赖蒽茵 浙江大学医学院生理系 求是特聘教授 浙江省“千人计划”人才,...
DESCRIPTION
Respiratory Physiology ( 呼吸生理学). 赖蒽茵 浙江大学医学院生理系 求是特聘教授 浙江省“千人计划”人才, 博导 [email protected]. May 26 and 27, 8:00 – 9:35 am, 基础医学各论 I 紫金港校区西 2-303 , 2012 级五年制临床 , 共 162 人. Respiratory. Exchange of oxygen (O2) and carbon dioxide (CO2) with environment. Pulmonary ventilation. - PowerPoint PPT PresentationTRANSCRIPT
赖蒽茵
浙江大学医学院生理系 求是特聘教授 浙江省“千人计划”人才,博导
May 26 and 27, 8:00 – 9:35 am, 基础医学各论 I紫金港校区西 2-303, 2012 级五年制临床 , 共 162 人
Respiratory Physiology(呼吸生理学)

Exchange of oxygen (O2) and carbon dioxide (CO2) with environment
Respiratory

气体经呼吸道进出肺的过程The process of moving air into and out of the lungs
Pulmonary ventilation

呼吸过程中肺内压的变化
吸气时,肺内压为 -2 to -1mmHg
尽力吸气时 (-100 to -30mmHg)
呼气时,肺内压为 1 to 2 mmHg
尽力呼气时 ( 60 to 140mmHg )
Pulmonary ventilation
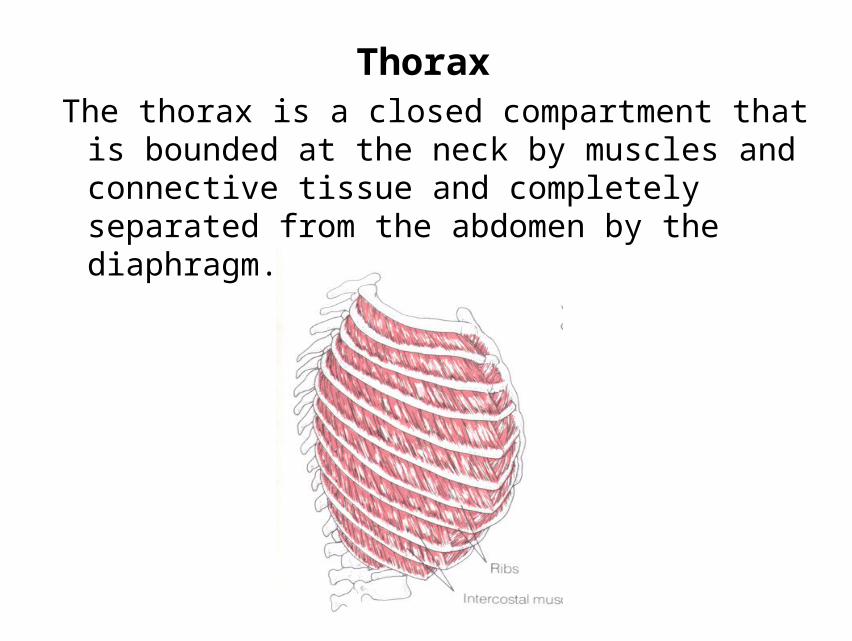
ThoraxThe thorax is a closed compartment that is bounded at the
neck by muscles and connective tissue and completely separated from the abdomen by the diaphragm.

Mechanics of pulmonary ventilation
Muscles that cause lung expansion and contraction
吸气肌: diaphragm ( 膈肌 )
external intercostals ( 肋间外肌 )
呼气肌: abdominal muscles ( 腹肌 )
internal intercostals ( 肋间内肌 )

Structures of pulmonary ventilation

Breathing is an active processTo inhale• Contraction of external intercostal muscles
→elevation of ribs & sternum →increased front-to-back dimension of thoracic cavity →lowers air pressure in lungs →air moves into lungs
• Contraction of diaphragm →diaphragm moves downward →increases vertical dimension of thoracic cavity →lowers air pressure in lungs →air moves into lungs

•To exhale
Relaxation of external intercostal muscles & diaphragm →return of diaphragm, ribs, & sternum ( 胸骨 ) to resting position →restores thoracic cavity to pre-inspiratory volume →increases pressure in lungs →air is exhaled


Pattern of respiration
•Abdominal breathing 腹式呼吸
•Thoracic breathing 胸式呼吸
•Eupnea 平静呼吸
•Forced breathing 用力呼吸

Principles of pulmonary ventilation
• Direct force of breathing
– Pressure gradient between atmosphere and lung
• Original force of breathing
– Respiratory movement

