perioperative fluid management
TRANSCRIPT
Perioperative fluid management
麻醉部王審之
Osmolarity and tonicity
• Osmolarity is the measure of solute concentration, defined as the number of osmoles (Osm) of solute per litre (L) of solution (osmol/L or Osm/L).– osmole (Osm or osmol) is a unit of measurement that defines the
number of moles of a chemical compound that contribute to a solution's osmotic pressure.
• Tonicity takes into account the total concentration of only non-penetrating solutes.
• From Wikipedia
Crystalloid solutions
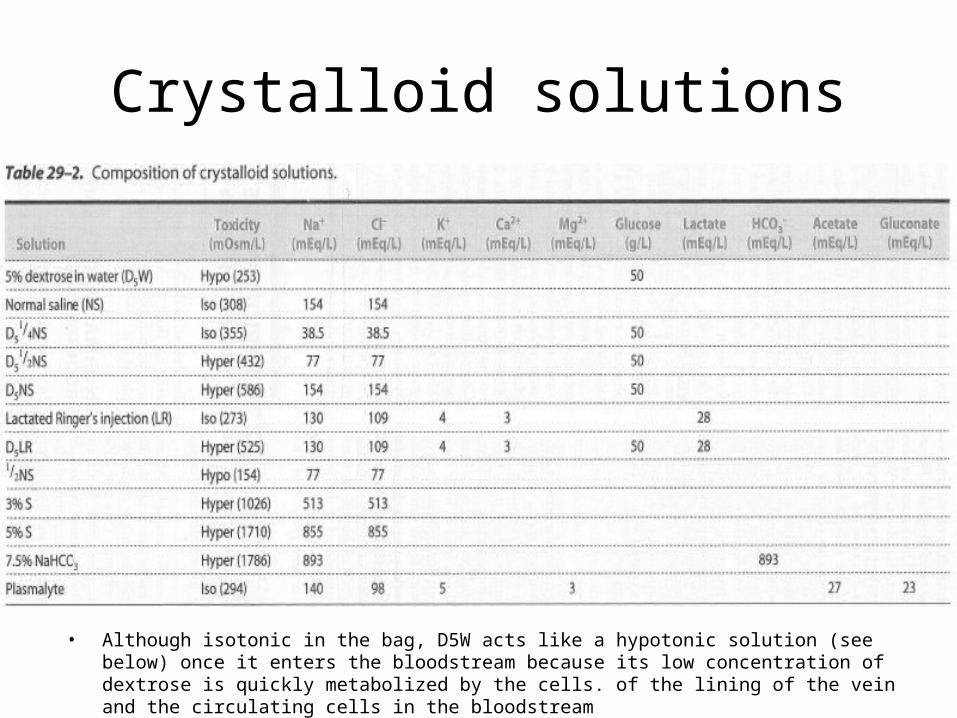
• Although isotonic in the bag, D5W acts like a hypotonic solution (see below) once it enters the bloodstream because its low concentration of dextrose is quickly metabolized by the cells. of the lining of the vein and the circulating cells in the bloodstream

Water physiology
• In a 70-kg man, total-body water is about 600 mL/kg.– The intracellular fluid volume averages 400 to 450 mL/kg – The extracellular fluid (ECF) volume averages 150 to 200 mL/kg
• The plasma volume (30 to 35 mL/kg)• The interstitial fluid (120 to 165 mL/kg)
– Miller’s Anesthesia 7th edition Ch.54
Intracellular Extracellular Interstitial Plasma

Choice of fluid
• Crystalloid: aqueous solutions of low-molecular-weight ions with intravascular half life of 20-30min.– Isotonic – Hypertonic
• Colloid: contain high-molecular-weight substances such as proteins or large glucose polymers.– Albumin– Gelatin – Hydroxyethyl starch

Hypertonic saline
• Osmotic pressure forces the water from the intracellular space into the extracellular space and decrease the total volume required for satisfactory resuscitation. – Traumatic brain injury– During mass casualties as seen in natural or man-made disasters.
• ease of storage• low cost• ability to rapidly expand plasma volume.• Short duration

