypatientsorpatients’relatives.Healthpsychologyandclinicalpsychologyalsoprovidespecificpsychologicaltreatmentforpeoplewithdepressionandanxiety,butdonotcoverthewholerangeofmentalhealthproblemsthatpresentinageneralhospital.
box 8: Risk factors associated with developing delirium during a hospital stay
predisposing factors precipitating factors
•Visionimpairment •Useofphysicalrestraints•Severeillness •Malnutrition/dehydration•Cognitiveimpairment •Morethanthreemedicationsadded•Raisedbloodurea/creatinine •Useofbladdercatheter •Anyiatrogenicevent(harmful
consequenceofaprocedure orintervention

No HealtH witHout MeNtal HealtH
23
24
No HealtH witHout MeNtal HealtH
CONDiTiON OR pRObLEM DiFFiCuLTiES FACED iN ThE hOSpiTAL
WhAT CAN LiAiSON pSyChiATRy SERviCES DO?
psychological reaction to physical illness
Somepatientswilldevelopmajordepressionoranxietyasa consequenceoftheirphysicaldisorder.
Theliaisonservicecantreatdepression,leadingtoreducedhealthcarecosts(e.g.indiabetes).
Delirium Failuretodetectandmanageproperly. Theliaisonservicecanimprovepatientoutcomeanddecreaselengthofstay.
Dementia Failuretodetectandmanageproperly. Theliaisonservicecanimprovepatientoutcomeanddecreaselengthofstay.
Disturbed behaviour Placesthepatientandothersatrisk andisdifficulttomanageintheacutesetting.
Liaisonserviceshavetheexpertise andskillstohelphospitalstaffmanagepatientswithverydifficultand disturbedbehaviour.
Self-harm Oneofthemostcommonreasonsforadmissiontoanacutemedicalbed.Thosepatientswhoareadmittedarethosewhohavemadethemostseriousattemptstokillthemselves.Someprofessionalsinthegeneralhospitalfindworkingwithpeoplewhoself-harmtobestressful.
Liaisonservicescaneffectivelyassessandtreatself-harm,resultingindecreasedpsychologicalsymptomsanddecreasedrepetitionofself-harm.Theycanalsoprovidesupportandtrainingtoacutecolleagues.
Medically unexplained Symptoms Thesepatientsrequirehighusageofhealthresources.
Liaisonpsychiatryinterventionscanimprovepatientoutcomesandreducecosts.
TAbLE 1: COMMON pRObLEMS MANAGED by LiAiSON pSyChiATRy SERviCES
No HealtH witHout MeNtal HealtH
25
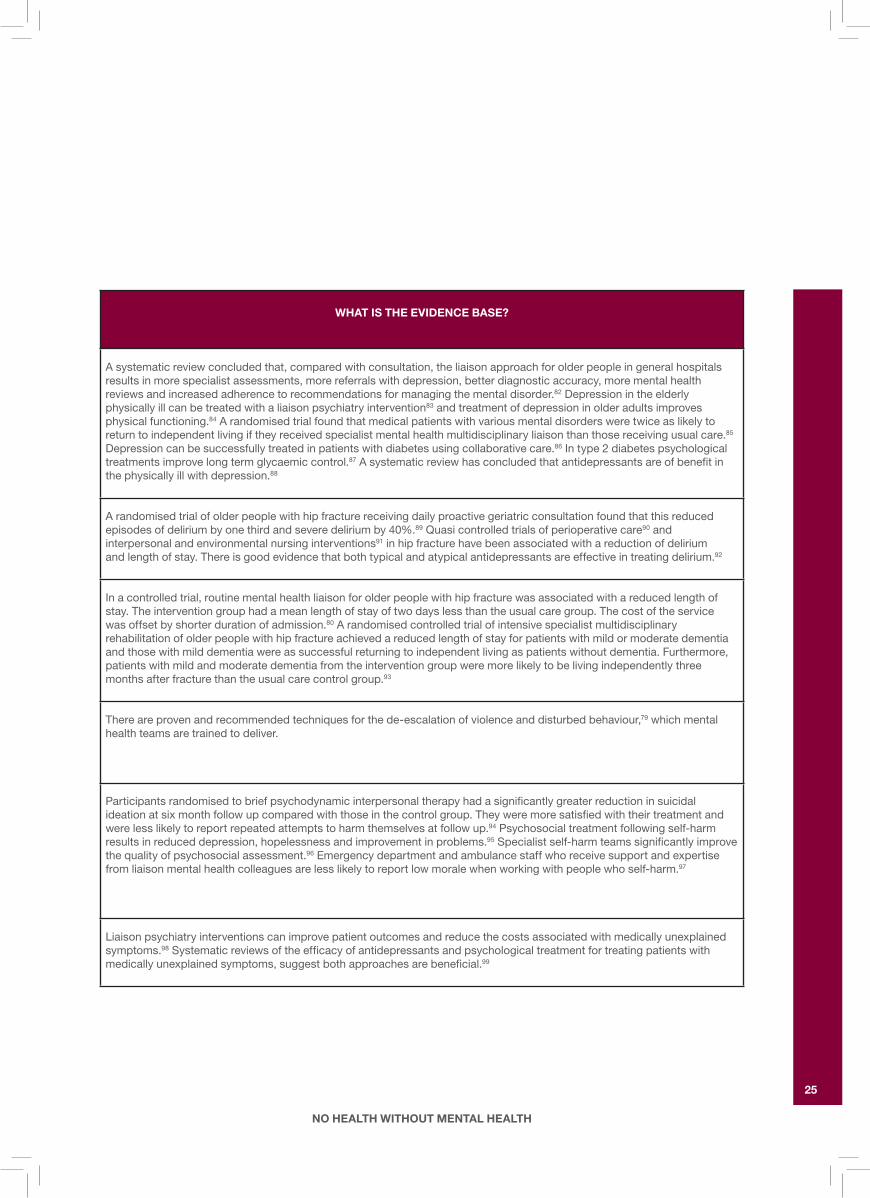
WhAT iS ThE EviDENCE bASE?
Asystematicreviewconcludedthat,comparedwithconsultation,theliaisonapproachforolderpeopleingeneralhospitalsresultsinmorespecialistassessments,morereferralswithdepression,betterdiagnosticaccuracy,morementalhealthreviewsandincreasedadherencetorecommendationsformanagingthementaldisorder.82Depressionintheelderlyphysicallyillcanbetreatedwithaliaisonpsychiatryintervention83andtreatmentofdepressioninolderadultsimprovesphysicalfunctioning.84Arandomisedtrialfoundthatmedicalpatientswithvariousmentaldisordersweretwiceaslikelytoreturntoindependentlivingiftheyreceivedspecialistmentalhealthmultidisciplinaryliaisonthanthosereceivingusualcare.85 Depressioncanbesuccessfullytreatedinpatientswithdiabetesusingcollaborativecare.86Intype2diabetespsychologicaltreatmentsimprovelongtermglycaemiccontrol.87Asystematicreviewhasconcludedthatantidepressantsareofbenefitin thephysicallyillwithdepression.88
Arandomisedtrialofolderpeoplewithhipfracturereceivingdailyproactivegeriatricconsultationfoundthatthisreducedepisodesofdeliriumbyonethirdandseveredeliriumby40%.89Quasicontrolledtrialsofperioperativecare90 and interpersonalandenvironmentalnursinginterventions91inhipfracturehavebeenassociatedwithareductionofdelirium andlengthofstay.Thereisgoodevidencethatbothtypicalandatypicalantidepressantsareeffectiveintreatingdelirium.92
Inacontrolledtrial,routinementalhealthliaisonforolderpeoplewithhipfracturewasassociatedwithareducedlengthofstay.Theinterventiongrouphadameanlengthofstayoftwodayslessthantheusualcaregroup.Thecostoftheservice wasoffsetbyshorterdurationofadmission.80Arandomisedcontrolledtrialofintensivespecialistmultidisciplinaryrehabilitationofolderpeoplewithhipfractureachievedareducedlengthofstayforpatientswithmildormoderatedementiaandthosewithmilddementiawereassuccessfulreturningtoindependentlivingaspatientswithoutdementia.Furthermore,patientswithmildandmoderatedementiafromtheinterventiongroupweremorelikelytobelivingindependentlythreemonthsafterfracturethantheusualcarecontrolgroup.93
Thereareprovenandrecommendedtechniquesforthede-escalationofviolenceanddisturbedbehaviour,79whichmentalhealthteamsaretrainedtodeliver.
Participantsrandomisedtobriefpsychodynamicinterpersonaltherapyhadasignificantlygreaterreductioninsuicidalideationatsixmonthfollowupcomparedwiththoseinthecontrolgroup.Theyweremoresatisfiedwiththeirtreatmentandwerelesslikelytoreportrepeatedattemptstoharmthemselvesatfollowup.94Psychosocialtreatmentfollowingself-harmresultsinreduceddepression,hopelessnessandimprovementinproblems.95Specialistself-harmteamssignificantlyimprovethequalityofpsychosocialassessment.96Emergencydepartmentandambulancestaffwhoreceivesupportandexpertise fromliaisonmentalhealthcolleaguesarelesslikelytoreportlowmoralewhenworkingwithpeoplewhoself-harm.97
Liaisonpsychiatryinterventionscanimprovepatientoutcomesandreducethecostsassociatedwithmedicallyunexplainedsymptoms.98Systematicreviewsoftheefficacyofantidepressantsandpsychologicaltreatmentfortreatingpatientswithmedicallyunexplainedsymptoms,suggestbothapproachesarebeneficial.99