Respiration
A processes involved in exchange of oxygen (O2) and
carbon dioxide (CO2) between an organism and the
environment
•Consist of
– Inspiration: the inhalation of air into the lung
– Expiration: breathing out
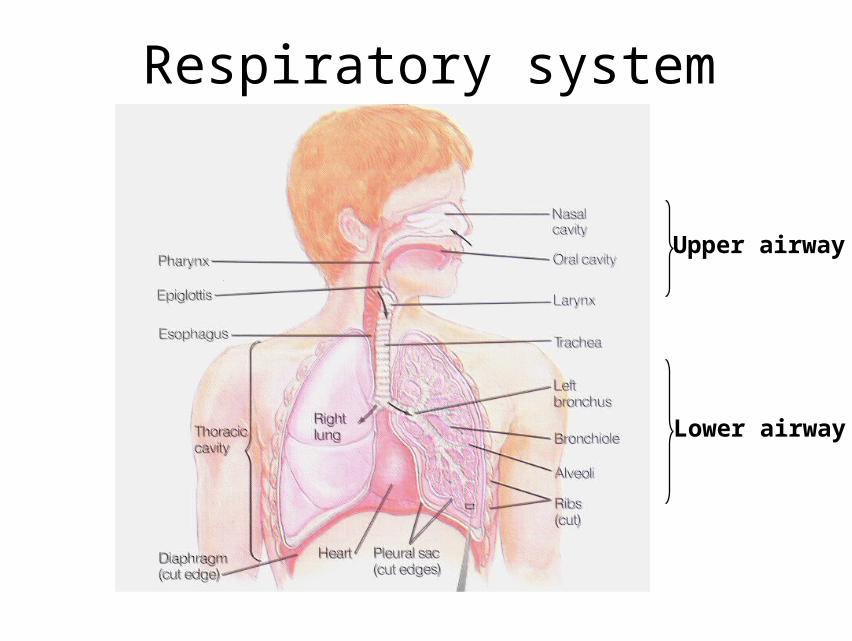
Respiratory system
Upper airway
Lower airway

The relaxation/contractionof circular smooth musclelining these “airways’” determines how easily airflow can occur.
Most gas exchange occurs in thealveolar sacs.

Four major steps of respiration
• 1.Pulmonary ventilation
• 2.Gas exchange
– Lung
– Tissue
• 3.Gas transport in blood
• 4.Cellular respiration

Respiratory process
}外呼吸 External respiration
气体在血液中的运输Gas transport in the blood
}内呼吸 Internal respiration
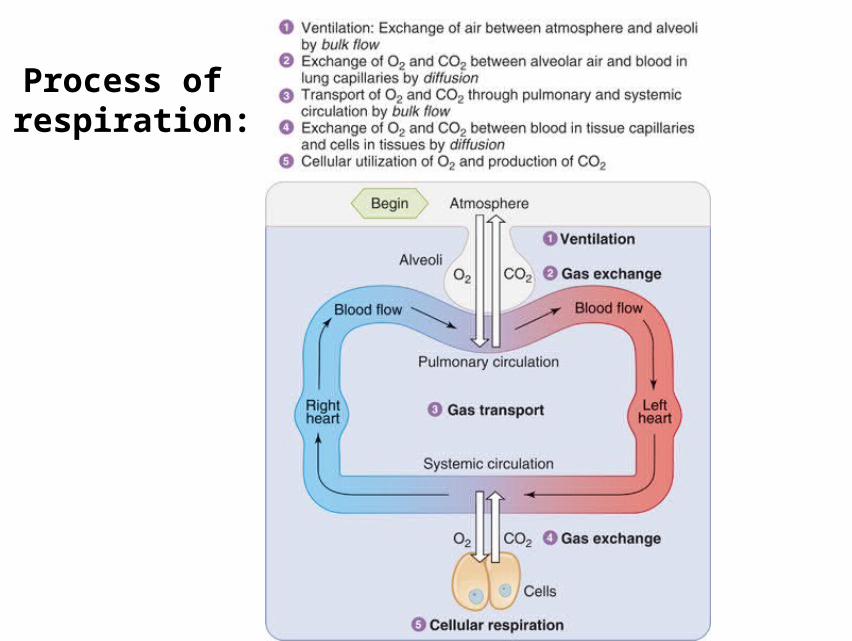
Fig. 13.06Process of respiration:

Gas exchange
Pulmonary gas exchange Tissue gas exchange
Tissue capillaries
Tissue cellsCO2
CO2O2
O2
Pulmonary capillaryCO2
CO2O2
O2

Principles of gas exchange
• Diffusion: continuous random motion of gas molecules.
• Partial pressure: the individual pressure of each gas, eg. PO2

Boyle’s law states that the pressure of a fixednumber of gas molecules is inversely proportional to the volume of the container.

Laws governing gas diffusion
• Henry’s law:
The amount of dissolved gas is directly proportional to the partial pressure of the gas

Factors affecting gas exchange
MWd
ATSPD
• D: Rate of gas diffusion
P: Difference of partial pressure• S: Solubility of the gas • T: Absolute temperature• A: Area of diffusion• d: Distance of diffusion• MW: Molecular weight

Gas partial pressure (mmHg)
Atmosphere Alveoli Arterial Venous
Tissue
Po2 159 104 100 40 30
Pco2 0.3 40 40 46 50
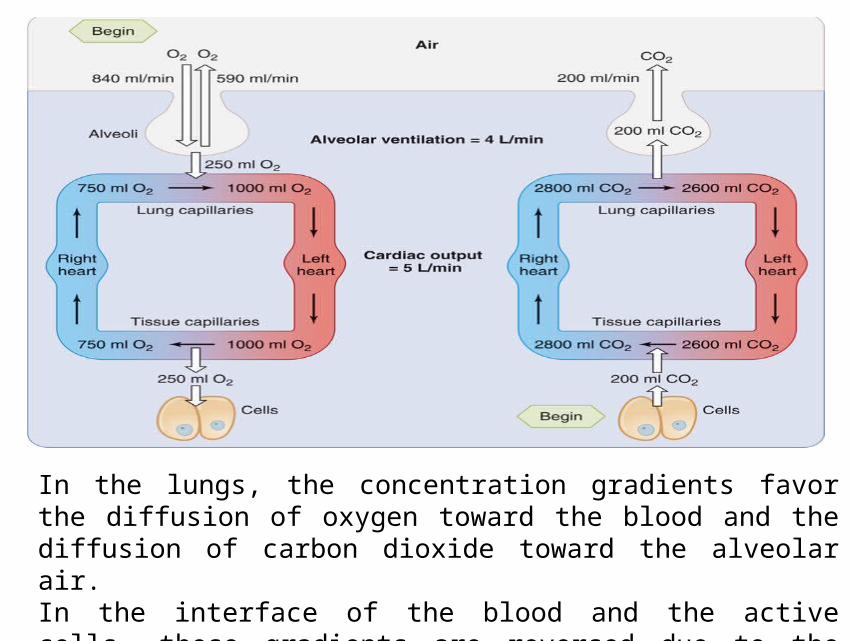
In the lungs, the concentration gradients favor the diffusion of oxygen toward the blood and the diffusion of carbon dioxide toward the alveolar air.In the interface of the blood and the active cells, these gradients are reversed due to the metabolic activities of cells.