Isotonic crystalloid
• Ringer’s solution (balance salt) versus normal saline– There is no guideline or consensus regarding the choice of intravenous
fluid for administration during major surgery.– When given in large volumes, normal saline (pH=6.0) produces a
dilutional hyperchloremic acidosis.– There is a growing body of evidence suggesting that renal function is
adversely affected by normal saline.
Crystalloid versus colloid
• Much controversy exists about the role of crystalloids and colloids in fluid therapy.– Kidney injury and coagulopathy
• Dose limit?• Monitoring of hemostasis?
– Most of the mainstream burn formulas add colloid during the resuscitation, at least in the second 24-hour period.
– 5% albumin use increases mortality among traumatic brain injury patients in SAFE trial.• SAFE (Saline versus Albumin Fluid Evaluation) trial: no difference in 28-day
mortality for critically ill patients resuscitated with albumin versus saline.
Traumatic brain injury guideline
How
Goal-directed

Perioperative fluid management
• Previous concept of assumed perioperative fluid management: insensible perspiration + third space loss + NPO (fasting and operative period) fluid loss
Perioperative fluid management
• Truth:– Blood volume after fasting is normal
• The extracellular deficit after usual fasting is low– Fluid-consuming third space has never been reliably shown
• The basal fluid loss via insensible perspiration is approximately 0.5-1 ml/kg/h during major abdominal surgery
• Avoid over-hydration and keep an adequate fluid replacement improve outcome.
Fluid (volume) responsiveness• Volume responsive – respond to fluid administration by
increasing C.O.– e.g. C.I. 15%

CVP and PCWP are not appropriate predictor of volume responsiveness
• Osman et al. (Crit Care Med 2007)– 96 severe septic or septic shock patients monitored with PA catheter
and mechanically ventilated in MICU– 150 volume challenges (500 ml of 6% hydroxyethyl starch infusion for
20 min)– Fluid responsiveness: increase in C.I. induced by the volume challenge
of 15% as responder– In septic patients receiving mechanical ventilation, cardiac filling
pressures (PCWP & CVP) afford a poor prediction of fluid responsiveness
Flow based parameter
• Stroke volume variation (under positive pressure ventilation)– PICCO– LidCO– Flotrac
• Pulse pressure variation• Pleth variability index (PVI)
– Derived from pulse oximetry
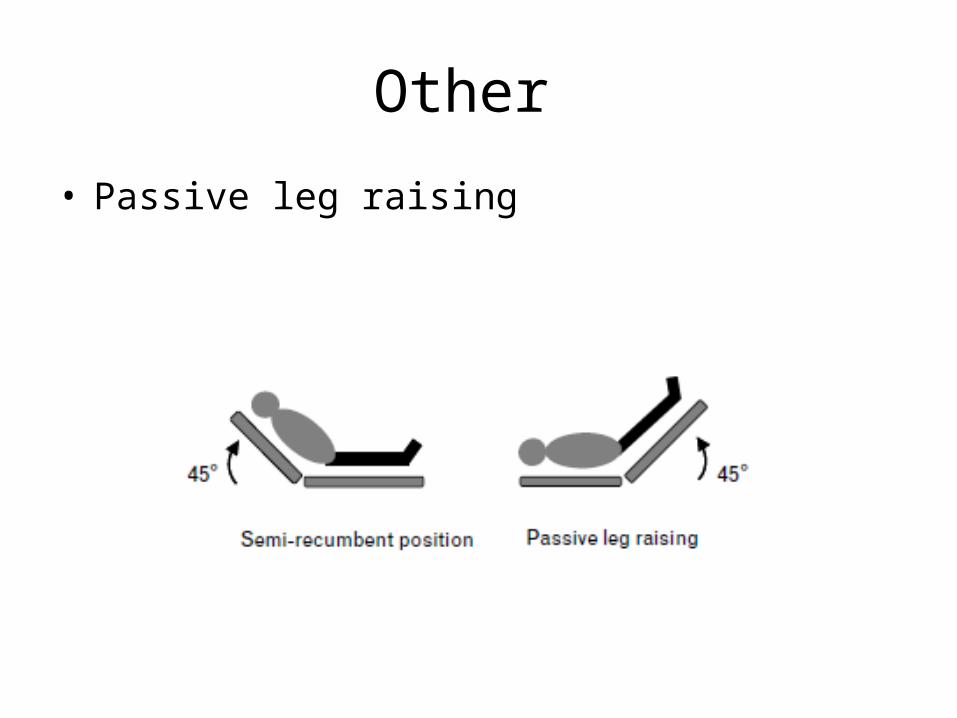
Other
• Passive leg raising
Perfusion pressure ?

