perioperative management of atrial fibrillation r1 劉志中 anaesthesia,1998,53,pages 665- 676
TRANSCRIPT
Perioperative management of atrial fibrillation
R1 劉志中
Anaesthesia ,1998,53,pages 665-676
Prevalence
0.4% in adult less than 60 years old
12% in those over 75 years
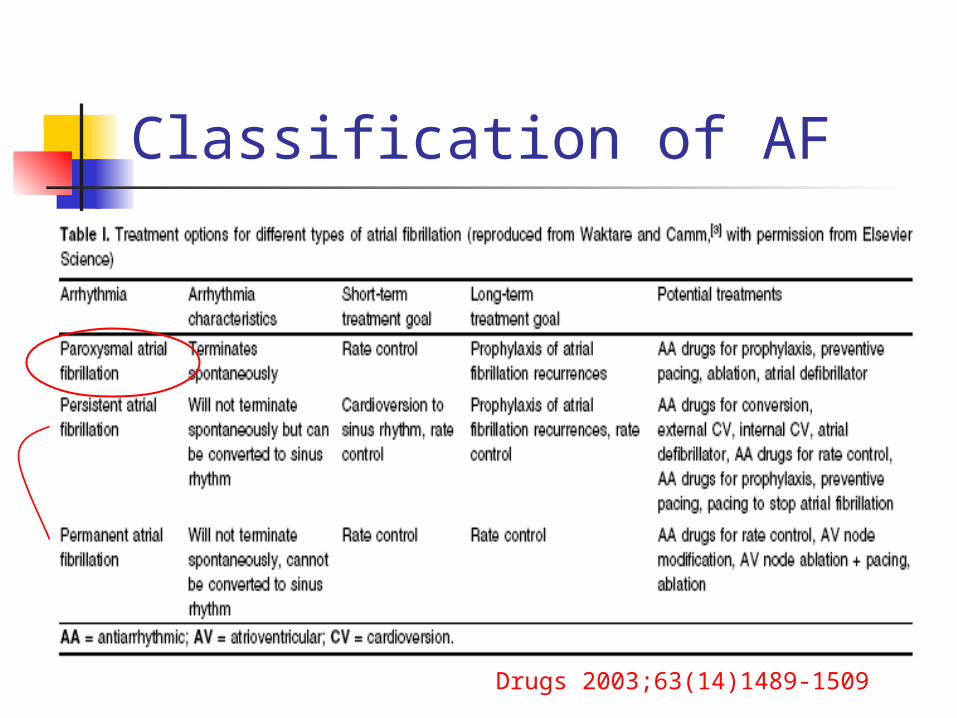
Classification of AF
Drugs 2003;63(14)1489-1509
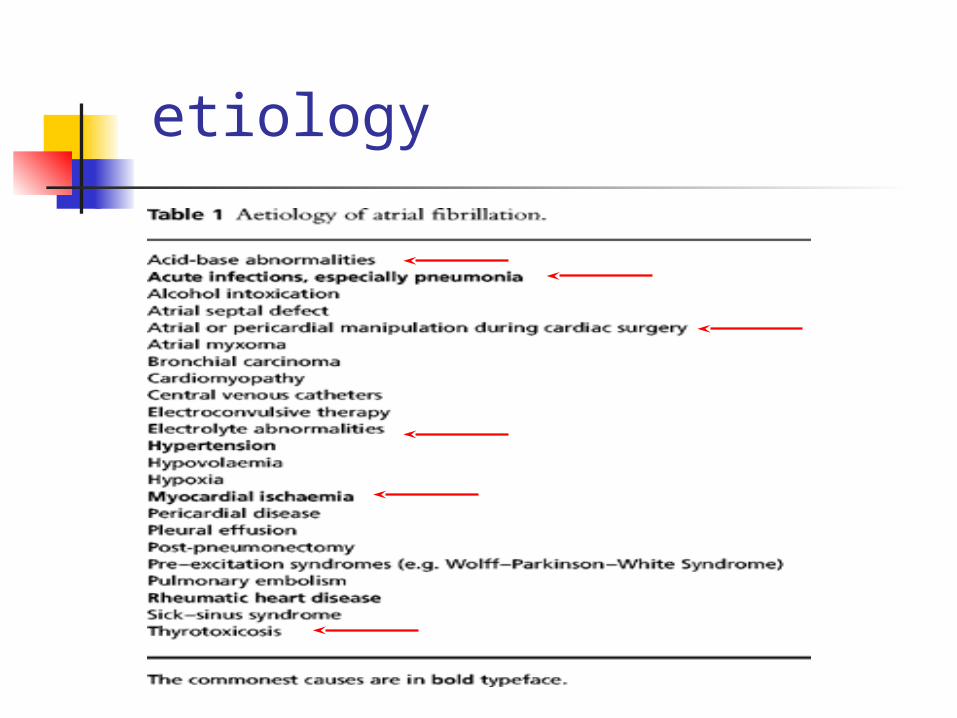
etiology
Volatile anesthetic agent
Sensitizing the myocardium to catecholamine
Have an apparent antifibrillary effect in the ventricle following periods of ischemia and reperfusion similar to CCB like verapamil.
