牙科公共衛生學 prevention & detection of oral cancer 口腔癌之預防與偵測...
TRANSCRIPT

牙科公共衛生學
Prevention & detection of oral cancer
口腔癌之預防與偵測
陳玉昆副教授 : 高雄醫學大學 口腔病理科 07-3121101~2755 [email protected]

參 考 書 目1. Gibbs WW. Untangling the roots of cancer. Sci Am 2003;289:56-65.2. What you need to know about cancer. Sci Am 1996 ;289:28-119.3. Hannen EJM, Riediger D. The quantification of angiogenesis in relation to metastasis in oral cancer: a review. Int. J
Oral Maxillofac Surg 2004;33:2-7.4. Shieh et al. Role of angiogenic and non-angiogenic mechanisms in oral squamous cell carcinoma: correlation with
histologic differentiation and tumor progression. J Oral Pathol Med 2004;33:601-6.5. Sharma DC. Betel quid and areca nut are carcinogenic without tobacco. Lancet Oncol 2003;4:587.6. Sharma DC. Indian betel quid more carcinogenic than anticipated. Lancet Oncol 2001;2:464.7. Braakhuis BJM et al. A genetic progression model of oral cancer: current evidence and clinical implications. J Oral
Pathol Med 2004;33:317-22.8. Braakhuis BJM et al. A Genetic explanation of slaughter’s concept of field cancerization: evidence and clinical
implications. Cancer Res 2003;63:1727-30.9. Loktionov A. Common gene polymorphisms, cancer progression and prognosis. Cancer Letters 2004;208 :1-33.10. Desmaze C et al. Telomere-driven genomic instability in cancer cells. Cancer Letters 2003;194:173-82.11. Hiyama E & Hiyama K. Telomerase as tumor marker. Cancer Letters 2003;194:221-33.12. Kaohsiung Medical University, Oral Pathology Department13. Huang AH et al. Isolation and characterization of normal hamster buccal pouch stem/stromal cells – a potential oral
cancer stem/stem-like cell model. Oral Oncol 2009;45: e189-e195.14. Umezawa & Gorham. Dueling models in head and neck tumor formation. Lab Investig 2010; 90:1546-8.15. Spillane JB, Henderson MA. Cancer stem cells: a review. ANZ J Surg 2007;77:464-8.16. Zhou ZT, Jiang WW. Cancer stem cell model in oral squamous cell carcinoma. Curr Stem Cell Res Ther 2008;3:17–20.17. Harper LJ et al. Stem cell patterns in cell lines derived from head and neck squamous cell carcinoma. J Oral Pathol Med
2007;36:594-603.18. Lim YC et al. Cancer stem cell traits in squamospheres derived from primary head and neck squamous cell carcinomas.
Oral Oncol 2011;47:83-91.
1. Gibbs WW. Untangling the roots of cancer. Sci Am 2003;289:56-65.2. What you need to know about cancer. Sci Am 1996 ;289:28-119.3. Hannen EJM, Riediger D. The quantification of angiogenesis in relation to metastasis in oral cancer: a review. Int. J
Oral Maxillofac Surg 2004;33:2-7.4. Shieh et al. Role of angiogenic and non-angiogenic mechanisms in oral squamous cell carcinoma: correlation with
histologic differentiation and tumor progression. J Oral Pathol Med 2004;33:601-6.5. Sharma DC. Betel quid and areca nut are carcinogenic without tobacco. Lancet Oncol 2003;4:587.6. Sharma DC. Indian betel quid more carcinogenic than anticipated. Lancet Oncol 2001;2:464.7. Braakhuis BJM et al. A genetic progression model of oral cancer: current evidence and clinical implications. J Oral
Pathol Med 2004;33:317-22.8. Braakhuis BJM et al. A Genetic explanation of slaughter’s concept of field cancerization: evidence and clinical
implications. Cancer Res 2003;63:1727-30.9. Loktionov A. Common gene polymorphisms, cancer progression and prognosis. Cancer Letters 2004;208 :1-33.10. Desmaze C et al. Telomere-driven genomic instability in cancer cells. Cancer Letters 2003;194:173-82.11. Hiyama E & Hiyama K. Telomerase as tumor marker. Cancer Letters 2003;194:221-33.12. Kaohsiung Medical University, Oral Pathology Department13. Huang AH et al. Isolation and characterization of normal hamster buccal pouch stem/stromal cells – a potential oral
cancer stem/stem-like cell model. Oral Oncol 2009;45: e189-e195.14. Umezawa & Gorham. Dueling models in head and neck tumor formation. Lab Investig 2010; 90:1546-8.15. Spillane JB, Henderson MA. Cancer stem cells: a review. ANZ J Surg 2007;77:464-8.16. Zhou ZT, Jiang WW. Cancer stem cell model in oral squamous cell carcinoma. Curr Stem Cell Res Ther 2008;3:17–20.17. Harper LJ et al. Stem cell patterns in cell lines derived from head and neck squamous cell carcinoma. J Oral Pathol Med
2007;36:594-603.18. Lim YC et al. Cancer stem cell traits in squamospheres derived from primary head and neck squamous cell carcinomas.
Oral Oncol 2011;47:83-91.