26
No HealtH witHout MeNtal HealtH
CONDiTiON OR pRObLEM DiFFiCuLTiES FACED iN ThE hOSpiTAL
WhAT CAN LiAiSON pSyChiATRy SERviCES DO?
Alcohol Abuse Thereispoormanagementofalcoholwithdrawalstatesresultinginincreasedlengthofstayorunnecessaryadmissions.
Briefliaisoninterventionscanbeeffectiveinthereductionofalcoholusebypatientsidentifiedashavingalcoholproblemsinthegeneralmedicalsetting.
people who attend the ED regularly (‘frequent attenders’)
Thesepatientsarehighusersofhealthresourcesandmorelikelytoexperiencepoorermentalhealth.
LiaisonpsychiatrycanhelpEDstaffmanagepatientsappropriatelyandensurepatientsareofferedappropriatecommunitybasedservices.Casereviewscanalsobeundertakenwhereappropriate.
Lack of mental capacity TheMentalCapacityActandtheAdultswithIncapacity(Scotland)Acthighlighttheneedforrapidassessmentsofcapacitytoconsenttomedicaltreatmentinthegeneralhospitalsetting.FailuretoimplementtheseActsappropriatelymaydisadvantagethepatient.Itcanalsoresultinlegalaction.
AnexperiencedConsultantLiaisonPsychiatristmightbebestequippedtomakeaninformedjudgementaboutcapacityforpatientswithcomplexphysicalandmentalhealthproblems.
Severe mental illness Asmallproportionofmedicalin- patientshaveseverementalillness (e.g.schizophrenia).Thesepatientscausegreatanxietyingeneralhospitalstaffandthereareoftenmajorriskissueswhichneedtobemanaged.
LiaisonServicescanrespondrapidlyandprovideacontinuityofservicebetweencommunityandhospitalwhilstthepatient’sphysicalneedsarebeingattendedto.
All mental health problems Generallackofknowledgeandskillsamongstgeneralhospitalstaffinthedetectionandmanagementofanymentalhealthproblem.
Educationandtrainingdeliveredbyliaisonservicesimproveknowledge,skillsandattitudesamongstgeneralhospitalstaff.
TAbLE 1: COMMON pRObLEMS MANAGED by LiAiSON pSyChiATRy SERviCES CONT.
No HealtH witHout MeNtal HealtH
27
WhAT iS ThE EviDENCE bASE?
Heavydrinkerswhoreceiveabriefalcoholinterventionaretwiceaslikelytomoderatetheirdrinkingsixto12monthsafteraninterventionwhencomparedwithheavydrinkerswhoreceivenointervention.100Inthegeneralhospitalsetting,heavydrinkerswhoarecounselledabouttheirdrinkinghaveasignificantlybetteroutcomethancontrolswhenfollowed-up12monthslater.77
50%ofpatientswhofrequentlyattendtheEDhavementalhealthproblems.91LiaisonmentalhealthstaffcanhelpEDstafftounderstandtheneedsofthisgroupandthereasonswhytheyuseservicesfrequently.102Thereareveryfewcontrolledstudiesofpsychiatricinterventioninthisgroupofpatients.ArecentstudysuggeststhatmultidisciplinarycasemanagementhasapositiveeffectonpsychosocialfactorsforfrequentattendeesbutincreasesEDutilisation.103
40%ofacutemedicalpatientsdonothavementalcapacitytomakeinformeddecisionsaboutmedicaltreatment,andclinicalteamsrarelyidentifypatientswhodonothavecapacity.104LiaisonpsychiatristsreceivemandatorytrainingintheassessmentofcapacityinrelationtotheMentalCapacityActinEnglandandWales.SomeliaisonpsychiatristswillalsobetrainedtoprovideassessmentsundertheDeprivationofLibertySafeguards(DOLS):thenewlegalframeworktosafeguardtherightsofpeoplewholackcapacityandneedtobedetainedinasafeenvironment.
NICEhaspublishedclinicalguidelinesonthetreatmentandmanagementofschizophrenia105andbipolardisorder.106
NICEhaspublishedguidanceonthetreatmentandmanagementofmostmentalhealthandbehaviouralconditionsincludingin2009aguidelineondepressioninchronichealthproblems(www.nice.org.uk).Psychiatrictreatmenthasshowntobeeffectiveintreatingpatientswithcomplexphysicalandmentalhealthproblems.107
28
No HealtH witHout MeNtal HealtH
Liaison psychiatry services are not limited to a general hospital setting
Integratedclinicalassessmentandtreatmentserviceshavebeensetupasaway ofmanagingreferralsintosecondarycareandprovidingpatientswithrapidaccesstoassessmentandtreatment.Liaisonpsychiatryservicescanbeembeddedintothesenewservicessothatpsychologicalproblemsandtreatablementalillnesscanbeaccessedinparallelwithphysicalhealthtreatment.Liaisonservicescanalso linkmorecloselywithprimarycaretoprovidesupervisionforprimarycarepractitionersforcomplexcasesandprovidegreatercontinuityofcareforpatientswithlongtermconditions.
box 9: providing mental health services to emergency departments (ED)
Inmanyareas,mentalhealthinputtotheEDisprovidedbyCrisisResolution andHomeTreatmentTeams(CRHTs),asystemwhichhastheadvantageofproviding24hourcover.However,theseteamsareexpectedtoprioritisepatientsinthecommunity,withamajorfocusonhometreatment,meaningthattheyarenotalwaysabletorespondpromptlytopatientsintheED.LiaisonpsychiatryoffersanalternativewayofprovidingmentalhealthprovisiontoEDs,eitherthroughliaisonteamsbasedentirelyintheEDorpreferablyviateamssetup tomanageurgentmentalhealthneedsthroughoutthewholeofthehospital. Thiswouldhelpensureequalaccesstomentalhealthcareforallgeneral hospitalpatients.
box 10: Links between liaison psychiatry and primary care
Therearetwokeyareaswhereliaisonmentalhealthservicescandirectlysupporttheworkofprimarycarepractitioners:
• Thecareofpeoplewhohavepsychologicalreactionstophysicalillness• Thecareofpeoplewithmedicallyunexplainedsymptoms.
InformationaboutthedetectionandmanagementofboththesehealthproblemsisavailableinarecentjointreportbytheRoyalCollegeofGeneralPractitionersandtheRoyalCollegeofPsychiatristsentitled‘TheManagementofPhysicalandPsychologicalProblemsinPrimaryCare:Apracticalguide’.ThetwocollegeshavealsorecentlyestablishedaForumforMentalHealthinPrimaryCare.Theaimsoftheforumaretoguideandpromotegoodpracticeinmentalhealthcare,actasanexpertresource,andinfluencenationalpolicyandstrategy. (www.rcpsych.ac.uk/college/mentalhealthinprimarycare.aspx)
Mentalhealthservicesshouldestablisheffectiveliaisonwithlocalprimarycareteammembersandotheragenciestoprovideonwardcarepathways.

No HealtH witHout MeNtal HealtH
29
Links with community learning disability services
Inmostareas,communitylearningdisabilityservicescanofferaccesstoarange ofprofessionalswhoareskilledinworkingwithpeoplewhohavelearningdisabilities.Theseprofessionalscanhelppatientsaccessprimaryandsecondarycare.Thiscanbeahelpfulresourceforpatients,generalhospitalstaffandliaisonmentalhealthteams,asthelearningdisabilityprofessionalwilloffersupportregardingassessmentandtreatment,andwherenecessary,anyconcurrentchallengingbehaviour.
box 11: providing mental health liaison to maternity services
Psychiatricdisorderisaleadingcauseofmaternalmorbidityandmortality, yetlessthanhalfofmentalhealthtrustsintheUKprovidespecialised perinatalpsychiatricliaisonasrecommendedbythematernaldeaths enquiries.108,109,110
Perinatalliaisonservicesareideallyplacedto:
• Provideexpertadviceandsupporttomaternityprofessionalsonthe individualriskandbenefitsofpsychiatrictreatmentduringpregnancy andbreastfeeding
• Seeindividualpatientsincrisisandconductassessments.
Mentalhealthprovisiontomaternityservicesshouldideallyoccurwithinanetworkwhichincludesaccesstospecialisedinpatientmotherandbabyunits ifnecessary.108,109Thisensuresthatthemostseriouslyillwomencanquicklyaccesstheappropriatelevelofcarewithoutunnecessarilybeingseparated fromtheirbabies.

30
No HealtH witHout MeNtal HealtH
Thissectionaddressestwoaspectsofpatientengagement;theimportanceofinvolvingpatientsintheirowncare;andthebroaderissueofinvolvingpatientsandcarersinservicedesign,deliveryandimprovement.
To be actively engaged in their care, patients need to be better informed
TheNationalInstituteforHealthandClinicalExcellence(NICE)andtheScottishIntercollegiateGuidelinesNetwork(SIGN)emphasisetheimportanceofprovidinginformationthatenablespatientstoexercisechoiceintheircareandtreatment.NICEhasrecentlyproducedaguidelineonMedicinesAdherence111thatis ‘about enabling patients to make informed choices by involving and supporting them in decisions about prescribed medicines’.
Many patients would like to be more involved and better informed
Asurveyofmorethan50,000inpatientsinEnglishgeneralhospitals112demonstratedthatalthoughmostweregenerallysatisfiedwiththecaretheyreceivedfromtheNHS,manyexpressedconcernsaboutlackofchoiceandinformationabouttreatmentandcare.Otherpatientandcarersurveysrevealsimilarfindings.113
Well informed patients experience less anxiety and better outcomes
Patientswhoarewellinformedaboutprognosisandtreatmentoptionsaremorelikelytoadheretotreatmentsandhavebetterhealthoutcomes.114Theyarealso lesslikelytoexperienceanxietyinrelationtohealthscreening115andoperativeprocedures.116Communicationisalsoimportant.Forexample,whenworkingwithpatientsforwhomEnglishisnottheirfirstlanguage,staffneedtomakesufficienttimeavailableforanindividualtoexpressandexplainthemselvesfully.Thisalsoallowstimetogainabetterunderstandingofculturalnormsandvalues.
box 12: Survey of over 50,000 adult inpatients
• Threequartersofthosewhoseadmissiontohospitalwereplannedin advancewasnotgivenachoiceofadmissiondates
• Halffeltthattheywereinvolvedindecisionsabouttheirdischarge,30% saidthattheywereinvolvedtosomeextentand17%feltthattheywere notinvolved
• Halfofthepatientswhotookmedicinehomewerenotgiveninformation aboutthepossiblesideeffects
• Duringtheirhospitalstay,only6%wereaskedtogivetheirviewsonthequalityoftheircare
• Athirdsaidthatstaffdidnotgivetheirfamilyorcareralltheinformation theyneededtohelpcareforthem
• Halfofpatientsdidnotreceivecopiesofletterssentbetweenhospital doctorsandtheirfamilydoctor.
5. ENGAGiNG pATiENTS AND CARERS