Depression of sinus node automaticity, increased supraventricular refractoriness and depressed AV nodal conduction

Clinical consequence
Loss of “atrial kick” Excessively rapid and irregular ventric
ular rate Systemic thrombo-embolism and a si
gnificant risk of stroke Patient discomfort due to palpitation
Loss of “atrial kick” Absent (atrial fibrillation) , ineffective
(atrial flutter) ,or altered timing of atrial contraction (low atrial or junctional rhythm) can reduce ventricular filling by 20-30%
LV dysfunction more depend on atrial kick
Excessively rapid and irregular ventricular rate Ventricular filling progressively beco
mes impaired at high heart rate (>120 beats/min in adult ).
Tachycardiomyopathy Tachycardia-induced LV dysfunction
due to high ventricular rate (>120 bpm) which is reversible with rate or rhythm control
LV dysfunction secondary to chronic tachycardia
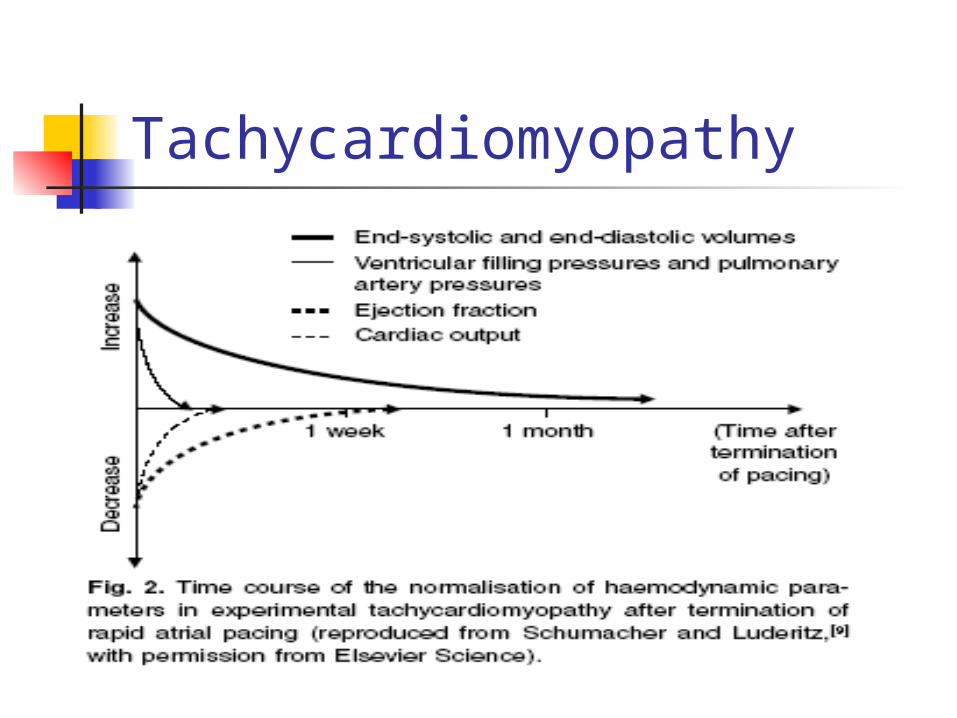
Tachycardiomyopathy
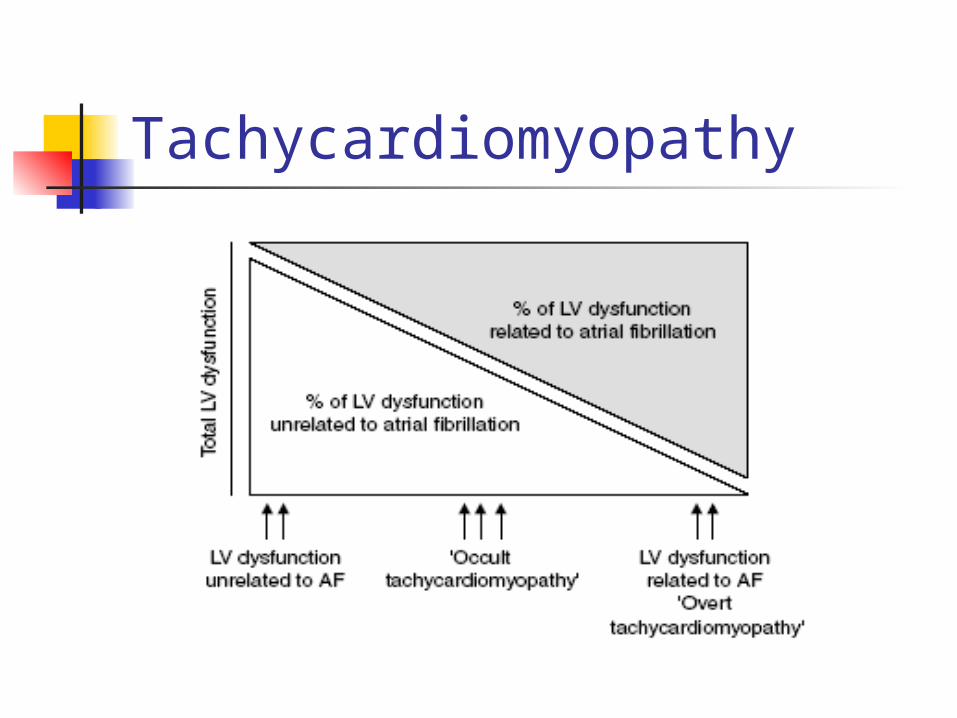
Tachycardiomyopathy
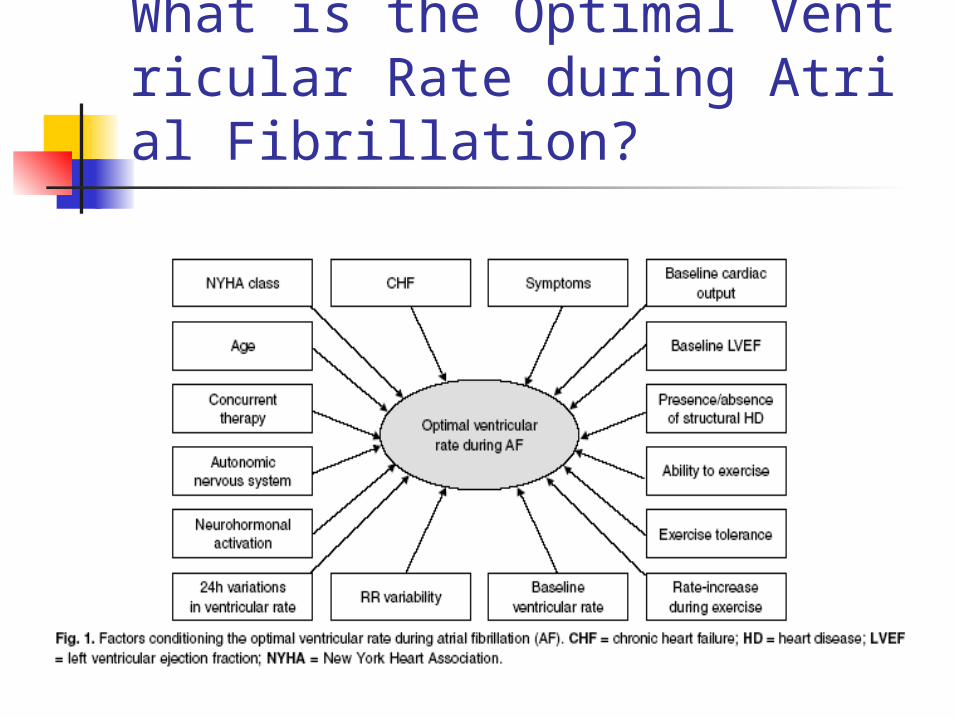
What is the Optimal Ventricular Rate during Atrial Fibrillation?