探索癌症之旅
始 點How cancerarise
Stages of carcinogenesis
癌化的標準教條
四種癌化理論
Field cancerization
癌細胞的六種超能力
癌症的預防
學 習 目 標
終 點11
22
3344
55
66
77

In this model, clonal variants, including stromal cells derived from tumor cells, generate a microenvironment (niche) for tumor cells, and support tumor progression after tumor cells undergo clonal evolution.
Stochastic Clonal Evolution Model
第一站: How Cancer Arises
Ref. 14
Stochastic clonal evolution model Interaction between tumor cellsand stromal cells
Tumor cell
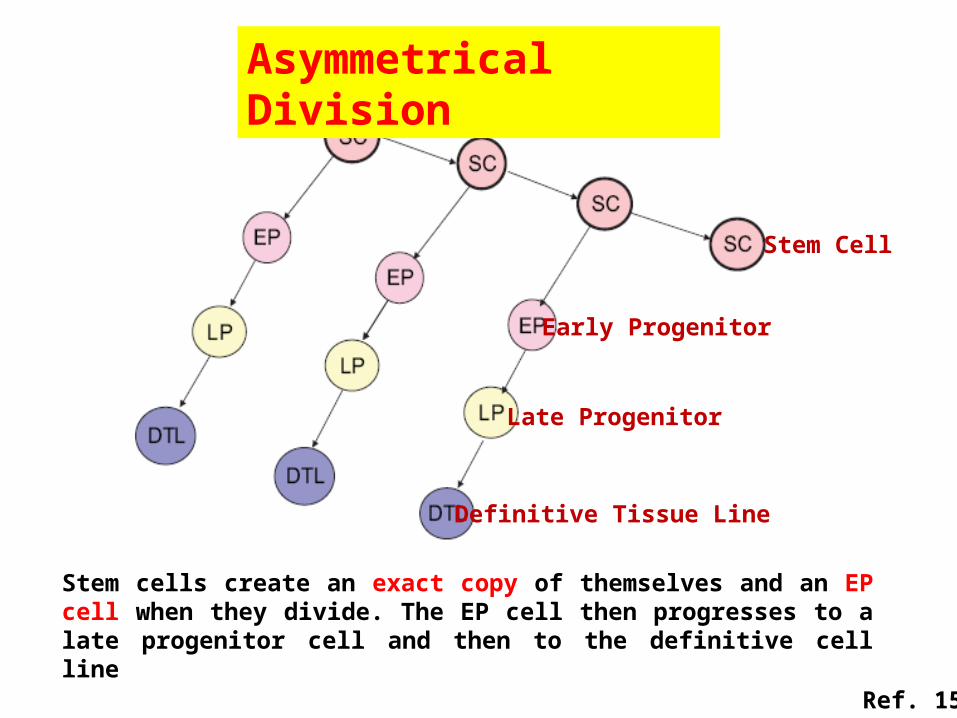
Stem cells create an exact copy of themselves and an EP cell when they divide. The EP cell then progresses to a late progenitor cell and then to the definitive cell line
Asymmetrical Division
Definitive Tissue Line
Early Progenitor
Late Progenitor
Stem Cell
Ref. 15