Perfusion pressure
• Cerebral perfusion pressure (CPP)– MAP – ICP (jugular venous pressure or CVP)
• Coronary perfusion pressure (CPP)– Right CPP = Aortic diastolic pressure – right atrial diastolic pressure
( DABP – CVP)– Left CPP = Aortic diastolic pressure – left atrial diastolic pressure
( DABP – PCWP)
• Abdominal perfusion pressure (APP)– MAP – IAP (intra-abdominal pressure)

Suggested optimal perfusion pressure
• Maintaining CPP (cerebral) 60-70 mmHg (in traumatic
brain injury patients)
• Maintaining APP 60 mmHg
Goal-directed hemodynamic management
Beneficial effect of hemodynamic optimization
Decrease the postoperative infection• Systemic review and meta-analysis: 26 randomized, controlled
trials with a total of 4188 surgical patients (Dalfino et al., Crit Care 2011)
• Significant reduction in surgical site infection, pneumonia, urinary tract infection, and total infectious episodes
• Flow-directed hemodyanamic therapy to optimize O2 delivery protects surgical patients against postoperative hospital-acquired infections
• Strategies to prevent infection in surgical patients:– Strict asepsis– Antibiotic prophylaxis– Avoidance of glucose imbalance– Normothermia– Flow-directed hemodynamic therapy to optimize O2 delivery
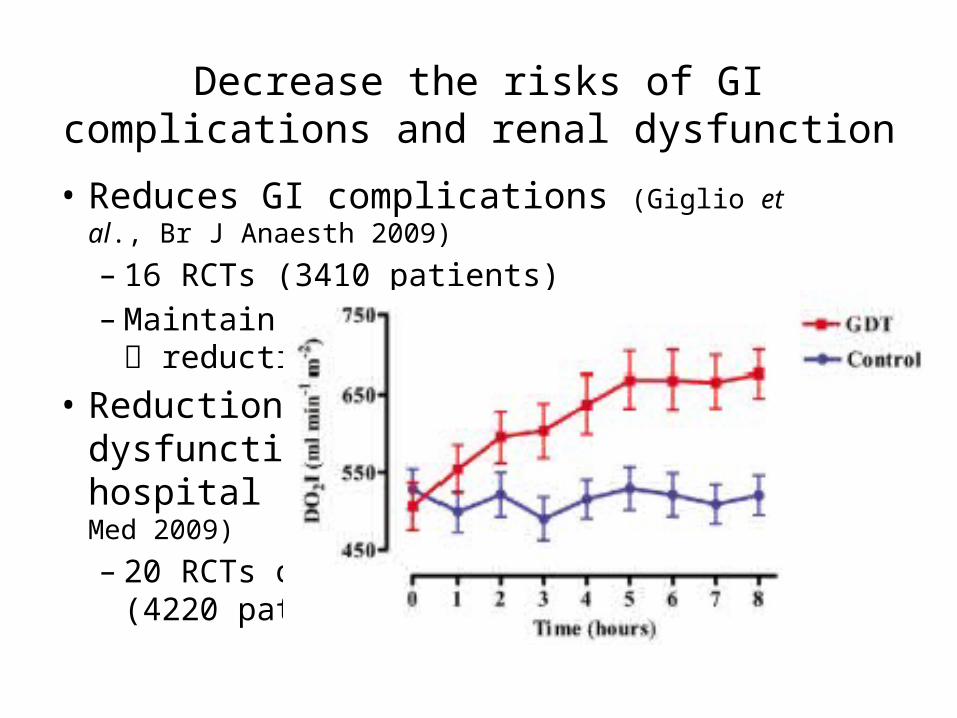
Decrease the risks of GI complications and renal dysfunction
• Reduces GI complications (Giglio et al., Br J Anaesth 2009)
– 16 RCTs (3410 patients) – Maintain adequate tissue oxygenation
reduction in GI complications• Reduction in complicaitons, renal
dysfunction and duration of hospital stay (Brienza et al., Crit Care Med 2009)
– 20 RCTs on goal-directed therapy (4220 patients)
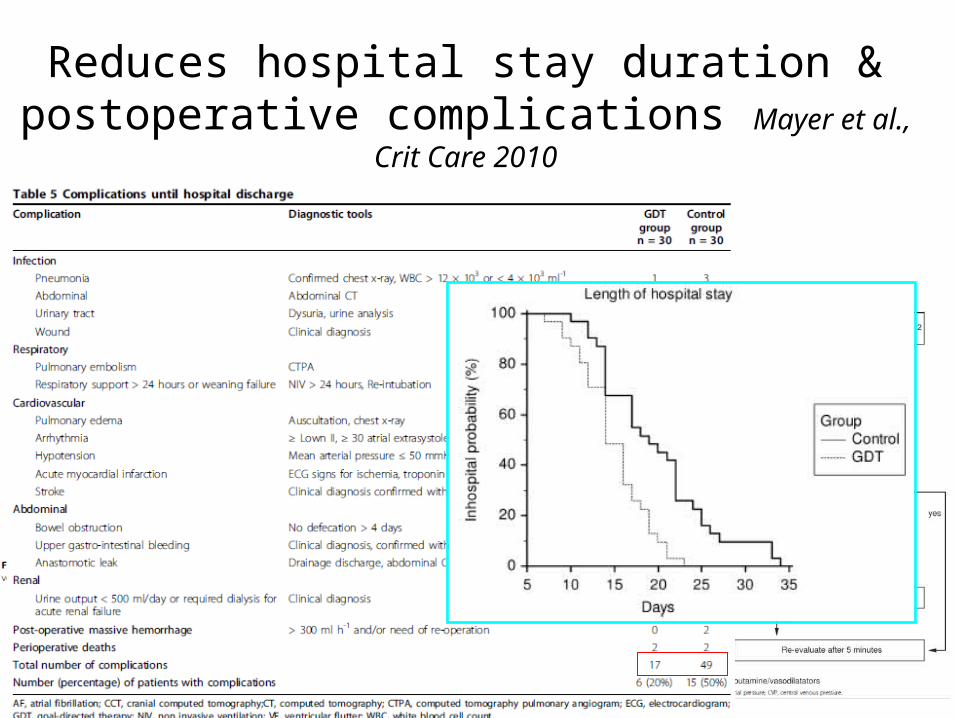
Reduces hospital stay duration & postoperative complications Mayer et al., Crit Care 2010