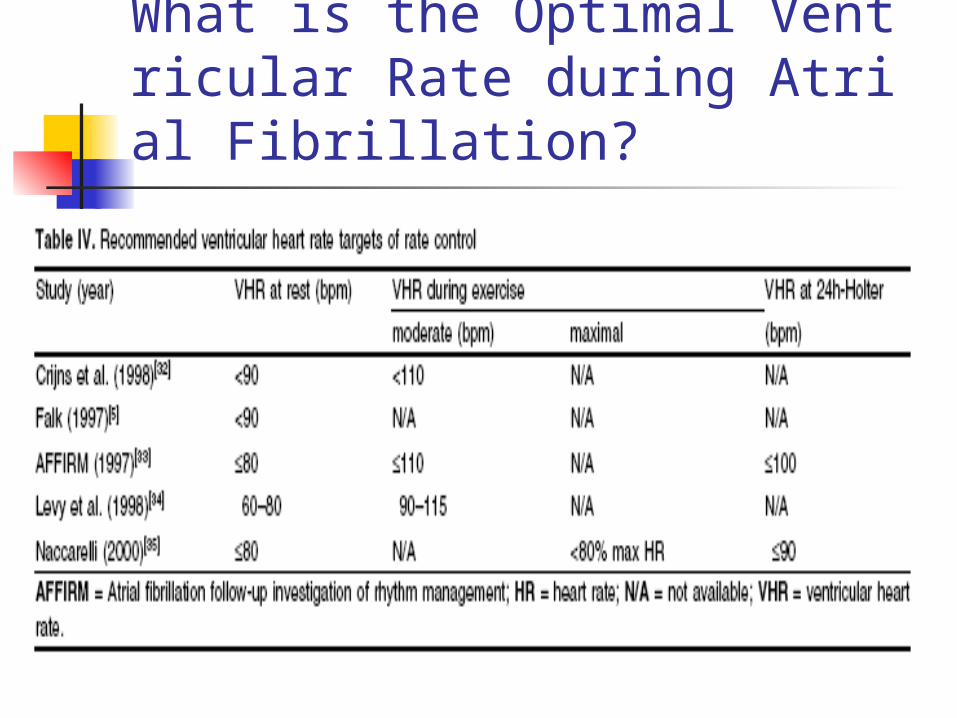
What is the Optimal Ventricular Rate during Atrial Fibrillation?
Current recommandation for the targets of rate control ≦80-90 bpm at rests ≦110-115 bpm during moderate exer
cise
Management strategies
Management of acute-onset AF Maitenance of sinus rhythm Control of ventricular rate Prevention of thromboembolism
Management of acute-onset AF ~ cardiversion ~ DC cardioversion: 1.Indication : AF associated with hypotensio
n, CHF, active ischemia or acute infarction. Patients with severe AS,MS,and hypertrophic cardiomyopathy
2.contraindication: digoxin toxicity, a history of bradycardia or
sick sinus syndrome,and inadequated correct precipitating factors.
Duration of AF>48 hrs without >3 weeks anticoagulation or exclude the atrial thrombus by TEE
Do Not DC cardioversion!!!