No HealtH witHout MeNtal HealtH
31
Engagement includes taking account of mental distress
Somepeoplewithmentalandphysicalhealthproblemsfeelthatgeneralhospitalstaffdonottaketheiremotionalwellbeingintoaccount.Forexample,manypeoplewhoattendhospitalfollowingself-harmreportthatstaffdonotaskabouttheiremotionaldistressandonethirdofemergencydepartmentstaffreportedthattheyshowedlessrespectandofferedlesssupporttopeoplewhoself-harmcomparedwithotherpatients.117Theattitudeofprofessionalscanhaveaprofoundimpactonpatientsandcarers:
“The nurse made such a difference to me just by taking the time out to chat and being sensitive to how mixed I was feeling about the situation” –Adultattendingtheemergencydepartmentfollowingself-harm,2007
patients can be supported to self-manage long term disease
TheExpertPatientsProgramme118isauser-ledself-managementprogrammespecificallyforpeoplelivingwithlongtermconditions.Theaimoftheprogrammeistosupportpeoplebyincreasingtheirconfidence,improvingtheirqualityoflifeandenablingthemtobettermanagetheircondition.Havingbeensuccessfullypiloted,theExpertPatientsProgrammecurrentlyoffersaround12,000courseplacesayear.Itisbeingmadeavailablethroughprimarycaretrustsandpartnerorganisations.Workisunderwaytoadaptcoursesforpeoplewithmentalhealthproblems,andforcarers.Feedbackfromaround1,000patientswhocompletedthecoursebetween2003and2005indicatesthattheprogrammeisachievingimprovedhealthoutcomesforpatientsandreducingthedegreetowhichtheyusehealthcareservices.
box 13: What do people with physical and mental health problems want from services?
A2004study113foundthattwothirdsofrespondentshadproblemsaccessingmentalhealthservicesbecauseoftheirphysicalimpairment.Asimilarproportionhaddifficultiesusingphysicaldisabilityservicesbecauseoftheirmentalhealthneeds.Whenaskedwhattheywantedfromservices,keyfactorswere:
• Forgeneralhospitalstafftotakeaccountofpatients’mentalhealthneeds,withoutmakingnegativejudgementsorbehavinginaderogatorymanner
• Forstafftotakeseriouslythepatient’sownviewoftheirhealth,andnottointerpretphysicalimpairmentspurelyasamanifestationofmentalillness. Oneperson,forexample,saidthat,whenhewasinhospital,‘the fact that I said I had [asthma and arthritis] was seen as an aspect of mental illness’
• Formentalhealthstafftohaveagreaterunderstandingofphysicalhealthneeds,withouthavingnegativeattitudesorlowexpectationsofthepatient
• Forallhealthcareprofessionalstohaveagreaterunderstandingoftherelationshipbetweenmentalandphysicalhealth
• Forstafftotreatthepatientasawholepersonandnotadisease• Formentalhealthprofessionalstotakeaccountofaccessneedsrelating
tophysicalimpairment,andviceversa• Clearcommunicationandpositiveattitudesfromstaff:“He was actually
helpful because he seemed normal and he didn’t use words that were not understandable”.

32
No HealtH witHout MeNtal HealtH
There remains a stigma around mental illness
Manypatientsfeelembarrassedtotalkabouttheiremotionalproblemsforfearof anegativeresponsefromhealthservicestaff,andthereremaindeeplyentrenchedviewsamongstsomecliniciansthatmentalhealthproblemsareshamefulorasignofweakness.Liaisonpsychiatryservicesarewellplacedtochallengestigmatisingviewsofmentalillness,througheducation,trainingandhighvisibilityinacutemedicalsettings.119
involving patients in service development, research and audit can improve mental health care in the acute setting
TheNHSPlan120placespatientsatthecentreofservicedesignanddelivery.Ideallythisinvolvementshouldextendtotheplanningoflocalservices,recruitment,trainingandeducationofstaff,research,clinicalauditandserviceevaluation. Box15illustrateshowthiscanworkinpractice.
box 14: Engaging with carers
Considerationshouldbegiventothesupportneedsofpeoplewhocareforsomeonewithmentalandphysicalhealthproblems.Carersmayfinditdifficult toaccesshealthprofessionalsandthehealthofcarersisalsooftenoverlooked.
box 15: involving service users in the improvement of self-harm services
TheRoyalCollegeofPsychiatrists’‘BetterServicesforPeoplewhoSelf-harm’projectwasestablishedin2005(www.rcpsych.ac.uk/cru/auditselfharm.htm).Peoplewhoself-harmwereinvolvedonmanylevels,includingdeveloping trainingmaterialsandcoursesforclinicians,providingtraining,designingdatacollectiontoolsandwritingreportsandrecommendations.Usersworkedalongsideambulance,emergencydepartmentandmentalhealthstafftoplanserviceimprovementthroughmeetings,workshopsandpeer-reviewvisitstootherhospitals.NHSstaffdescribedtheirinputas‘very helpful’inbringing aboutpositivechangeasdescribed:
“[They gave] an insight of what it is like to receive a service...a good relationship was established, allowing a freedom to share views, even those of a potentially controversial nature. It felt that service users were extremely active and equal partners and played a significant role in the project. For this we thank them.”
Many of the service users involved gained from the experience:
“I have been able to develop training skills which has led to me being invited to join the planning team for student nursing training at a local university. I have gained sufficient confidence in my own abilities to be able to return to work, albeit part time and in a junior position, for the first time in six years.”
“All my trouble with self-harm has finally been put to use and my experiences have been invaluable in helping improve things. I feel useful!”

No HealtH witHout MeNtal HealtH
33
BothNICEandSIGNinvolvepatientsandcarersintheprocessofdevelopingtheirclinicalpracticeguidance.InEngland,LordDarziconcludedinhis2008reportthat‘Peoplewantagreaterdegreeofcontrolandinfluenceovertheirhealthandhealthcare’.122Inkeepingwiththis,thefocusintheNHSisshiftingfromtreatmentoutcomesthataredefinedbythecliniciantothosethataredefinedbythepatient.ThisisreflectedintheDepartmentofHealth’sworktodevelopPatientReportedOutcomesMeasures(PROMS)foruseinperformancemanagementofservices.
There are many barriers to involving patients and carers in improving services
Inrealityhowever,theoftenverygoodintentionsofinvolvingpatients‘cansometimesfailtomovebeyondrhetoricintoreality’121andrunstheriskofbeingtokenisticandsuperficial.Severalfactorscanhindermeaningfulinvolvement,includingpracticalbarriersrelatingtorecruiting,supportingandpayingusersandcarers.Someprofessionalsalsodescribedifficultiesinfindingpeoplewhoarerepresentativeofthe‘typicalpatient’butLindow123warnsthatthisshouldnotbe usedasareasontoexcludepatients:
“The most usual strategy to discredit user voices is to suggest that we are too articulate, and not representative…We ask how representative are others on the committee? We point out that as they are selected for their expertise and experience, so are we…We ask, would workers send their least articulate colleagues to present their views, or the least confident nurse to negotiate for a change in conditions?”
Itisequallyimportantthatpeopleshouldnotbedisenfranchisedpurelybecauseofintellectualimpairments.Whengivenappropriatesupportandopportunitypeoplewithlearningdisabilitiesandtheircarersarecapableofgivinginvaluableinsightsintopotentialbarrierstoeffectivehealthcare.63
The value of patient expertise should not be underestimated
‘By definition, no one else, no matter how well trained or qualified, can possibly have had the same experience of the onset of illness, the same contact with services or the same journey through the health system.121
Theseexperiencesareanimportantresourcethatcanhelptoimproveindividualpackagesofcareaswellasservicesgenerally.Wheninvolvingpatientsorcarersinanykindofservicerevieworimprovement,caremustbetakentoprovidetheappropriateemotional,financialandpracticalsupport.