Pulmonary gas exchange factors
• Thickness of respiratory membrane ( 呼吸膜 )
• Surface area of respiratory membrane
• The diffusion coefficient of gas ( 扩散系数 )
• The pressure difference of gas between the two sides of membrane

AlveoliEach of the clustered
alveoli includes an abundance of pulmonary capillaries, thereby assuring that the ventilated air is brought into close proximity to the “pulmonary” blood, allowing efficient and thorough gas exchange between the air and the blood.

Extensive branchingof alveoli produceslots of surface area for exchange between air and blood.
Alveolar and capillary walls are thin, permitting rapid diffusion of gases.

Respiratory membrane• Is the structure through which oxygen diffuse from the
alveolus into the blood, and carbon dioxide in the opposite direction.
surfactant
epithelial cell
interstitial space
alveolus capillary
red blood cell
endothelial cell
O2O2
CO2CO2

Gas transport in the blood• Respiratory gases are transported in the blood in two
forms:– Physical dissolution
– Chemical combination
Alveoli Alveoli BloodBlood Tissue Tissue
O2 →dissolve→combine→dissolve→ O2O2 →dissolve→combine→dissolve→ O2
CO2 ←dissolve←combine←dissolve← CO2CO2 ←dissolve←combine←dissolve← CO2


Transport of oxygen
• Forms of oxygen transported
– Chemical combination: 98.5%
– Physical dissolution: 1.5%
• Hemoglobin ( 血红蛋白, Hb) is essential for the
transport of O2 by blood. (porphyrin molecules, 卟啉分子 )

• Normal adult hemoglobin is composed of four subunits linked together, with each subunit containing a single heme -- the ring-like structure with a central iron atom that binds to an oxygen atom.

Hb + O2 HbO2
High PO2
Low PO2

• Oxygen capacity 氧容量– The maximal capacity of Hb to bind O2 in a blood
sample
• Oxygen content 氧含量– The actual binding amount of O2 with Hb
• Oxygen saturation 氧饱和度– Is expressed as O2 bound to Hb devided by the
maximal capacity of Hb to bind O2
– (O2 content / O2 capacity) x 100%

Hb >50g/L --- Cyanosis 紫绀• is a physical sign causing bluish discoloration of the
skin and mucous membranes.
• is caused by a lack of oxygen in the blood.
• is associated with cold temperatures, heart failure, lung diseases. It is seen in infants at birth as a result of heart defects, respiratory distress syndrome, or lung and breathing problems.
Hb + O2 HbO2

Cyanosis
• Hb >50g/L

Carbon monoxide poisoning • CO competes for the O2 sides in Hb
• CO has extremely high affinity for Hb
• Carboxyhemoglobin---20%-40%, lethal ( 致命的 ).
• A bright or cherry red coloration to the skin

Transport of carbon dioxide
• Forms of carbon dioxide transported
– Chemical combination: 93%
• Bicarbonate ion (HCO3-) : 70%
• Carbamino hemoglobin( 氨基甲酸血红蛋白 ): 23%
– Physical dissolve: 7%

Total blood carbon dioxide
Sum of
• Dissolved carbon dioxide
• Bicarbonate
• carbon dioxide in carbamino hemoglobin

tissue capillaries
tissues CO2 transport in tissue capillaries
CO2 + Hb HbCO2
CO2
plasmaplasmatissue capillaries
CO2 + H2O H2CO3
H+ +HCO3-HCO3HCO3--
carbonic anhydrase
CO2
Cl Cl --

pulmonary capillaries
CO2 + Hb HbCO2
H+ +HCO3-
HCO3HCO3--
H2CO3carbonic anhydraseCO2 + H2O
plasmaplasma
alveoli
Cl-
pulmonary capillaries
CO2 transport in pulmonary capillaries
CO2CO2
CO2
Cl-Cl-