(a) The traditional model of tumor formation. A series of mutations affect a mature cell, causing it to become malignant. Any cell has the potential to form a tumor
Traditional Model ofTumor Formation
MatureDefinitiveTissueCell
TumorTumor
Mutation
Mutation
Mutation
Mutation Onlyat the Stem Cell
(b) Mutation only at the stem cell or progenitor cell level. The cancer stem cell replicates forming an exact copy of itself as well as a continuous supply of heterogeneous tumor cells
Tumor
Stem CellMutation
Ref. 15

Cancer Stem Cell Model
mutation
mutationSelf-renewingstem cell
Progenitorcell
Mature cell
Cancer cell
Self-renewingcancer stem cell
Ref. 15
In the stem cell model, only the stem cells or their progenitor cells have the ability to form tumors. Tumor characteristics vary depending on which cell undergoes the malignant transformation

Comparison of Somatic and Cancer Stem Cells
Somatic Stem Cell Cancer Stem Cell
Self renew, highly regulated
Self-renew, poorly regulated
Differentiate, produces mature tissue
Differentiate, produces tumor
Migrate to distant tissuesMetastasize to distant sites
Long lifespan Long lifespan
Resistant to apoptosisResistant to apoptosis
Ref. 15
• The hierarchical stem cell structure present in human oral epithelia indicates that stem cells are the only long-time residents of oral epithelia and, consequently, the only cells able to accumulate the necessary number of genetic changes for malignancy to develop
Stem cell - Oral Epithelia
• According to the progression model, the development of most of OSCC takes months or years.
• As normal human oral epithelia have a rate of renewal estimated to be about 14-24 days, most epithelial cells do not exist long enough to accumulate the genetic changes necessary for the development of an OSCC.

1, CSC might come from epithelial SC or progenitor within basal layer with genetic alterations; 2, muscle-derived SCs; 3, fibroblast-derived SCs; 4, vessel wall-derived SCs; 5, blood-derived SCs; and 6, adipose derived SCs.
A Schematic Diagram Showing Sites of Origins of Putative CSCs in OSCC
Ep
ith
eliu
mC
on
nec
tive
tis
sue
Ref. 16

Putative Cell Surface Markers of Presumptive CSC
SP-C+CCA+
Tumor Type Surface Markers
Ref. 16

CD44+CD24- Lineage negative
CD44+CD24-
CD44+CD24-Tumor formed
New tumor formed
Ref. 16
A minority population of CD44+ cancer cells (<3%/<10% of the cells in head and neck SCC cell line), but not the CD44- cancer cells, generate new tumors in vivo

Potential Mechanisms of CSC Formation
CSC
MUTATIONA
Progenitors
Self renewal
Self renewal
Stem/progenitor cellsDifferentiated cells
Ref. 16
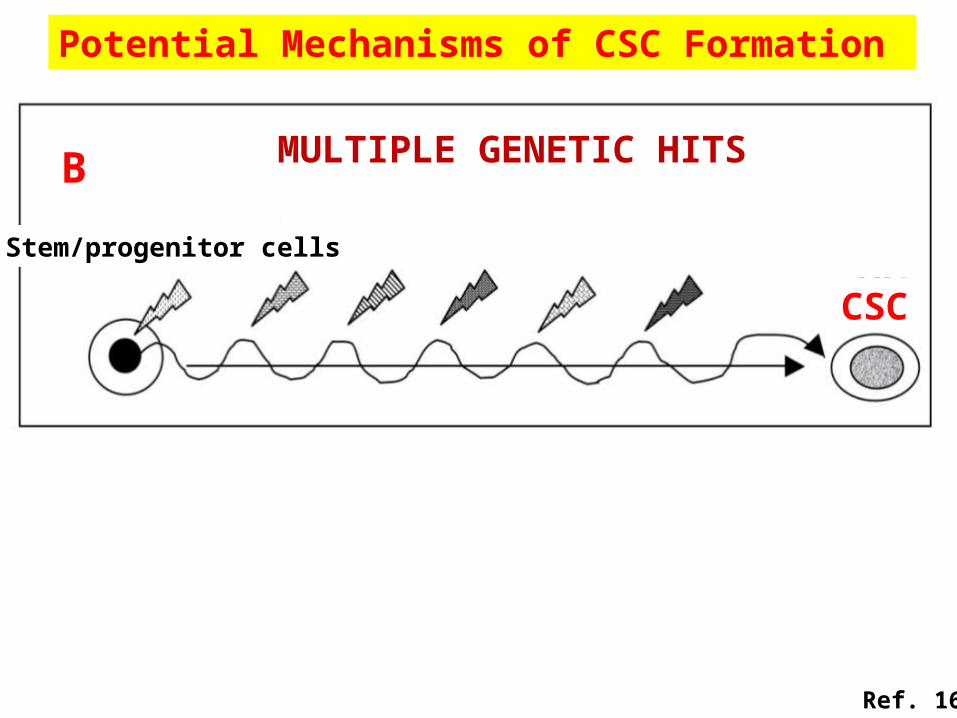
CSC
MULTIPLE GENETIC HITSB
Stem/progenitor cells
Potential Mechanisms of CSC Formation
Ref. 16