34
No HealtH witHout MeNtal HealtH
General hospitals need flexible and responsive liaison mental health services
ThisistheviewoftheRoyalCollegeofPhysicians,RoyalCollegeofPsychiatristsandtheAcademyofMedicalRoyalColleges.70,81ARoyalCollegeofPhysicianstaskforcerecommendsthatacutementalhealthservices,includingthosededicatedtotheneedsofolderpeople,shouldbepartoftheacutespectrumofcare,and thatallfutureacutemedicalunitsshouldhaveasafeareaformanagingpatientswithacutementalhealthproblems,arelatives/carersroomandaroomforprivate orconfidentialinterviews.124
however, there is little incentive for the NhS to develop such services
Thisisbecauselocalmentalandphysicalhealthcareservicesarecommissionedseparatelyandmanagedbydifferentorganisations.Liaisonmentalhealthteamsarethereforenota‘must do’foreithermentalhealthoracuteservices.Asaresult,thereispatchyandinconsistentprovisionacrosstheUK.Whereahospitaldoeshavealiaisonmentalhealthservice,thisisinvariablyprovidedandmanagedbythelocalmentalhealthtrust.
TheDepartmentofHealth’sdriveforintegratedcare,especiallyforlongtermconditions,andtheshiftincommissioningtoprimarycareanddevelopmentof‘Practice Based Commissioning’,presentanopportunityforthedevelopment ofservicesinalessdualisticfashion.125
There are different models of service
However,liaisonpsychiatryservicesworkmosteffectivelywhentheyareembeddedintotheworkofthegeneralhospital.Thisallowsliaisonstafftoworkcloselywithgeneralstafftoimproverapiddetectionandtreatmentofpatientswithmentalproblemsinthegeneralhospitalsetting.Mostservicesincludetrainingandeducationalcomponentstoimprovetheoverallqualityofserviceprovisioninthegeneralhospital.Liaisonserviceswillalsohelpensureappropriateguidelines (e.g.NICEandSIGN)arebeingfollowedandthatclearpathwaysofcarearedevelopedforpatientswithparticularmentalhealthproblems.
Liaisonservicesshould‘map’ontothespecificneedsofanacutehospital.Asacutehospitalsvaryinsizeandservicedelivery,thesizeandmakeupofeachliaisonservicewillalsovary.Forexample,teachinghospitalsrequirelargerliaisonservicesthandistrictgeneralhospitals,becausetheyareusuallylargerandareoftenlocatedininnercityareaswithhighratesofdeprivation.Teachinghospitalsalsomanagepatientswhoaretertiaryreferrals(i.e.peoplewithhighlycomplexhealthproblems).
6. RE-ORGANiSATiON OF SERviCES, COMMiSSiONiNG AND QuALiTy STANDARDS
No HealtH witHout MeNtal HealtH
35
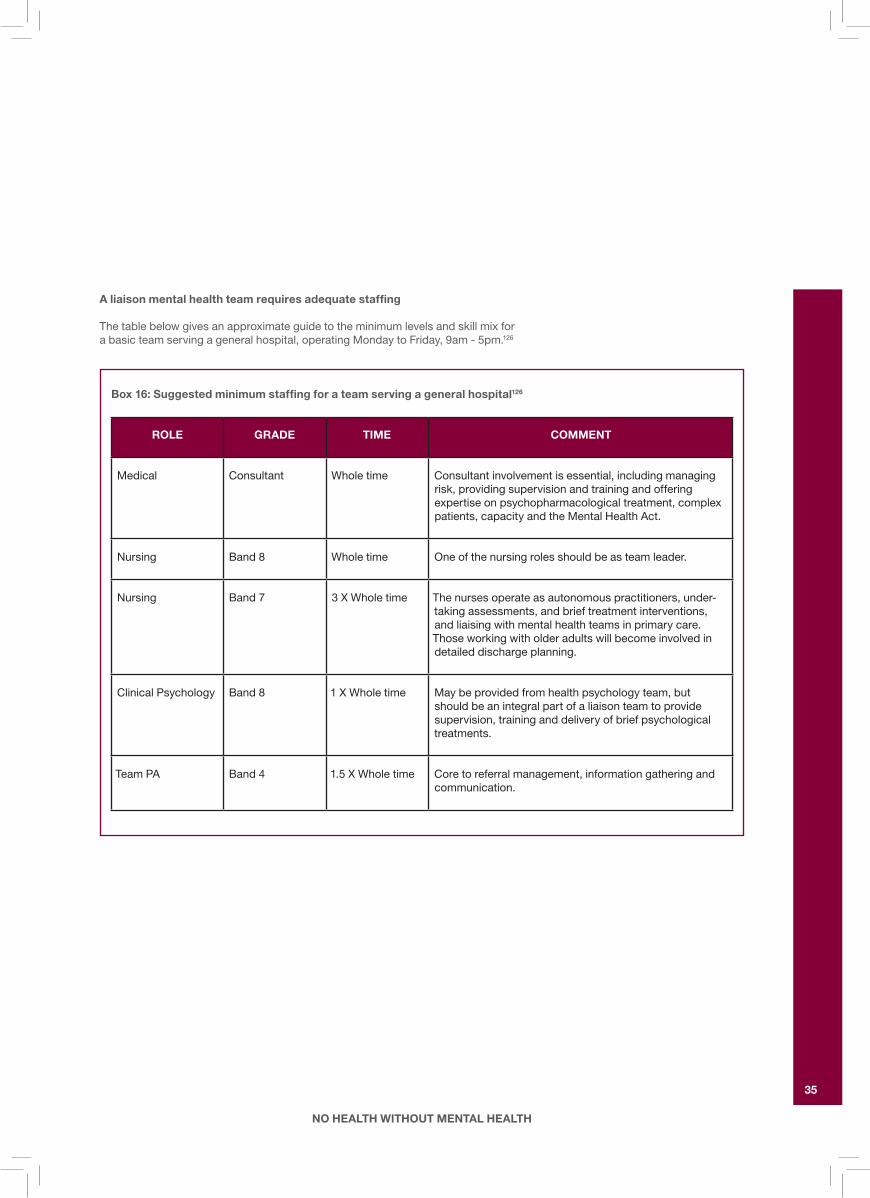
A liaison mental health team requires adequate staffing
Thetablebelowgivesanapproximateguidetotheminimumlevelsandskillmixforabasicteamservingageneralhospital,operatingMondaytoFriday,9am-5pm.126
box 16: Suggested minimum staffing for a team serving a general hospital126
ROLE GRADE TiME COMMENT
Medical Consultant Wholetime Consultantinvolvementisessential,includingmanagingrisk,providingsupervisionandtrainingandofferingexpertiseonpsychopharmacologicaltreatment,complexpatients,capacityandtheMentalHealthAct.
Nursing Band8 Wholetime Oneofthenursingrolesshouldbeasteamleader.
Nursing Band 7 3XWholetime Thenursesoperateasautonomouspractitioners,under-takingassessments,andbrieftreatmentinterventions,andliaisingwithmentalhealthteamsinprimarycare.Thoseworkingwitholderadultswillbecomeinvolvedindetaileddischargeplanning.
ClinicalPsychology Band8 1XWholetime Maybeprovidedfromhealthpsychologyteam,butshouldbeanintegralpartofaliaisonteamtoprovidesupervision,traininganddeliveryofbriefpsychologicaltreatments.
TeamPA Band4 1.5XWholetime Coretoreferralmanagement,informationgatheringandcommunication.

36
No HealtH witHout MeNtal HealtH
Thesestaffinglevelsrepresenttheabsoluteminimum,andadditionalcoverwouldalmostcertainlyberequired,dependingonthepopulationserved.Toprovideacomprehensiveliaisonservicewhichspecificallycatersforthespecialneedsofadultswithcomplexneedsanddementia,greaternumbersofthestafflistedabovearerequired.Inaddition,theteamwouldalsorequireatleastonefulltimeoccupationaltherapist,1.5WTEsocialworker,sessionsfromasupportworkerandadditionaladministrativesupport.Thestaffinglevelsrequiredtoprovidealiaisonservicetoolder-agedpatientsareavailableathttp://www.rcpsych.ac.uk/PDF/RaisingtheStandardOAPwebsite.pdf.
Ifliaisonprofessionalsaretoprovideteaching,trainingandsupporttocolleagueswithintheirteamandthroughoutthegeneralhospital;thestaffingratiosabovewouldneedtobeincreasedtoallowforthis.
Finally,thetableabovedoesnotincludechildandadolescentmentalhealthservices(CAMHS)togeneralhospitals.ThisoughttobeprovidedbyspecialistmultidisciplinaryCAMHSliaisonteams,butcurrentprovisioniscurrentlypatchy andfurtherinvestmentisrequired.
Quality Standards WeneedqualitystandardsformentalhealthcareingeneralhospitalsThesewouldclarifytheroleofliaisonservices,andprovideameansbywhich tomeasureandimprovethequalityofcaretheyprovide.Ina2008reportbytheAcademyofMedicalRoyalColleges,127theChairoftheAcademyemphasised theimportanceofsettingsuchqualitystandards(Box17).
The psychiatric Liaison Accreditation Network will support implementation
TheRoyalCollegeofPsychiatrists’CentreforQualityImprovement(CCQI)hasestablishedanationalaccreditationprogrammeformentalhealthservicestogeneralhospitals(www.rcpsych.ac.uk/PLAN).
box 17: The importance of setting standards
“We witness mental distress and mental illness daily, in people of all ages and in many different circumstances. Yet in our society they command less priority than do physical problems….the same standard of assessment, diagnosis and intervention should be provided for mental health care as is expected for physical health care. This requires an extension of current standards to cover practice in these acute services, commissioning of services and assessment of performance.”
-ProfessorDameCarolBlack,Chair,AcademyofMedicalRoyalColleges
No HealtH witHout MeNtal HealtH
37
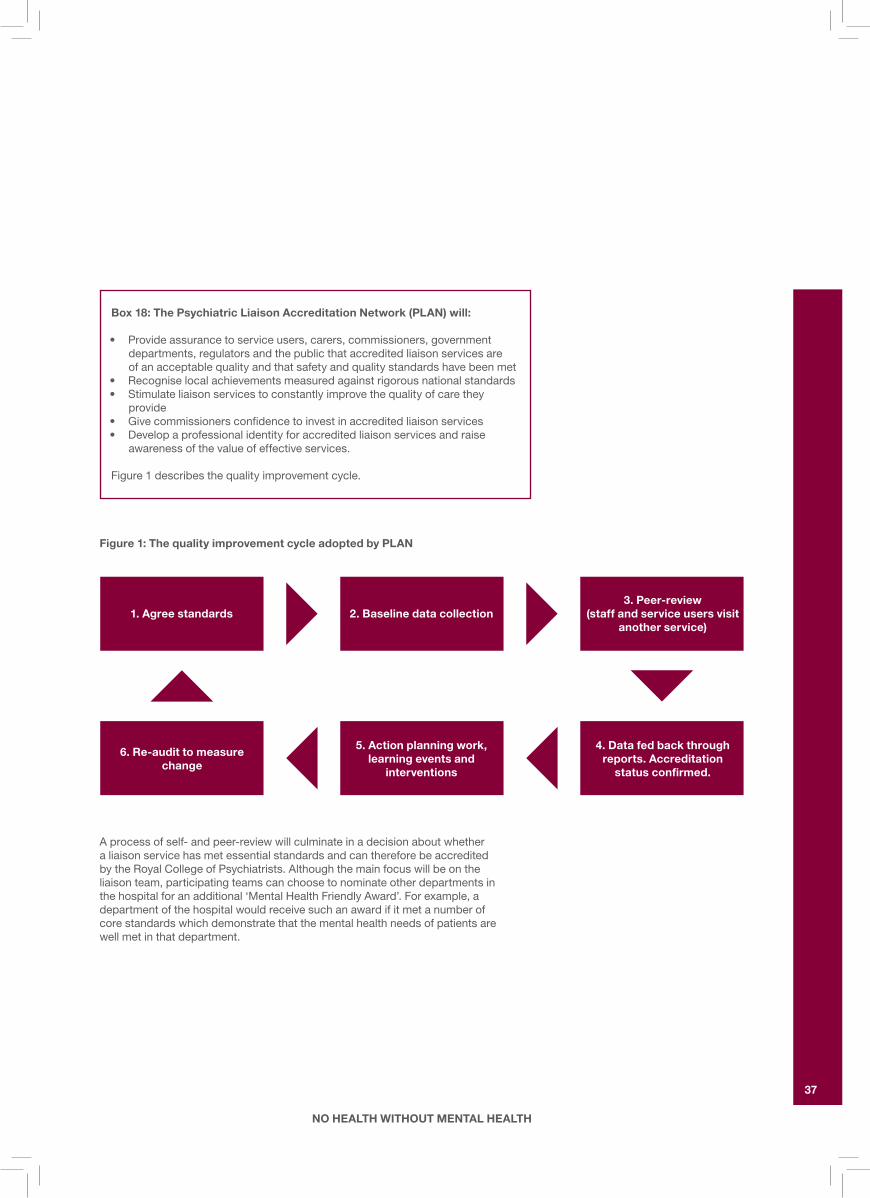
Figure 1: The quality improvement cycle adopted by pLAN
Aprocessofself-andpeer-reviewwillculminateinadecisionaboutwhether aliaisonservicehasmetessentialstandardsandcanthereforebeaccredited bytheRoyalCollegeofPsychiatrists.Althoughthemainfocuswillbeonthe liaisonteam,participatingteamscanchoosetonominateotherdepartmentsin thehospitalforanadditional‘MentalHealthFriendlyAward’.Forexample,adepartmentofthehospitalwouldreceivesuchanawardifitmetanumberof corestandardswhichdemonstratethatthementalhealthneedsofpatientsare wellmetinthatdepartment.
box 18: The psychiatric Liaison Accreditation Network (pLAN) will:
• Provideassurancetoserviceusers,carers,commissioners,governmentdepartments,regulatorsandthepublicthataccreditedliaisonservicesare ofanacceptablequalityandthatsafetyandqualitystandardshavebeenmet
• Recogniselocalachievementsmeasuredagainstrigorousnationalstandards• Stimulateliaisonservicestoconstantlyimprovethequalityofcarethey
provide• Givecommissionersconfidencetoinvestinaccreditedliaisonservices• Developaprofessionalidentityforaccreditedliaisonservicesandraise
awarenessofthevalueofeffectiveservices.
Figure1describesthequalityimprovementcycle.
1. Agree standards 2. baseline data collection
5. Action planning work, learning events and
interventions
6. Re-audit to measure change
3. peer-review (staff and service users visit
another service)
4. Data fed back through reports. Accreditation
status confirmed.