Airflow (F) is a function of the pressure differences between the alveoli (Palv) and the atmosphere (Patm) divided by airflow resistance (R).
Air enters the lungs when Palv < Patm
Air exits the lungs when Palv > Patm
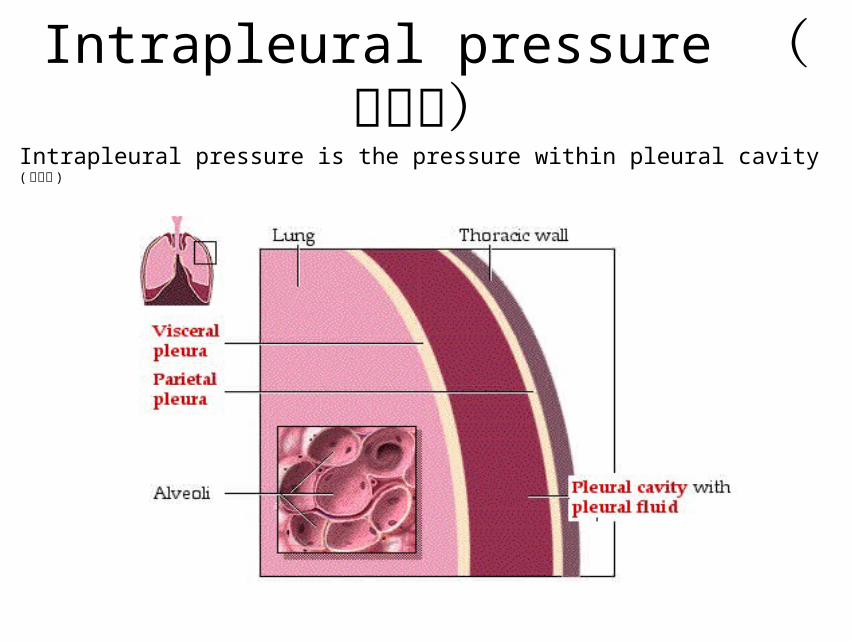
Intrapleural pressure (胸内压)Intrapleural pressure is the pressure within pleural cavity ( 胸膜腔 )

Intrapleural pressure
• Pleural cavity– Pleural cavity is the closed space between parietal
pleura & lungs covered with visceral pleura

Intrapleural pressure
the pressure within pleural cavity

Direct measurement of intrapleural pressure

Indirect measurement of intrapleural pressure
Measurement of the
pressure inside the
esophagus


Formation of intrapleural pressure
•Fetus lung
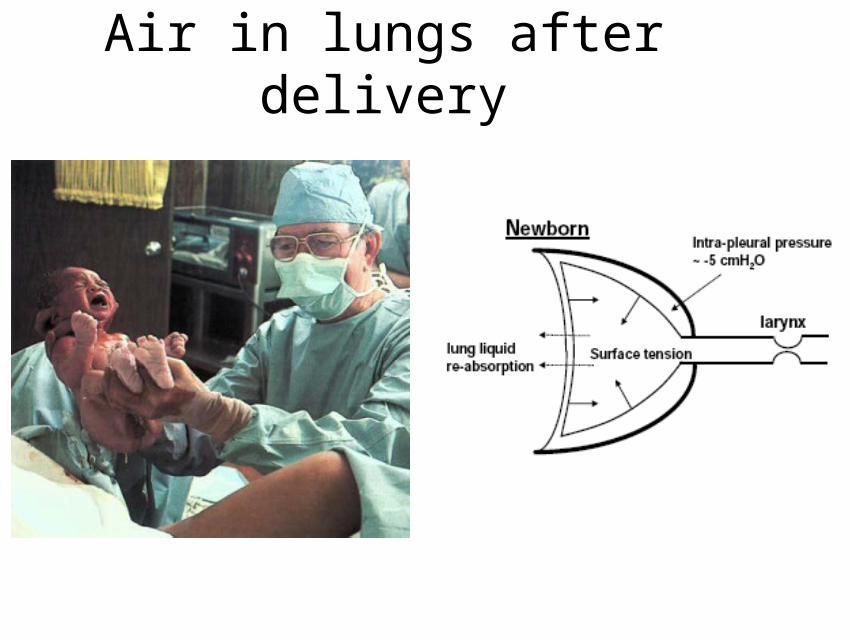
Air in lungs after delivery
Formation of intrapleural pressure
• Air in lungs after delivery
• Because the elastic recoil ( 弹性回缩 ) causes the lungs to try to collapse, a negative force is always needed to the outside of the lungs to keep the lungs expanded. This force is provided by negative pressure in the normal pleural space.

Intrapleural pressure• Intrapleural pressure = Intrapulmonary pressure –
the recoil pressure of the lung
• Intrapleural pressure = – the recoil pressure of the
lung

Pressures involved - intrapulmonary pressure = atmospheric pressure (760 mmHg) - collapsing force of lung ( 肺回缩力 ) - intrapleural pressure
Physiological significance of intrapleural negative pressure ( 胸膜腔负压 )
•Allow expansion of the lungs ( 利于肺的扩张 )
• Facilitate the venous & lymphatic return ( 促进静脉血和淋巴液的回流 )

Pneumothorax ( 气胸 )
Air escapes from the lungs or leaks through the chest wall and enters the pleural cavity

Lateral 单侧 Bilateral 双侧



Compliance of the lungs ( 肺的顺应性 )
•The extent to which the lungs expand for each unit increase in pressure C=ΔV/ΔP (L/cmH2O)
•Determined by the elastic forces of the lungs (R, 肺弹性阻力 ) C=1/R

Compliance of the lungs
• Compliance ( 顺应性 ): the expand ability of
elastic tissues when acted on by foreign forces or
the extent to which the lungs expand for each unit
increase in pressure.
• C=ΔV/ΔP (L/cmH2O)
• Elastic Resistance (R) C=1/R

Compliance (顺应性) varies within the lung according to the degree of inflation. Poor compliance is seen at low volumes (because of difficulty with initial lung inflation) and at high volumes (because of the limit of chest wall expansion), with best compliance in the mid-expansion range.