CSC
FUSIOND
Cancer cell
Stem/progenitor cells
Potential Mechanisms of CSC Formation
Ref. 16
CSC
MULTISTEP DEDIFFERENTIATIONC
Cancer cell

DMBA-Induced Hamster Buccal Pouch Model
14-wk
Normal
Carcinogen: DMBA
• Hamster buccal-pouch mucosa provides one of the most widely-accepted experimental models for oral carcinogenesis
Ref. 12
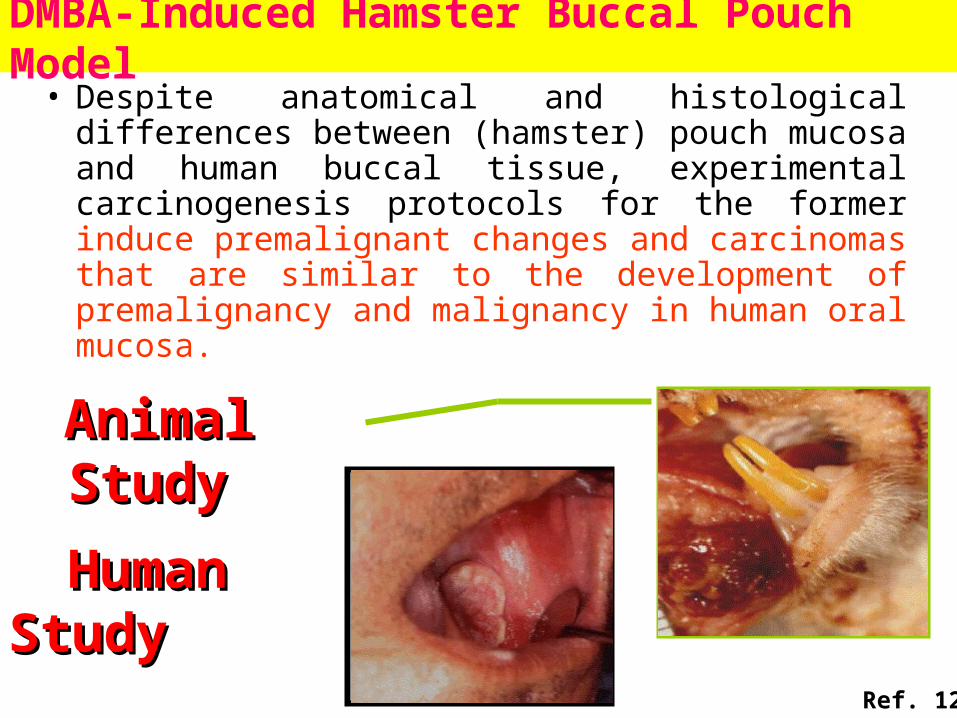
DMBA-Induced Hamster Buccal Pouch Model• Despite anatomical and histological differences
between (hamster) pouch mucosa and human buccal tissue, experimental carcinogenesis protocols for the former induce premalignant changes and carcinomas that are similar to the development of premalignancy and malignancy in human oral mucosa.
AnimalAnimal StudyStudy
HumanHuman StudyStudy
Ref. 12