38
No HealtH witHout MeNtal HealtH
Many healthcare professionals would welcome better mental health training
ThelackofintegratedthinkingaboutphysicalandmentalhealthintheNHSmeansthatthereisarealneedforhealthcareprofessionalstoacquireagreaterunderstandingoftherelationshipbetweenmentalandphysicalhealth.However,recentrecommendationsandauditfindingsreflectthefactthatmanyhealthcareprofessionalshavenotbeenprovidedwithadequatementalhealtheducation:
Doctors need better training in the detection and treatment of mental health problems in patients who are physically ill
MostUKmedicalstudentsreceiverelativelylittletraininginmentalhealth,andmostofthatfocusesonthemanagementofsevereandenduringmentalhealth.Medicalgraduatesinitiallybecomefoundationdoctorsfortwoyears,duringwhichtimetheyacquirethemajorityoftheircorementalhealthcompetenciesinanticipationofbecominggeneralpractitionersorhospitalspecialists.132
box 19: Training needs of general hospital staff and Gps
• In2003,theRoyalCollegesofPhysiciansandPsychiatristsrecommendedthatcommissionersensureimprovedtrainingofgeneralhospitalstaffin thementalhealthneedsofolder-agedadults81
• Atthesametime,theChildren’sNationalServiceFrameworkstatedthatliaisonarrangementsshouldprovidefortheeducationandtrainingofallchildren’shealthcarestaffinthementalhealthneedsofchildrenandtheirfamilies110
• In2008,theAcademyofMedicalRoyalCollegesrecommendedbetter mentalhealthtrainingopportunitiesforstaffinemergencydepartments,medical,paediatricandsurgicalwards127
• TheHealthPromotionAgencyforNorthernIrelandsurveyedover500 primarycareprofessionalsin2008andfoundthateightoutof10wanted moretraininginrecognisingmentalhealthproblems,suicide,self-harm andmentalhealthpromotion.Barrierstotrainingwereidentifiedasalack oftimeandalackofaccess.Asuggestedsolutiontothisproblemwas onlinetraining128
• Arecentauditfoundthatmorethanhalfof500emergencydepartment staffwouldhavelikedtheirinitialtrainingtoincludemoreemphasison mentalhealth129
• VariousNICEandSIGNguidelinesstipulatetheneedforbettermental healthawarenessamongstphysicalhealthprofessionals(www.nice.org.uk)
• Traininginrelationtotheneedsofpeoplewithlearningdisabilityisalsogenerallyinadequateleavingmanyhealthcareprofessionalsfeelinguncomfortableandunprepared130
• ThelearningdisabilitycomponentoftheRoyalCollegeofPsychiatrists’curriculumforbasicspecialisttrainingemphasisestheimportanceofrecognisingtheinfluenceofphysicalfactorsonpsychologicalpresentation. Itisessentialthatgeneralhospitalstaffaretrainedaboutnotjustthehighratesofandatypicalpatternsofhealthdeficitsinpeoplewithlearningdisability,butalsothepotentialatypicalpresentationofphysicalsymptoms.131
7. TRAiNiNG AND EDuCATiON

No HealtH witHout MeNtal HealtH
39
Thefoundationcurriculumemphasisestheimportanceofpsychological,socialandculturalfactorsintheassessmentandmanagementofphysicallyillpatients.Morespecifically,foundationdoctorsmustbeabletomanagepatientsfollowingself-harm,withanacuteconfusionalstateandwithpsychosis.Theyarealsorequiredtodeveloppositiveattitudes,inwhichtheymustconsidertheimpactof:132
• Physicalproblemsonpsychologicalandsocialwell-being• Physicalillnesspresentingwithpsychiatricsymptoms• Psychiatricillnesspresentingwithphysicalsymptoms• Somatisation• Familydynamics.
However,thedichotomyofcarebetweenmentalhealthandacutetrustsorNHSboardscanmakeacquisitionofthesecompetenciesverydifficult.Thereareanumberofwaysinwhichmentalhealthstaffcanfacilitatetheprocess:
• Generalhospitalshaveweeklygrandroundswhichshouldbeattendedbymultidisciplinarymembersoftheliaisonpsychiatryteam,whoshouldalsotaketheirturninpresentinganddiscussingcasesandissuesofsharedinterest
• Mentalhealthprofessionalsshouldparticipateintheregularteachingofacutetruststaff–notonlyintheformalsettingofcontinuingprofessional development–butalsoonthewards.Sharingknowledgeandattitudesduringroutinecareofferstheopportunityofinvolvingthepatient’sownperspective andexpectations
• Mentalhealthprofessionalsshoulddevelopworkingrelationshipswithacutecareunitswheretheprevalenceofpsychologicalmorbidityisparticularlyhigh– suchasrheumatologyandgastroenterology.Thedaytodaypresenceofmentalhealthprofessionalsontheseunitspromoteslearningandincreasedawarenessofmentalhealthissues
• Mentalhealthprofessionalscantraincolleaguesintheuseofeasilyimplementedmentalhealthscreeningquestionnaires,whichimprovestaffawarenessforpsychologicalandpsychiatriccomplications.TheHospitalAnxietyandDepressionScaleisawellvalidatedself-ratingscaleforusein thegeneralhospital.133
box 20: All doctors working in a general hospital setting should be able to:
• Elicitpatient’sconcernsaboutillnessinasensitiveandcompetentmanner• Screenfordepressionandanxiety• AssesscognitivefunctionusingtheMiniMentalStateExamination• Carryoutabasicriskassessmentforsuicideandself-harm• Beabletoassessbasiccapacitytogiveconsentformedicaltreatment• Detectdementiaanddeliriumandtreattheseappropriately• Detectsymptomsofdrugandalcoholwithdrawalandtreatthese
appropriately.

40
No HealtH witHout MeNtal HealtH
Competencies need to be checked
‘Knowing Why’and‘Knowing How’,usuallytestedbywrittenandclinicalexams,arenotconsideredtobesufficientevidenceofcompetence.ThecurrentgoldstandardistheWorkplaceBasedAssessment,particularlyasthisincludesfeedbackandreflectivepractice.Twoofthese,currentlyapprovedbythePostgraduateMedicalEducationandTrainingBoard,lendthemselvesparticularlywelltothedevelopmentofintegratedphysicalandmentalhealthskills:
• CaseBasedDiscussion(CBD):IntheCBDthehealthcareprofessionaldiscussesanindividualpatient.Thetrainercanfocustheconversationonaspectsofmanagementthatrequireattentiontophysicalandpsychologicalneeds,andcanhelpidentifypointsofstrengthandareasthatcouldbedevelopedfurther
• Mini-ClinicalExamination(mini-CEX):Inthemini-CEX,whichusuallylasts10-15minutes,thehealthcareprofessionalinteractswithapatientwhilstbeingobserved.Theexercisecould,forexample,betoassessthepatient’smood,theimpactoftheirphysicalillnessontheiremotionalhealth,ortheirunderstandingoftheirillness.Again,thetrainerorsupervisorcanfocusthesubsequentfeedbackanddiscussiononareasrelevanttointegratedcare.
Training in primary care needs to be improved
Therearealsoopportunitiesforteachingandawarenessraisinginprimarycare.Recentdevelopmentssuchasprimarycarementalhealthteams,GPswithspecialinterestsinmentalhealth,theImprovingAccesstoPsychologicalTherapies(IAPT)ProgrammeandtheGatewayWorkersProgrammeraiseawarenessofmentalhealthissuesandaccesstotreatmentsinprimarycare.Theseteamsneedtotrainandsupportactivecasemanagersandpatientswithlongtermconditionstointegratephysicalandpsychologicalcare.Secondarycarementalhealthspecialistsneedtotrain,superviseandsupportprimarycarestafftoacquireandmaintainrelevantmentalhealthskills.
TheRoyalCollegeofPsychiatristsandtheRoyalCollegeofGeneralPractitionersrecentlyrecommendedthatGPsintrainingwouldbenefitfromspendinganattachmentinLiaisonPsychiatry.134Thetypeofmentalhealthproblemsseenbyliaisonpsychiatryservicesaremorediversethanthoseseenbyteamswhospecialiseinthetreatmentofseverementalillness,andtheproblemsaremorerelevanttothosemostfrequentlyencounteredbyGPsintheirdailypractice. Thecollegesalsorecommendedthatmorepsychiatrictraineesshouldspenda sixmonthattachmentinprimarycare.ThenewlyestablishedForumforMentalHealthinPrimaryCarealsoprovidesusefulupdatesaboutpsychologicalaspects ofphysicalhealthandactsasanexpertresource (www.rcpsych.ac.uk/college/mentalhealthinprimarycare.aspx).
Manypatientswithchronicconditionssuchaspainareincreasinglylikelytobeseeninintermediatecaresettings.Newservicesneedtoincludementalhealthspecialistssothatstaffbecomefamiliarwithmanagingtheinterfacebetweenphysicalandpsychologicalcare,andtrainingneedsshouldbeprioritised.
Finally,thenationalguidelinesdevelopedbyNICEandSIGNrelatingtophysicalconditionsvaryintermsofmentalhealthcontent(seewww.rcpsych.ac.uk/nohealthforadetaileddescription).Itisvitalthatnationalguidanceensuresthatmentalhealthissuesreceiveadequatefocus.