Resistances to Ventilation
• Elastic resistance: The ability of an elastic structure to
resist stretching or distortion. 70%
• Non-elastic resistance: 30%
气道阻力咽喉 + 直径 > 2mm 气道 的气道阻力 = 80%
直径 < 2mm 气道 的气道阻力 = 20%

Lung compliance is ameasure of the lung’s “stretchability.”
When compliance is abnormally high, the lungs might fail to hold themselves open, and are prone to collapse.
When compliance is abnormally low, the work of breathing is increased.
肺气肿
肺纤维化

Elastic forces of the lungs
• 1/3 Elastic forces of the lung tissue itself (肺组织本身的弹性回缩力)
• 2/3 Elastic forces caused by surface tension ( 表面张力 )
of the fluid that lines the inside walls of the alveoli

Surface tension
• Elastic-like force existing in the surface of a liquid, tending to minimize the area of surface
• Caused by asymmetries ( 不对称 ) in the intermolecular forces between surface molecules

Surface tension
• The surface tension at the air-water interfaces within the alveoli.
• At an air-water interface, the attractive forces between the water molecules (surface tension) make the alveoli like stretched balloons that constantly try to shrink and resist further stretching.

Pierre Simon Laplace(1749 -1827) Laplace’s law: P=2T/r
P= 肺泡內压力 , T= 表面张力 , r= 肺泡半径

Laplace’s law: P=2T/r
In the absence of surfactant, the attraction between water molecules can cause alveolar collapse.
Alveolar surfactant ( 表面活性物质 )
• Secreted by type II alveolar epithelial cells
• Surfactant is a complex mixture of
– Several phospholipids ( 二软脂酰卵磷脂 dipalmitoyl phosphatidyl choline, DPPC)
– Surfactant-associated proteins
– Ions (calcium)

Type II alveolar epithelial cells


Physiological effect of Alveolar surfactant
• Reduces surface tension, eases expansion of lung• Maintains the stability of alveoli in different size• Keeps the dryness of alveoli

Neonatal respiratory distress syndrome (NRDS)( 新生儿呼吸窘迫综合征 ) lack of surfactant
retraction of soft tissue on inspiration

By reducing the surface tension of water, surfactant helps prevent alveolar collapse.

Laplace’s law: P=2T/r
Ta=Tb Ta>Tb
ra>rb ra>rb
Pa<Pb Pa=Pb

Pulmonary surfactant
• Pulmonary surfactant is a mixture of phospholipids and protein.
• It is secreted by type II alveolar cells.
• It lowers the surface tension of the water layer at the alveolar surface, which increases lung compliance, makes the lungs easier to expand.
• Its surface tension is lower in smaller alveoli thus stabilizing alveoli.
• A deep breath increases its secretion by stretching the type II cells. Its concentration decreases when breaths are small.
• Production in the fetal lung occurs in late gestation ( 妊娠 ).

Non-elastic resistance ( 非弹性阻力 )
• Airway resistance 气道阻力 : 80~90%
– caused by gas molecules and the inner wall of
airway
– R1/r4
• Inertial resistance 惯性阻力 • Viscous resistance 粘滞阻力 : The effect of surface
friction between a particle and a liquid.
• Regulation of the respiratory smooth muscle by
autonomic nervous system:
– Vagus nerve: Ach M receptor Contraction
– Sympathetic nerve: NE 2-receptor
Relaxation
• Regulation of the respiratory smooth muscle by
endocrine or paracrine factors:
– Histamine, Bradykinin Contraction
– NE, E, Isoproterenol Relaxation


Timed vital capacity ( 时间肺活量 )
Pulmonary volumes and capacities
• Spirometer ( 肺活量计 )
a spirometer---a device used to measure lung health.
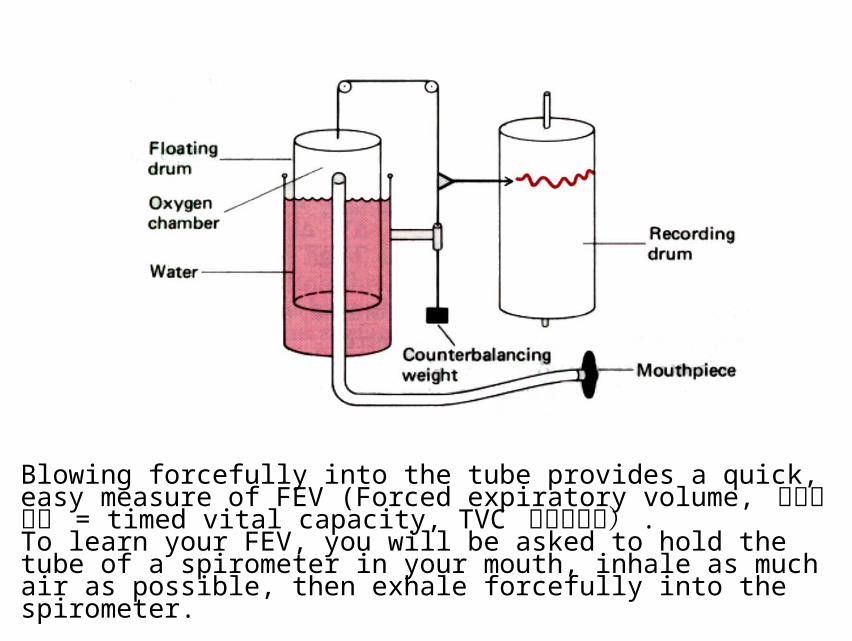
Blowing forcefully into the tube provides a quick, easy measure of FEV (Forced expiratory volume, 用力呼气量 = timed vital capacity, TVC 时间肺活量) .To learn your FEV, you will be asked to hold the tube of a spirometer in your mouth, inhale as much air as possible, then exhale forcefully into the spirometer.