Goal-directed hemodynamic management
Some protocols
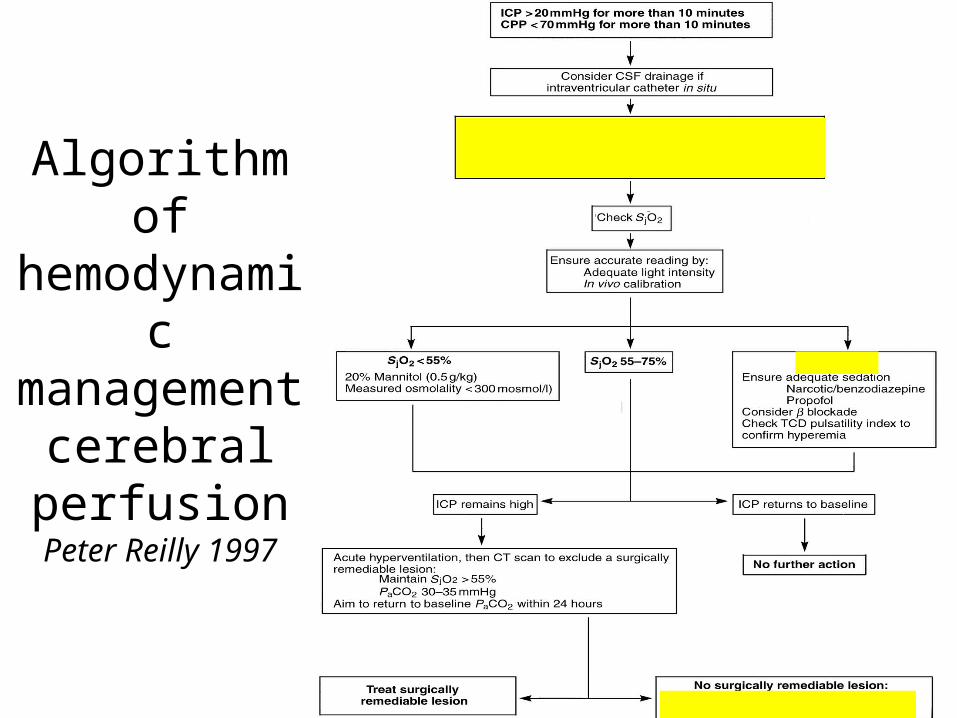
Algorithm of hemodynamic management
cerebral perfusion
Peter Reilly 1997