No HealtH witHout MeNtal HealtH
41
ItishopedthattheALERTreportwillnotonlyenhanceunderstandingofthe linkbetweenmentalandphysicalhealth,butalsoprovideamuchneededimpetus forthedevelopmentofbetterservicesforthissignificantandlargelyneglectedgroupofpatients.Moresubstantialmentalhealthprovisionacrossthegeneralhospitalsettingwillbenefitpatients,carersandhealthcareprofessionalsfrom allbackgrounds.ItisenvisagedthattheMedicalRoyalCollegesandotherorganisationswillworktogethertomaketherecommendationsinthisreport areality.
8. SuMMARy

42
No HealtH witHout MeNtal HealtH
This report has been compiled by:
professor Else Guthrie ChairoftheFacultyofLiaisonPsychiatry,RoyalCollegeofPsychiatrists.HonoraryProfessorofPsychologicalMedicineandMedicalPsychotherapyUniversityofManchester
Lucy palmer ProgrammeManager,NoHealthwithoutMentalHealthProjectRoyalCollegeofPsychiatrists’CentreforQualityImprovement
Dr paul Lelliott DirectoroftheRoyalCollegeofPsychiatrists’ResearchandTrainingUnit
Dr Carolyn Chew-Graham SeniorLecturerinPrimaryCare,UniversityofManchesterGeneralPractitioner,Manchester.ClinicalChampionforMentalHealth,RoyalCollegeofGeneralPractitioners
professor Derek bell ProfessorofAcuteMedicineatImperialCollegeConsultantPhysicianatChelseaandWestminsterHospitalNHSFoundationTrustRoyalCollegeofPhysicians’representativeonthePsychiatricLiaisonAccreditationNetwork
Deborah Agulnik ProjectWorker,NoHealthwithoutMentalHealthProjectRoyalCollegeofPsychiatrists’CentreforQualityImprovement
With valuable contributions from:
Dave Anderson AssociateMedicalDirector/Consultant,MerseycareNHSTrust
Janey Antoniou ServiceuserAdvisor,RoyalCollegeofPsychiatrists
Roger banks VicePresident,RoyalCollegeofPsychiatrists
Alan Carson ConsultantinNeuropsychiatry,DepartmentofClinicalNeurosciencesandDepartmentofPsychiatry,UniversityofEdinburgh
irene Cormac ConsultantForensicPsychiatrist,RamptonHospital
Chris Dickens SeniorLecturerinPsychologicalMedicine,UniversityofManchester
Melanie DupinProjectWorker,RoyalCollegeofPsychiatrists
Charlotte Edwards HonoraryResearchAssistant,RoyalCollegeofPsychiatrists
ACKNOWLEDGEMENTS

No HealtH witHout MeNtal HealtH
43
paul Gill ConsultantLiaisonPsychiatrist,SheffieldCareTrust
Max henderson MRCResearchTrainingFellow,KingsCollegeLondon,InstituteofPsychiatry
peter hindleyConsultantChildandAdolescentPsychiatrist,StThomas’Hospital
Sheila hollinsProfessorofPsychiatryofLearningDisability,StGeorge’sUniversityofLondon
Khalida ismail ClinicalReader,DepartmentofPsychologicalMedicine,InstituteofPsychiatry
Glyn Jones ConsultantPsychiatrist,DirectorateofLearningDisabilityServices,AbertaweBroMorgannwgUniversityNHSTrust
Damien LongsonConsultantLiaisonPsychiatrist,ManchesterHead,SchoolofPsychiatry,NorthWestDeanery
Jackie Macklin ServiceUserAdvisor,RoyalCollegeofPsychiatrists
Satveer Niijar ServiceUserAdvisor,RoyalCollegeofPsychiatrists
Margaret Oates ConsultantinPerinatalPsychiatry(retired)
Johan Redelinghuys ConsultantPsychiatrist,WestLondonNHSMentalHealthTrust
Guy Sanders ConsultantinEmergencyMedicine,RoyalSussexCountyHospital,Brighton
Geraldine Swift ConsultantinLiaisonPsychiatry,CheshireandWirralPartnership,NHSFoundationTrust
barry Wright ConsultantChildPsychiatrist,HonorarySeniorLecturer,HullYorkMedicalSchool
With thanks to:
Rosie Carlow PublicationsManager,AcademyofMedicalRoyalColleges
James Taylor Designer

44
No HealtH witHout MeNtal HealtH
1. Charmaz,K.Lossofself:afundamentalformofsufferinginthechronicallyill.Sociology of Health & Illness 2008;5(2):168-195.
2. KellyB,BurnettP,PelusiD,BadgerS,VargheseFRobertsonM.Terminallyillcancerpatients'wishtohastendeath.Palliat Med 2002;16(4):339-45.
3. GuthrieE,JacksonJ,ShafferJ,ThompsonD,TomensonB,CreedF.Psychologicaldisorderandseverityofinflammatoryboweldiseasepredicthealth-relatedqualityoflifeinulcerativecolitisandCrohn'sdisease. The American Journal of Gastroenterology2004;97(8):1994-1999.
4. DowdyD,EidP,SedrakyanA,Mendez-TellezP,PronovostP,HerridgeM,NeedhamD.Qualityoflifeinadultsurvivorsofcriticalillness:Asystematicreviewoftheliterature. Intensive Care Medicine2005;31(5):611-620.
5. KatonW.Clinicalandhealthservicesrelationshipsbetweenmajordepression,depressivesymptoms,andgeneralmedicalillness. Biol Psychiatry2003;54(3):216-26.
6. PattenS.LongtermmedicalconditionsandmajordepressioninaCanadianpopulationstudyatwaves1and2.J Affect Disord2001;63:35-41
7. MacHaleS.Managingdepressioninphysicalillness.Advances in Psychiatric Treatment 2002;8:297-305.TheRoyalCollegeofPsychiatrists
8. DepartmentofHealth.NationalServiceFrameworkforChildren. Gettingtherightstart:StandardforHospitalServices.2003.
9. WestcottH,CrossM.This far and no further: towards ending the abuse of disabled children.Birmingham:VenturePress,1996.
10. NationalWorkingGrouponChildProtectionandDisability,2003.
11. LeeM.UKinquiryintomentalhealthandwell-beinginlaterlife. Improvingservicesandsupportforolderpeoplewithmentalhealthproblems. AgeConcern;2007.
12. HarwoodD,HawtonK,HopeT,JacobyR.Psychiatricdisorderandpersonalityassociatedwithsuicideinolderpeople:adescriptiveandcase–controlstudy. Int J Geriatr Psychiatry2001;16:155–156.
13. CiechanowskiPS,WalkerEA,KatonWJ,RussoJE.AttachmentTheory:Amodelforhealthcareutilizationandsomatisation. Psychosom Med2002;64:660-667.
14. MarazzitiD,MungaiF,VivarelliL,PrestaS,Dell’ossoB.Painandpsychiatry:acriticalanalysisandpharmacologicalreview.Clin Pract Epidemol Ment Health 2006;2:31:10.1186/1745-0179-2-31
15. RoyalCollegeofPsychiatrists. Who Cares Wins. Improving the outcome of Older people admitted to the general hospitals. Guidelines for the development of liaison mental health services for older people. RoyalCollegeofPsychiatrists,2005.
16. BarthJ,SchumacherM,Herrmann-LingenC.Depressionasariskfactorformortalityinpatientswithcoronaryheartdisease:ameta-analysis.Psychosom Med2004;66:802–13.
REFERENCES AND FuRThER READiNG

No HealtH witHout MeNtal HealtH
45
17. FanVS,RamseySD,GiardinoND,MakeBJ,EmeryCF,DiazPTetal. Sex,depression,andriskofhospitalizationandmortalityinchronic obstructivepulmonarydisease.Arch Intern Med2007;167:2345–2353.
18. StapletonRD,NielsonEL,EngelbergRA,PatrickDL,CurtisJR.Association of depression and life-sustaining treatment preferences in patients with COPD.CHESTJanuary2005vol.127no.1328-334.
19. PohjasvaaraT,VatajaR,LeppavuoriA,KasteM,ErkinjunttiT.Depressionis anindependentpredictorofpoorlongtermfunctionaloutcomepoststroke. Eur J Neurol 2001;8:315–319.
20. CepoiuM,McCuskerJ,ColeMG,SewitchM,BelzileE,CiampiA. Recognitionofdepressionbynon-psychiatricphysicians—Asystematic literaturereviewandmeta-analysis.J Gen Intern Med 2008;23(1):25–36.
21. GoldbergD,HuxleyP.Common mental disorders.London:Routledge;1992.
22. Chew-GrahamCA,HoggT.Patientswithchronicphysicalillnessandco-existingandco-existingpsychologicalmorbidity:GPs’viewsontheirroleindetectionandmanagement.Primary care psychiatry 2002;8(2):35-39.
23. BurroughsH,MorleyM,LovellK,BaldwinR,BurnsA,Chew-GrahamCA.“Justifiabledepression”:Howhealthprofessionalsandpatientsviewlate-lifedepression;aqualitativestudy. Family Practice 2006;23:369-377.
24. KesslerD,LloydK,LewisG,GrayDP.Crosssectionalstudyofsymptomattributionandrecognitionofdepressionandanxietyinprimarycare.British Medical Journal1999;Feb13;318(7181):436-9.
25. NHSInformationCentre.QualityOutcomesFramework. http://www.qof.ic.nhs.uk/
26. KirmayerLJ,GroleauD,LooperKJ,DaoMD.Explainingmedicallyunexplainedsymptoms.Can J Psychiatry 2004;49:663-672.
27. HenningsenP,ZimmermannT,SattelH.Medicallyunexplainedphysicalsymptoms,anxiety,anddepression:ameta-analyticreview. Psychosom Med 2003;65:528–33.
28. KroenkeK,SpitzerR,WilliamsJ,LinzerM,HahnS,deGruyF,BrodyD.Physicalsymptomsinprimarycare.Predictorsofpsychiatricdisordersandfunctionalimpairment.ArchiveofFamilyMedicine1994;3:774–79.
29. JacksonJ,FiddlerM,KapurN,WellsA,TomensonB,CreedF.Numberofbodilysymptomspredictsoutcomemoreaccuratelythanhealthanxietyinpatientsattendingneurology,cardiologyandgastroenterologyclinics. J Psychosom Res2006;60,353–359.
30. NimnuanC,HotopfM,WesselyS.Medicallyunexplainedsymptoms: anepidemiologicalstudyinsevenspecialities.J Psychosom Res2001;51(1):361.
31. HimelhochS,WellerW,WuAW,AndersonGF,CooperLA.Chronicmedicalillness,depression,anduseofacutemedicalservicesamongmedicarebeneficiaries. Med Care2004;42(6):512-521.
32. Egede,L.Comorbiddepressionisassociatedwithincreasedhealthcareuse andexpendituresinindividualswithdiabetes.Diabetes Care2002;25(3):464-70.
46
No HealtH witHout MeNtal HealtH
33. LauzonL,BeckCA,HuynhT,DionD,RacineN.Depressionandprognosisfollowinghospitaladmissionbecauseofacutemyocardialinfarction.Can Med Assoc J 2003;168(5):547-552
34. vanMelleJ,deJongeP,SpijkermanT,TijssenJ,OrmelJ,vanVeldhuisenDetal.
Prognosticassociationofdepressionfollowingmyocardialinfarctionwithmortalityandcardiovascularevents:ameta-analysis.Psychosom Med2004;66:814-822.
35. NgT,NitiM,TanW,CaoZ,Ong,K,EngP.Depressivesymptomsandchronicobstructivepulmonarydisease:effectonmortality,hospitalreadmission,symptomburden,functionalstatus,andqualityoflife.Arch Intern Med.2007;167(1):60-67.
36. HolmesJ,HouseA.Psychiatricillnessinhipfracture.Age Ageing2000;29:537-546.
37. DisabilityRightsCommission.‘EqualTreatment:ClosingtheGap’2006. A formal investigation into physical health inequalities experienced by people with learning disabilities and/or mental health problems.
38. HarrisE,BarracloughB.Excessmortalityofmentaldisorder.Br J Psychiatry 1998;173:11-53.
39. NationalInstituteofHealthandClinicalExcellence.The management of bipolar disorder in adults, children and adolescents, in primary and secondary care. NICE,2006.
40. AndersonRJ,FreedlandKE,ClouseRE,LustmanPJ.Theprevalenceof comorbiddepressioninadultswithdiabetes:Ameta-analysis.Diabetes Care 2001;24:1069-1078.
41. RuguliesR.Depressionasapredictorofcoronaryheartdisease:asystematicreviewandmeta-analysisoftheliterature. Am J Prev Med2003;23:51-61.
42. Hippisley-CoxJ,VinogradovaY,CouplandC,ParkerC.RiskofMalignancy inPatientswithSchizophreniaorBipolarDisorder.ArchGenPsychiatry.2007;64(12):1368-1376.
43. BindmanJ,TigheJ,ThornicroftG,LeeseM.Poverty,poorservices,andcompulsorypsychiatricadmissioninEngland.SocPsychiatryPsychiatrEpidemiol.2002Jul;37(7):341-5.
44. StaffordM,MarmotM.Neighbourhooddeprivationandhealth:doesitaffectus allequally?IntJEpidemiol.2003Jun;32(3):357-66.
45. WeichS,LewisG.Materialstandardofliving,socialclass,andtheprevalenceofthecommonmentaldisordersinGreatBritain.Journal of Epidemiology and Community Health1998;52:8-14.
46. LasserK,BoydJW,WoolhandlerS.Smokingandmentalillness.JAMA2000;284:2606-10.
47. DepartmentofHealth.Atleastfiveaweek: Evidence on the impact of physical
activity and its relationship to health. A report from the Chief Medical Officer. DH,2004b.
48. McCreadieR.Diet,smokingandcardiovascularriskinpeoplewithschizophrenia:descriptivestudy, Br J Psychiatry2003;183:534-39.