Pulmonary volumes
• Tidal volume ( 潮气量 TV)
Volume of air inspired or expired with each normal breath
Normal value: 400~500 ml• Inspiratory reserve volume ( 补吸气量 IRV)
Amount of air that can be inspired above and beyond TV
Normal value: 1500~2000 ml
• Expiratory reserve volume ( 补呼气量 ERV)
Amount of air that can be expired after a tidal expiration
Normal value: 900~1200 ml
• Residual volume ( 残气量 RV)
The volume of air remaining in the lungs at the end of a maximal exhalation
Normal value: M 1500 ml, F 1000 ml


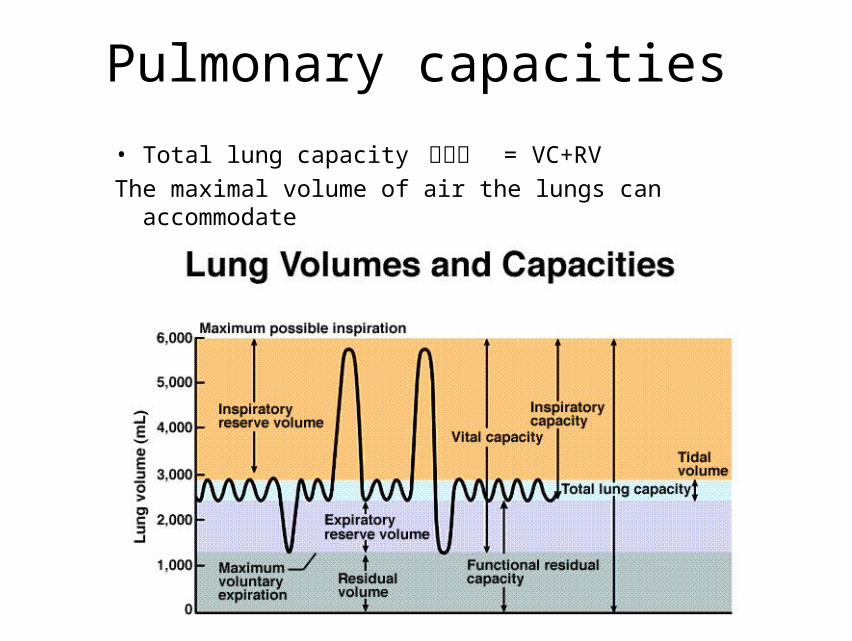
The tidal volume is the amount of air moved in/out of the airways in a single breathing cycle. Inspiratory and expiratory reserve volumes are the additional volume that can inspired or expired; all three quantities sum to the lung’s vital capacity. The residual volume is the amount of air that must remain in the lungs to prevent alveolar collapse.

Pulmonary capacities
• Inspiratory capacity 深吸气 = IRV+TV
• Functional residual capacity 功能残气量 The volume of air that still remains in the lungs after expiration of a resting tidal volume.
FRC = ERV+RV
• Vital volume ( 肺活量 Vital capacity, VC)
The maximal of air that a person can expire after a maximal inspiration
VC = TV+IRV+ERV
Normal value: M 3500 ml, F 2500 ml
Pulmonary capacities
• Total lung capacity 肺总量 = VC+RV
The maximal volume of air the lungs can accommodate

Pulmonary capacities
• Forced expiratory volume ( 用力肺活量, timed vital volume 时间肺活量 )
The maximal volume of air that can be exhaled as fast as possible from the lungs following a maximal inspiration
Normal value:
1st sec. (FEV1) -- 83 %2nd sec. (FEV2) -- 96 %3rd sec. (FEV3) -- 99 %

Pulmonary ventilation
• Pulmonary ventilation ( 每分通气量 VE)
The total amount of air inspired/expired during one minute
VE = TV x breaths/min = 500 X12 = 6000 ml

Pulmonary ventilation
• Alveolar ventilation ( 肺泡通气量 VA)
The amount of inspired air that is available for gas exchange
each minute
VA = (TV - dead space 无效腔 ) x breaths/min
= (500-150) X12 = 4200 ml

Dead space


Dead space
• Anatomical dead space
Volume in respiratory passageways which can not
be exchanged
~ 150ml
• Alveolar dead space
Alveoli which have little or no blood supply and
cease to function in gas exchange
Normally ~ 0

Because of the anatomic dead space, “Fresh” inspired air is diluted by the left over air remaining in the lungs from the previous breathing cycle.