A B
Isolation and Characterization of Stem Cells from Normal Hamster Buccal Pouch (HBPSC)
Representative sample of the normal hamster buccal pouch tissues revealed no obvious grossly (A; inset) and histological (B, Hematoxylin & eosin stain, 200) changes.
Ref. 13

Minimal Criteria of Stem Cell Capacity
• Self-renewal---Colony forming unit (CFU)---Proliferation
• One or more lineages differentiation---Adipogenic differentiation---Osteogenic differentiation---Chondrogenic differentiation---Neurogenic differentiation
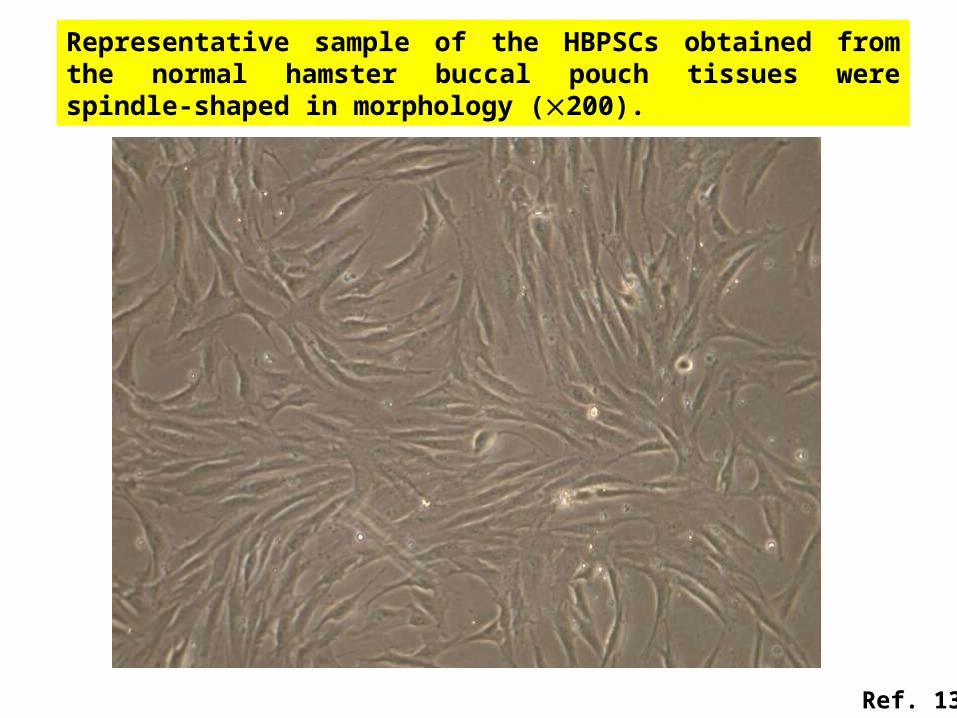
Representative sample of the HBPSCs obtained from the normal hamster buccal pouch tissues were spindle-shaped in morphology (200).
Ref. 13
A
B
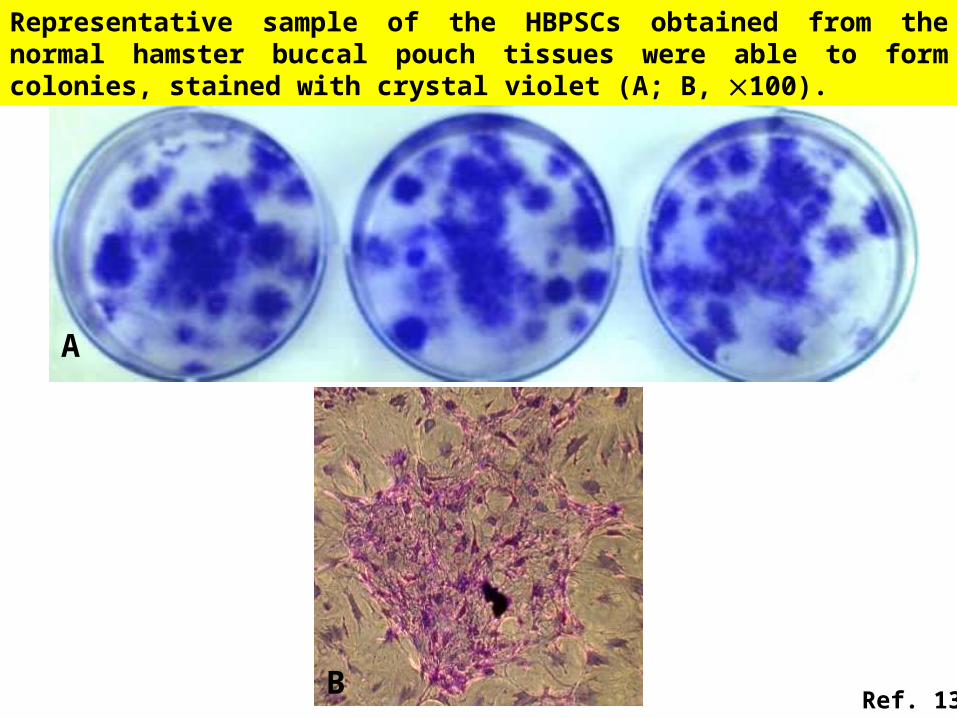
Representative sample of the HBPSCs obtained from the normal hamster buccal pouch tissues were able to form colonies, stained with crystal violet (A; B, 100).
Ref. 13