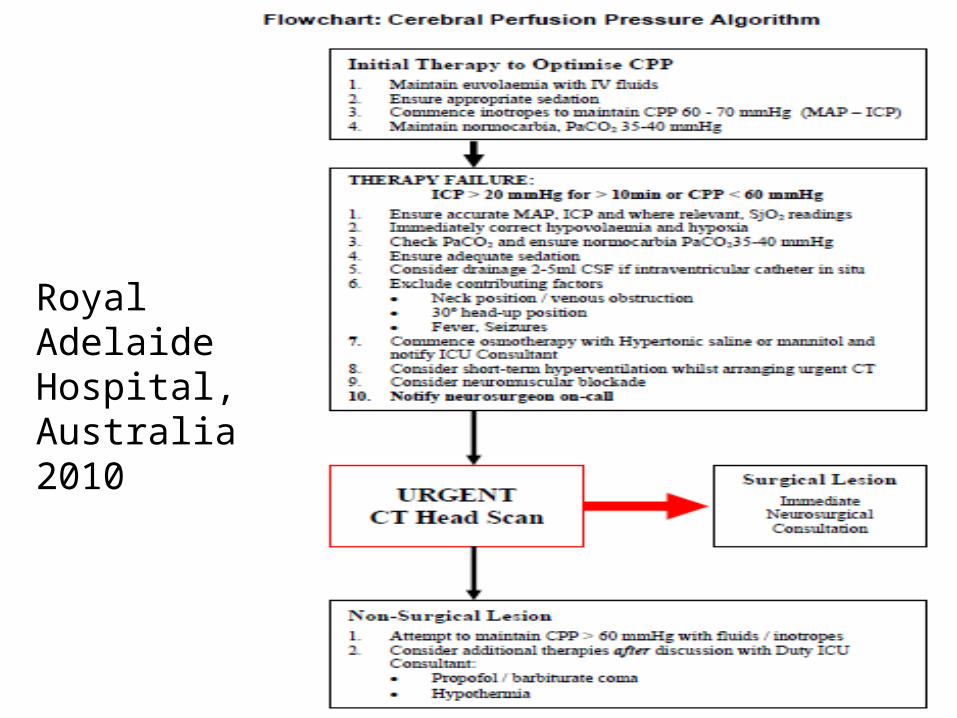
Royal Adelaide Hospital, Australia 2010
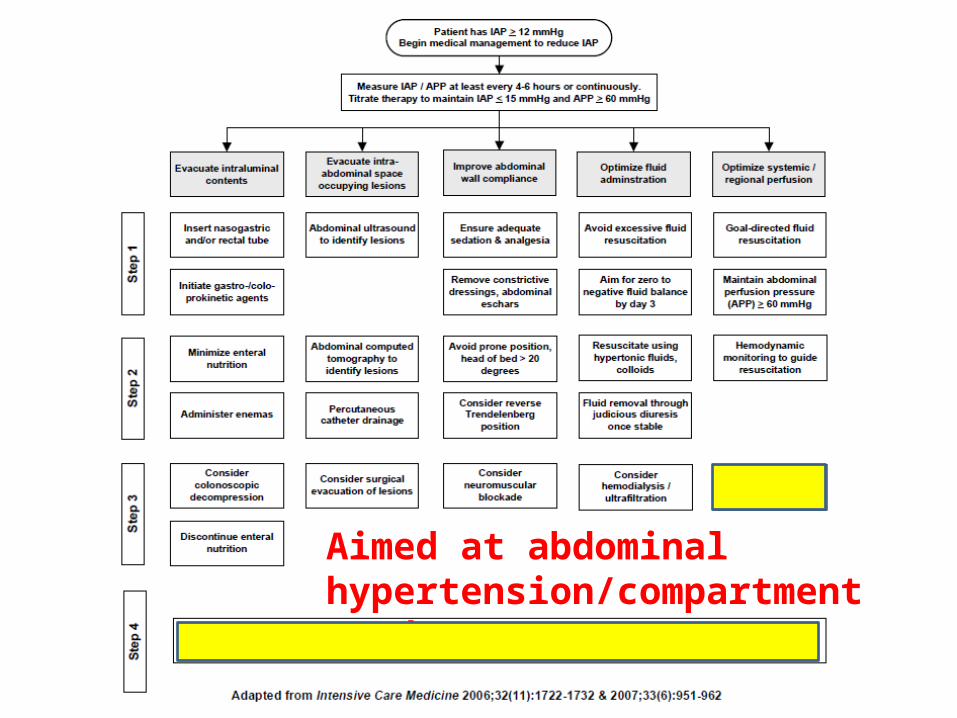
Aimed at abdominal hypertension/compartment syndrome