No HealtH witHout MeNtal HealtH
47
49. DemblingBP,ChenDT,VachonL.Lifeexpectancyandcausesofdeathinapopulationtreatedforseriousmentalillness.Psychiatr Serv 1999;50:1036-1042.
50. SmithM,HopkinsD,PevelerRC,HoltRIG,WoodwardM,IsmailK.First-v.second-generationantipsychoticsandriskfordiabetesinschizophrenia:systematicreviewandmeta-analysis.Br J Psychiatry 2008;192(6):406-411.
51. JoukamaaM,HeliovaaraM,RaitasaloR,LehtinenV.Schizophrenia,neuroleptic
medicationandmortality.Br J Psychiatry2006;188:122-127.
52. GibsonPA,NewtonRW,SelbyK,PriceDA,LeylandK,AddisonGM.LongitudinalstudyofthyroidfunctioninDown’ssyndromeinthefirsttwodecades. Arch Dis Child2005;90:574-578.
53. Down’sSyndromeAssociationwebsite(2008)www.downs-syndrome.org.uk
54. WhittingtonJ,HollandT.Prader-WilliSyndrome:Development and Manifestations Cambridge:CambridgeUniversityPress;2004.20-25.
55. AndoN,UedaS.Functionaldeteriorationinadultswithcerebralpalsy. Clin Rehabil2000;14:300–306.
56. AsprayTJ,FrancisRM,ThompsonA,QuillamSJ,RawlingsDJ,TyrerSP.Comparisonofultrasoundmeasurementsattheheelbetweenadultswith mentalretardationandcontrolsubjects.Bone 1998;22:665-668.
57. HollinsS,AttardM,vonFraunhoferN,SedgwickP.Mortalityinpeoplewithlearningdisability;risks,causes,anddeathcertificationfindingsinLondon.Developmental Medicine & Child Neurology (1998).40:50-56.
58. CataldoM,HarrisJ.Thebiologicalbasisforself-injuryinthementallyretarded.Analysis and Intervention in Developmental Disabilities1982,2(1),21-39.
59. CooperSA,MelvilleCA,MorrisonJ.Peoplewithintellectualdisabilities. Theirhealthneedsdifferandneedtoberecognisedandmet. Br Med J2004;329:414-15.
60. DeathByIndifference;followinguptheTreatMeRight!Campaign.(2007) Mencap.http://www.mencap.org.uk/document.asp?id=284
61. DeafMentalHealthCharter(2008)CommissionedbySign(theNational SocietyforMentalHealthandDeafness)andtheMentalHealthFoundation www.mentalhealth.org.uk/our-work/all-adults/deaf-charter
62. LavisD,CullenP,RoyA.Identificationofhearingimpairmentinpeoplewith alearningdisability;fromquestioningtotesting.British Journal of Learning Disabilities;25,100-105
63. GibbsSM,BrownMJ,MuirW.Theexperiencesofadultswithintellectualdisabilitiesandtheircarersingeneralhospitals:afocusgroupstudy. J Intellect Disabil Res2008;52(Part12),1061-1077.
64. Lantman-deValkHM,WalshPN.Managinghealthproblemsinpeoplewithintellectualdisabilities.Br Med J 2008;337:1408-1412.
65. NurseyAD,RohdeJR,FarmerRD.Astudyofdoctors’andparents’attitudestopeoplewithmentalhandicaps.J Ment Defic Res 1990;34:143-55.

48
No HealtH witHout MeNtal HealtH
66. BrownS,FlynnMC,WistowG.Back to the Future: Joint Work for People with Learning Disabilities. London:NationalDevelopmentTeam&NuffieldInstituteforHealthServicesStudies,1992.
67. ValuingPeopleSupportTeam,StGeorge’sUniversityofLondon http://www.intellectualdisability.info/values/top_ten_tips.htm
68. PalmerL,StrevensP,BlackwellH.BetterServicesforPeoplewhoSelf-harm:
Keyfindingsfromtwobaselineaudits.Royal College of Psychiatrists,2007. 69. CreedF,FernandesL,TomensonB.Thecost-effectivenessofpsychotherapy
andparoxetineforsevereirritablebowelsyndrome.RandomizedControlledTrial.Gastroenterology2003;124(2):303-17.
70. RoyalCollegeofPhysicians&RoyalCollegeofPsychiatrists. The Psychological Care of Medical Patients. Recognition of Need and Service Provision. Council Report CR35.London:RoyalCollegeofPhysicians&RoyalCollegeofPsychiatrists,1995.
71. PalmerL,BlackwellH,StrevensP.Service Users’ Experience of Emergency Services Following Self-Harm: A National Survey of 509 patients. Better Services for People who Self-harm Programme. RoyalCollegeofPsychiatrists,2008.
72. NationalInstituteofClinicalExcellence(NICE)andtheNationalCollaboratingCentreforMentalHealth.The short-term physical and psychological management and secondary prevention of self-harm in primary and secondary care (National Clinical Practice Guideline Number 16).NICE,2004.
73. OwensD,DennisM,JonesS.Self-poisoningpatientsdischargedfrom accidentandemergency:riskfactorsandoutcome. J R Coll Physicians 1991;25(3):218–222.
74. HickeyL,HawtonK,FaggJ.Deliberateself-harmpatientswholeavetheaccidentandemergencydepartmentwithoutapsychiatricassessment:aneglectedpopulationatriskofsuicide.J Psychosom Res2001;50(2):87–93.
75. RoyalCollegeofPhysicians(RCP).Alcohol - can the NHS afford it? Recommendations for a coherent alcohol strategy for hospitals. Report of a working party of the Royal College of Physicians.RCP,2001.
76. VerrillC,SmithS,SheronN.AretheopportunitiestopreventalcoholrelatedliverdeathsintheUKinprimaryorsecondarycare?Aretrospectiveclinicalreview andprospectiveinterviewstudy.Subst Abuse Treat Prev Policy2006;1:16.
77. McManusS,HipkinsJ,HaddadP.Implementinganeffectiveintervention forproblemdrinkersonmedicalwards. Gen Hosp Psychiatry 2003;25(5): 332-337.
78. KannabiranM,DeshpandeS,WallingA,AlagarsamyJ,ProtheroeD,TrigwellP.Cross-sectionalsurveyofdisturbedbehaviourinpatientsingeneralhospitals inLeeds.Postgrad Med J2008;84(994):428-431.
79. NationalInstituteofClinicalExcellence(NICE)Guideline.Violence: The short-term management of disturbed/violent behaviour in in-patients psychiatric settings and emergency departments, CG25. NICE,2005.
80. StrainJJ,LyonsJS,HammerJS,FahsM,LebovitzA,PaddisonPLetal.
Costoffsetfromapsychiatricconsultationliaisonintervention withelderlyhipfracturepatients. Am J Psychiatry 1991;148:1044-9.