Regulation of respiration
Breathing is controlled by the central neuronal network
to meet the metabolic demands of the body
– Neural regulation
– Chemical regulation

Respiratory center
• Medulla
• Pontine ( 脑桥 )
• Higher respiratory center: cerebral cortex,
hypothalamus & limbic system ( 下丘脑和边缘系统 )
• Spinal cord: respiratory motor neurons
低位脑干 -- 脑桥和延髓
Basic respiratory center: produce and control
the respiratory rhythm
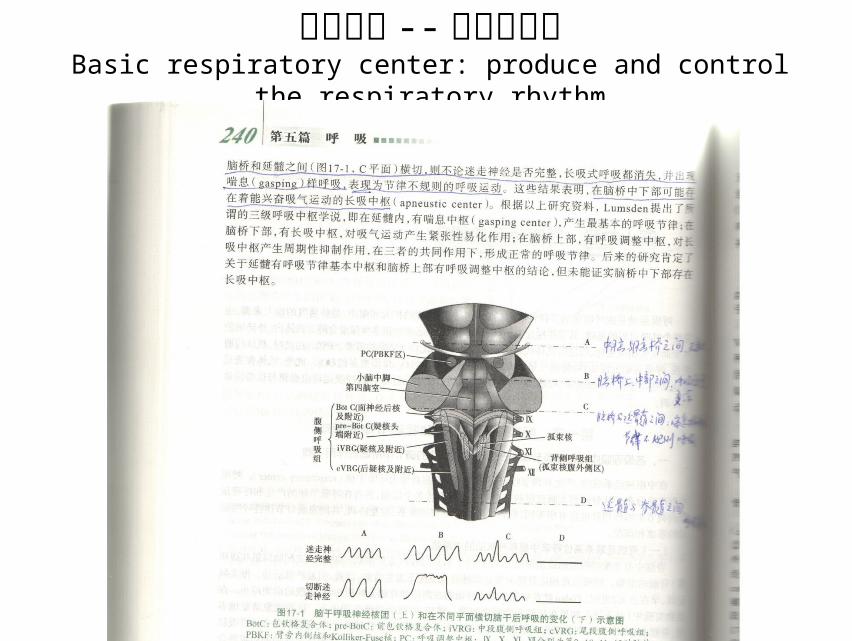
低位脑干 -- 脑桥和延髓Basic respiratory center: produce and control the respiratory rhythm
Respiratory center
• Dorsal respiratory group (medulla) – mainly causes
inspiration
• Ventral respiratory group (medulla) – causes either
expiration or inspiration
• Pneumotaxic center (upper pons 脑桥上部 ) – inhibits
apneustic center & inhibits inspiration,helps control the
rate and pattern of breathing
• Apneustic center (lower pons) – to promote inspiration
• Voluntary breathing center
– Cerebral cortex
• Automatic (involuntary) breathing center
– Medulla 髓
– Pontine 脑桥
Neural regulation of respiration


Neural generation of rhythmical breathing
The discharge of medullary inspiratory neurons provides rhythmic input to the motor neurons innervating the inspiratory muscles. Then the action potential cease, the inspiratory muscles relax, and expiration occurs as the elastic lungs recoil.
Chemical control of respiration
Chemoreceptors
– Central chemoreceptors 中枢化学感受器 : medulla
• Stimulated by [H+] in the CSF
– Peripheral chemoreceptors 外周化学感受器 :
• Carotid body
– Stimulated by arterial PO2 or [H+]
• Aortic body

Central chemoreceptors

Chemosensory neurons that respond to changes in blood pH and gas content are located in the aorta and in the carotid sinuses; these sensory afferent neurons alter CNS regulation of the rate of ventilation.
Peripheral chemoreceptors

舌咽神经
迷走神经

Hering-Breuer inflation reflex(Pulmonary stretch reflex 肺牵张反射 )
The reflex is originated in the lungs and mediated by the
fibers of the vagus nerve ( 迷走神经 ):
– Pulmonary inflation reflex ( 肺扩张反射 ):
• inflation of the lungs, eliciting expiration.
– Pulmonary deflation reflex ( 肺缩小反射 ):
• deflation, stimulating inspiration.

Pulmonary inflation reflex
Inflation of the lungs +pulmonary
stretch receptor +vagus nerve -
medualar inspiratory neurons
+eliciting expiration



Small changes in the carbon dioxide content of the blood quickly trigger changes in ventilation rate.
Effect of carbon dioxide on pulmonary ventilation
CO2 respiratory activity

Central and peripheralchemosensory neurons that respond to increased carbon dioxide levels in the blood are also stimulated by the acidity from carbonic acid, so they “inform” the ventilation control center in the medulla to increase the rate of ventilation.
CO2+H2O H2CO3 H+ + HCO3-
Regardless of the source, increases in the acidity of the blood cause hyperventilation.
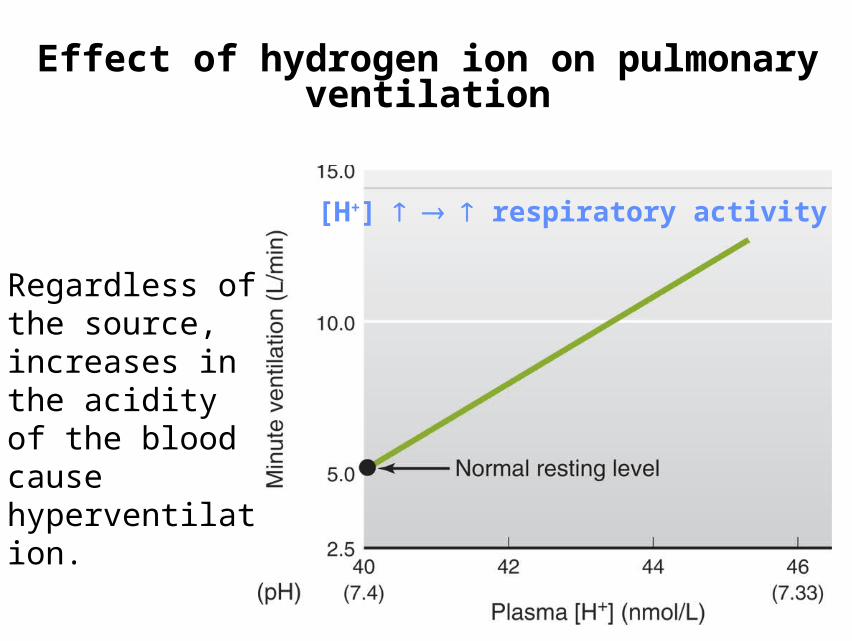
Effect of hydrogen ion on pulmonary ventilation
[H+] respiratory activity