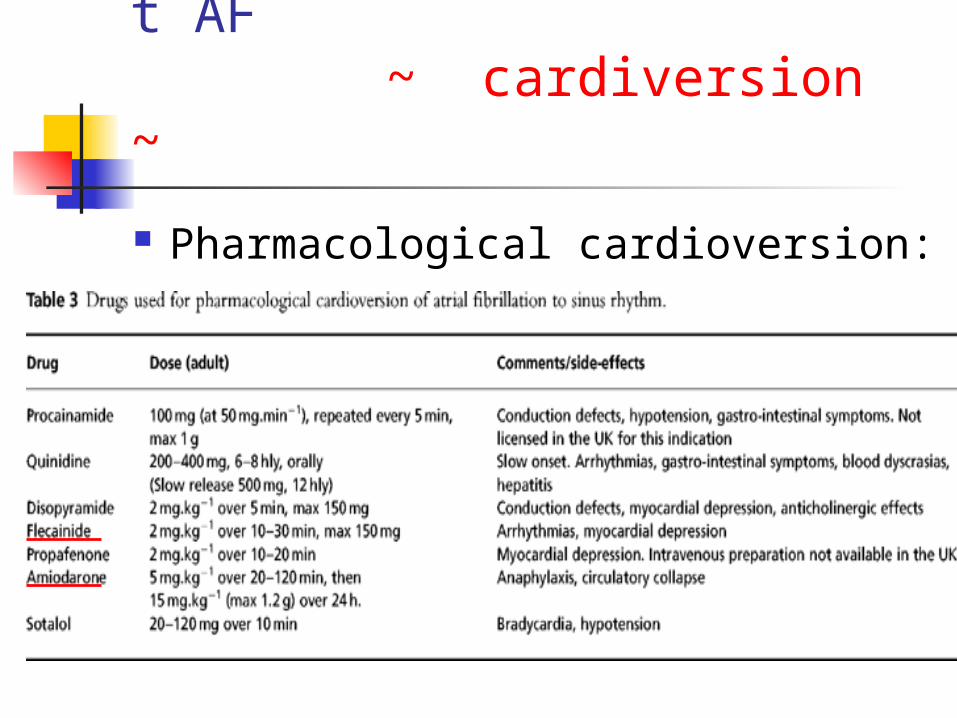
Management of acute-onset AF ~ cardiversion ~ Pharmacological cardioversion:
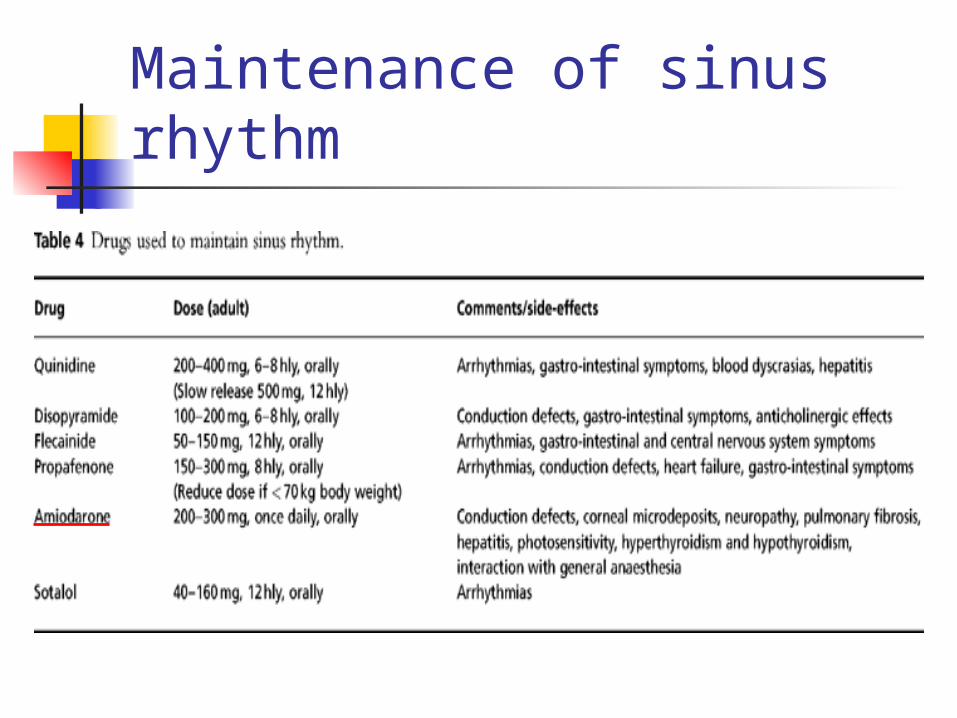
Maintenance of sinus rhythm
Rate control vs. Rhythm control
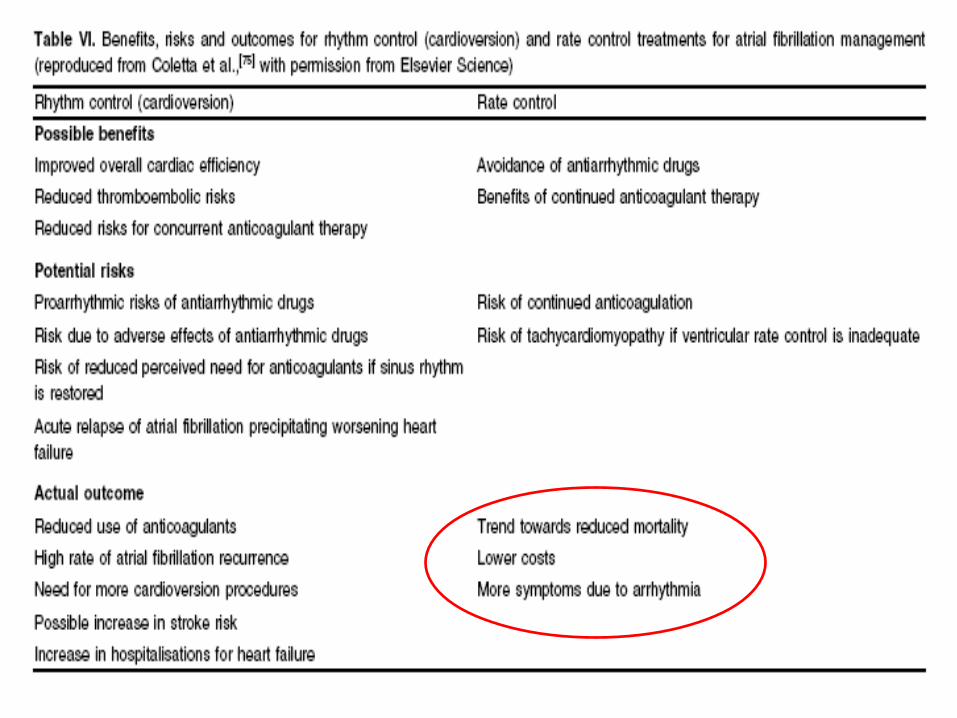