No HealtH witHout MeNtal HealtH
49
81. RoyalCollegeofPhysiciansandRoyalCollegeofPsychiatrists. The psychological care of medical patients. A practical guide. RCPandRoyalCollegeofPsychiatrists,2003.
82. DraperB.Theeffectivenessofoldagepsychiatryservices.Int J Geriatr Psychiatry 2000;15;687-703.129.
83. Cullum,TuckerS,ToddC,BrayneC.Effectivenessofliaisonpsychiatricnursing inoldermedicalinpatientswithdepression:arandomisedcontrolledtrial.AgeAgeing2007;36(4):436-442.
84. CallahanCM,KroenkeK,CounsellSR,HendrieHC,PerkinsAJ,KatonWetal.Treatmentofdepressionimprovesphysicalfunctioninginolderadults.J Am Geriatrics Soc 2005;53:367-373.
85. ColeMG,FentonFR,EngelsmanF,MansouriI.Effectivenessofgeriatricpsychiatryconsultationinanacutecarehospital:arandomisedclinicaltrial. J Am Geriatr Soc1991;39:1183-8.
86. KatonWJ,SimonG,RussoJ,vonKorffM,LinE,LudmanEetal.Qualityofdepressioncareinapopulation-basedsampleofpatientswithdiabetesand majordepression.Med Care 2004;42:1222-1229.
87. IsmailK,WinkleyK,Rabe-HeskethS.Systematicreviewandmeta-analysisofrandomised,controlledtrialsofpsychologicalinterventionstoimproveglycaemiccontrolinpatientswithtype2diabetes.Lancet 2004;363(9421);1589-97.
88. GillD,HatcherS.Antidepressantsfordepressioninmedicalillness. Cochrane Database of Syst Rev 2000,Issue4.Art.No.:CD001312. DOI:10.1002/14651858.CD001312.pub2.
89. MarcantonioER,FlackerJM,WrightRJ,ResnickNM.Reducingdeliriumafter hipfracture:arandomisedtrial.J Am Geriatr Soc 2001;49:516-22.
90. GustafsonY,BrannstromB,BerggrenD.Ageriatric-anaesthesiologicprogram toreduceacuteconfusionalstatesinelderlypatientstreatedforfemoralneckfractures. J Am Geriatr Soc 1991;39;655-62.
91. WilliamsRL,GuthrieE,Mackway-JonesK.Psychiatricstatus,somatisation, andhealthcareutilizationoffrequentattendersattheemergencydepartment. Acomparisonwithroutineattenders.J Psychosom Res 2001;50:161–7.
92. BourneRS,TahirTA,BorthwickM,SampsonEL.Drugtreatmentofdelirium: past,presentandfuture.J Psychosom Res 2008;65:273-82.
93. HuuskoTM,KarppiP,AvikainenV,KautiainenH,SulkavaR.Randomised,clinicallycontrolledtrialofintensivegeriatricrehabilitationinpatientswithhipfracture:subgroupanalysisofpatientswithdementia.BMJ2000;321:1107-1111.
94. GuthrieE,KapurN,Mackway-JonesK,Chew-GrahamC,MooreyJ,MendelEetal.Randomisedcontrolledtrialofbriefpsychologicalinterventionafterdeliberateselfpoisoning.BMJ 2001;323:135–138.
95. TownsendE,HawtonK,AltmanDG,ArensmanE,GunnellD,HazellPetal. Theefficacyofproblem-solvingtreatmentsafterdeliberateself-harm:meta-analysisofrandomizedcontrolledtrialswithrespecttodepression,hopelessnessandimprovementinproblems.Psychol Med 2001;31:979-988.

50
No HealtH witHout MeNtal HealtH
96. WhyteS,BlewettA.TheimpactofaspecialistDSHteamonassessmentquality.Psychiatr Bull 2001;25:98-101.
97. PalmerL,StrevensP,BlackwellH.Key Findings from 2 Baseline Audits: Findings from 38 UK Emergency Departments and their associated mental health and ambulance services.RoyalCollegeofPsychiatrists.2007.
98. SmithGRJr,RostK,KashnerTM.Atrialoftheeffectofastandardizedpsychiatricconsultationonhealthoutcomesandcostsinsomatisingpatients.Arch Gen Psychiatry 1995;52:238–243.
99. O’MalleyP,JacksonJ,SantoroJ.Antidepressanttherapyforunexplainedsymptomsandsymptomsyndromes.J Fam Pract.1999;48:980-990.
100. WilkAI,JensonNM,HavighurstC.Meta-analysisofrandomizedcontroltrialsaddressingbriefinterventionsinheavyalcoholdrinkers.J Gen Intern Med1997;12(5):274–283.
101. ChickJ,LloydG,Crombie,E.Counsellingproblemdrinkersinmedicalwards: acontrolledstudy.Br Med J 1985;290:965-967.
102. OlssonM,HansagiH.Repeateduseoftheemergencydepartment:qualitativestudyofthepatient'sperspective.Emerg Med J2001;18:430-434;doi:10.1136/emj.18.6.430.
103. PhilipsG,BrophyD,WeilandT,ChenhallA,DentA.Theeffectofmultidisciplinarycasemanagementonselectedoutcomesforfrequentattendersatanemergencydepartment.MJA 2006;184:602-606.
104. RaymontV,BingleyW,BuchananA,DavidA,HaywardP,WesselySetal.Prevalenceofmentalincapacityinmedicalinpatientsandassociatedriskfactors:cross-sectionalstudy. Lancet 2004;364(9443):1421-1427.
105. NationalInstituteofHealthandClinicalExcellence.Schizophrenia: core interventions in the treatment and management of schizophrenia in primary and secondary care CG82.NICE,2002.
106. NationalInstituteofHealthandClinicalExcellence.The management of bipolar disorder in adults, children and adolescents, in primary and secondary care CG38. NICE,2006.
107. StiefelF,ZdrojewskiC,BelHadgF,BoffaD,DorogiY,SoAetal.Effectsofamultifacetedpsychiatricinterventiontargetedforthecomplexmedicallyill: arandomizedcontrolledtrial.Psychother Psychosom 2008;77:247-56.
108. LewisG,editor.Saving mothers’ lives: reviewing maternal deaths to make motherhood safer - 2003-2005. The seventh report on confidential enquiries into maternal deaths in the United Kingdom.London:CEMACH;2007.
109. NationalInstituteforHealthandClinicalExcellence.Antenatal and postnatal mental health. Clinical management and service guidance. NICE Clinical Guideline 45.London:NICE;2007.
110. DepartmentofHealth.National Service Framework for Children, Young People and Maternity Services. Standard 11: Maternity Services.London:DH;2004.
111. NationalInstituteforHealthandClinicalExcellence(2009)NICEClinicalGuideline76:MedicinesAdherence–Quickreferencesheetforpharmacists

No HealtH witHout MeNtal HealtH
51
112. TheCareQualityCommission(formerlytheHealthcareCommission)SurveyofAdultInpatients(2008)http://www.cqc.org.uk/usingcareservices/healthcare/patientsurveys/hospitalcare/inpatientservices.cfm
113. Morris,J(2004)'Onetownformybody,anotherformymind':Servicesforpeoplewithphysicalimpairmentsandmentalhealthsupportneeds.JosephRowntreeFoundation.
114. Mullen,PD.Compliancebecomesconcordance.Br Med J1997;314:691–692.
115. HumphrisGM,IrelandRS,FieldEA.Randomisedtrialofthepsychologicaleffectofinformationaboutoralcancerinprimarycaresettings.Oral Oncology2001;37:7548-552Volume37,Issue7,Pages548-552.
116. PattonM,SchaerfR.Thoracotomy,criticalpathway,andclinicaloutcomes. Cancer Practice 1995;3(5):286-94.
117. PalmerL,StrevensP,Blackwell,H(2006)BetterServicesforPeoplewho
Self-Harm:DataSummary–Wave1BaselineData.
118. TheExpertPatientsWebsite.www.expertpatients.co.uk
119. BoltonJ.Howcanwereducethestigmaofmentalillness?BMJ 2003;326:s57-58.
120. DepartmentofHealth.The NHS Plan: a plan for investment, a plan for reform. 2000.
121. TaitandLester.Encouraginguserinvolvementinmentalhealthservices.Advances in Psychiatric Treatment 2005;11:168–175.
122. DepartmentofHealth(2008)HighQualityCareforAll:NHSNextStageReviewFinalReport,2008,pg9
123. Lindow,V.Power,liesandinjustice:theexclusionofserviceusers’voices. In:Parker,M,editor.EthicsandCommunityintheHealthCareProfessions. London:Routledge,1999.p.154–177.
124. RoyalCollegeofPhysicians.Acute medical care: The right person, in the right setting, first time'.RCP,2007.
125. DepartmentofHealthPracticeBasedCommissioningWebsitehttp://www.dh.gov.uk/en/Managingyourorganisation/Commissioning/Practice-basedcommissioning/DH_076565
126. RoyalCollegeofPsychiatrists’CentreforQualityImprovement.Mental Health Policy Implementation Guide: Liaison Psychiatry and Psychological Medicine in the General Hospital.RoyalCollegeofPsychiatristsCentreforQualityImprovement,2008.
127. TheAcademyofMedicalRoyalColleges.ManagingUrgentMentalNeedsintheAcuteTrust(2008).http://www.aomrc.org.uk/aomrc/admin/reports/docs/MHdoc.pdf
128. HealthPromotionAgencyforNorthernIreland.Assessment of training needs of primary care health professionals. Health promotion and the feasibility of delivering training through e-learning.HPA,2007.

52
No HealtH witHout MeNtal HealtH
129. HinchcliffeG,PalmerL,DupinM.TheviewsofEmergencyDepartmentprofessionalsworkingwithpeoplewhoself-harm(inpreparation). [email protected]
130. Duff.Moretrainingisneededinhealthcareofpeoplewithlearningdisabilities.BMJ 2000;321:385.
131. EvenhuisHM,MulM,LemaireEKG,deWijsJPM.Diagnosisofsensoryimpairmentinpeoplewithintellectualdisabilityingeneralpractice.J Intellect Disabil Res 1997;41:422–429.
132. TheFoundationprogramme.http://www.foundationprogramme.nhs.uk/pages/home/training-and-assessment
133. WhooleyMA,AvinsAL,MirandaJ,BrownerWS.Case-findinginstruments fordepression.Twoquestionsareasgoodasmany.J Gen Intern Med1997; 12(7):439-45.
134. RoyalCollegeofPsychiatristsandRoyalCollegeofGeneralPractitioners. The management of patients with physical and psychological problems in primary care: a practical guide Report of a joint working group. RoyalCollege ofPsychiatristsandRoyalCollegeofGeneralPractitioners,2009.
135.BaxterH,LoweK,HoustonH,JonesG,FelceD,KerrM.Previouslyunidentifiedmorbidityinpatientswithintellectualdisability.British Journal of General Practice February2006,93-98.
136.FelceD,BaxterH,LoweK,DunstanF,HoustonH,JonesGetal.Theimpactofrepeatedhealthchecksforadultswithintellectualdisabilities.Journal of Applied Research in Intellectual Disabilities 2008,21,585-596.
137.CooperS.A,MorrisonJ,MelvilleC,FinlaysonJ,AllanL,MartinGetal.Improvingthehealthofpeoplewithintellectualdisabilities:outcomesofahealthscreeningprogrammeafteroneyear.Journal of Intellectual Disability Research 50,667-677.

No HealtH witHout MeNtal HealtH
53

AcademyofMedicalRoyalColleges70WimpoleStreetLondonW1G8AX
RegisteredCharityNumber1056565
RoyalCollegeofPsychiatrists 17BelgraveSquare London,SW1X8PG
RegisteredCharityNumber228636