Regardless of the source, increases in the acidity of the blood cause hyperventilation, even if carbon dioxide levels are driven to abnormally low levels.
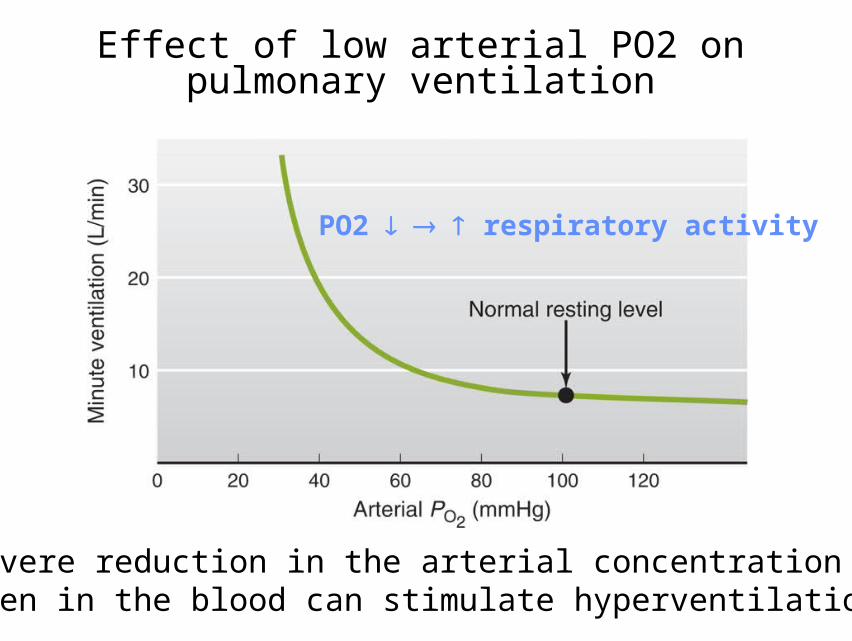
A severe reduction in the arterial concentration of oxygen in the blood can stimulate hyperventilation.
Effect of low arterial PO2 on pulmonary ventilation
PO2 respiratory activity
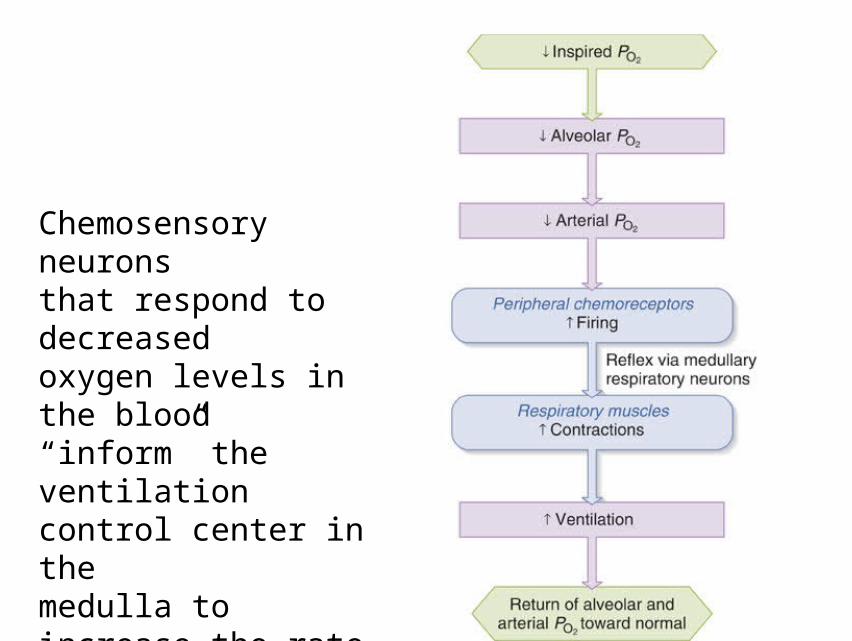
Chemosensory neuronsthat respond to decreasedoxygen levels in the blood“inform” the ventilation control center in themedulla to increase the rate of ventilation.

The levels of oxygen, carbon dioxide, and hydrogen ions in blood and CSF provide information that alters the rate of ventilation.
In summary:

Summary

Questions
Describes the effects of PCO2, [H+] and PO2 on alveolar ventilation and their mechanisms
CO2 - respiratory activity; Peripheral mechanism and central mechanism, the latter is the main one.
[H+] - respiratory activity; Peripheral mechanism and central mechanism, the former is the main one.
PO2 - respiratory activity; Peripheral mechanism is excitatory.
Questions
• What is the major result of the ventilation-
perfusion inequalities throughout the lungs?
• Describe the factors that influence gas exchange
in the lungs.
• If an experimental rabbit’s vagi were obstructed
to prevent them from sending action potential,
what will happen to respiration?