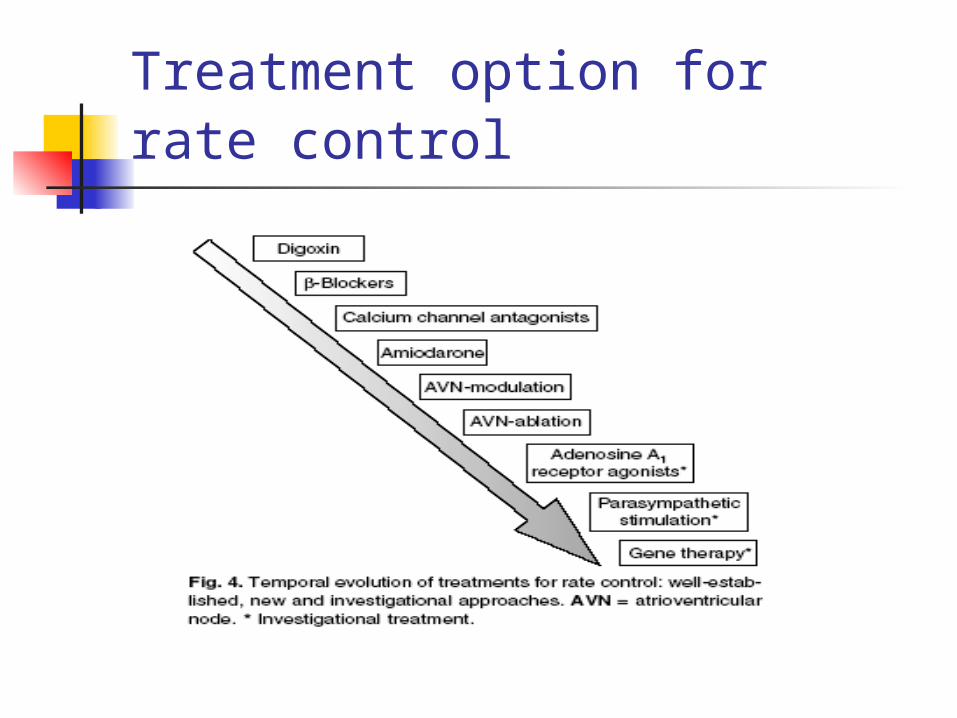
Treatment option for rate control
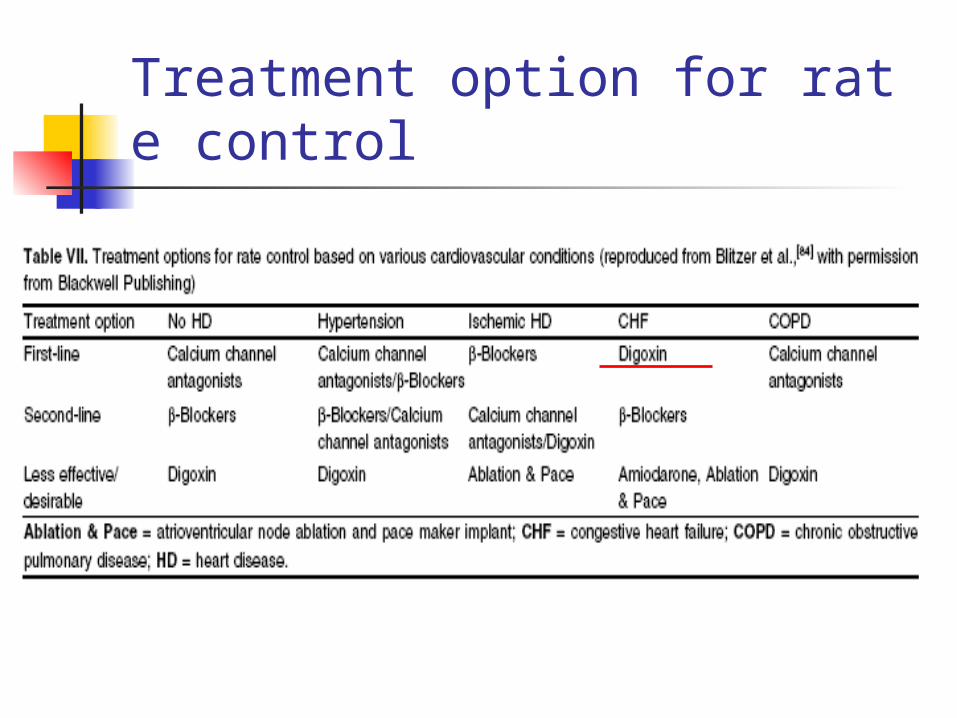
Treatment option for rate control
Further investigation of AF Full history and examination 12 lead ECG (including and ECG during periods
of sinus rhythm if AF is paroxysmal in order to detect intra-atrial conduction defect)
Echocardiography(Dx of impaired LV function) Serum chemistry screen including thyroid fun
ction test Exercise ECG if arrythmia is exercise-induced. Electrophysiological studies in p’t who are y
oung or refractory to treatment.