Summary
• Maintain adequate blood volume hemodynamic stability: avoid hypovolemia & hypoperfusion
• Improve tissue oxygenation: optimize oxidative killing ability of neutrophils, tissue repair, and wound healing
• Flow-directed hemodynamic therapy aims at optimizing perioperative tissue oxygenation

Massive transfusion
When should we use FFP
When to alarm
• Adult patients requiring > 4 units of PRBCs in first hour of resuscitation or. pediatric patient requiring > 20 ml/kg of PRBCs in first hour of resuscitation.
• Adult patients with the high likelihood of requiring transfusion of > 10 units of PRBCs within the first 12 hours of resuscitation or pediatric patient with the high likelihood of requiring transfusion of > 0.1 units/kg of PRBCs within the first 12 hours of resuscitation.– Stanford Medical center since 2005/Apr
The role of FFP
• The optimal replacement ratio (FFP:PRBC)– 1:1, patients related to combat-associated trauma
• requiring >10 units packed red blood cells (RBC) per 24 hours.– 2:3, derived from computor model
• Data from trauma center in Huston.• The standard massive transfusion pack suggested by Stanford Medical
Center: 4 units FFP ; 6 units PRBC ; 1 unit platelet pheresis– 1:2, Denver Health Medical Center
• Data from single trauma center
Right thing, right now.
• Point-of-care– Thromboelastography
Thanks for your attention