A B
Cytoplasmic keratin (A, 200) and vimentin (B, 200) stainings were noted for the representative sample of the HBPSCs obtained from the normal hamster buccal pouch tissues.
Ref. 13

Prol
ifera
tion
rate
(# o
f fol
ds)
Pouch 2 Pouch 3
Proliferation rates for the HBPSCs obtained from the three normal hamster buccal pouch tissues (p: passage).
Ref. 13

A
NM GAPDH PPAR
B
50
100
150
200250300350400
bp
(A) Representative sample of the HBPSCs obtained from the normal hamster buccal pouch tissues were able to differentiate towards adipogenic lineage (×200). (B) Expression of PPARγ mRNA (401-bp) upon RT-PCR also indicates adipogenic lineage of HBPSCs obtained from normal hamster buccal pouch tissues; GAPDH (135-bp) was the positive control; H2O was the negative control (N); M: molecular weight marker.
Ref. 13

Representative sample of the HBPSCs obtained from the normal hamster buccal pouch tissues were able to differentiate towards chondrogenic lineage (×200); inset: a yellowish chondroid pellet (~3mm in diameter).
Ref. 13
Representative sample of the HBPSCs obtained from the normal hamster buccal pouch tissues were able to differentiate towards osteogenic lineage (×200).

Representative sample of the HBPSCs obtained from the normal hamster buccal pouch tissues expressed the differentiation markers (Osteonectin: 323-bp & Nestin: 416-bp) and stem cell markers (Nanog: 364-bp, Rex-1: 232-bp & Oct-4: 717-bp) upon RT-PCR. GAPDH (135-bp) was the positive control; H2O was the negative control (N); M: molecular weight marker.
M N GA
PD
H
Ost
eon
ecti
n
Ne
sti
n
Oc
t-4
Na
no
g
Re
x-1
100
200
300
400500600700
bp
Ref. 13

Representative sample of the HBPSCs obtained from the normal hamster buccal pouch tissues showed high expression for surface markers: CD29, CD90, and CD105 but very low expression for CD14, CD34, and CD45 (Black/blue line: isotype control, Red line: marker of interest; Max: maximum).
0.9
CD14
% o
f M
ax
100
CD 29
% o
f M
ax
93.6
100
CD 34
% o
f M
ax
100
1.7
CD 45
1.5
% o
f M
ax
100
CD 90
85.8
% o
f M
ax
100
51.3
CD 105
100
% o
f M
ax
100
Ref. 13

Isolation of normal HBPSC, we may follow in vitro the sequential changes of the normal HBPSCs during multistep oral carcinogenesis or the alternations of these cells upon irradiation treatment and/or chemotherapy. Hence, the isolated normal HBPSCs, would provide a potential avenue for the future study of CSCs of buccal SCCs.
DMBA-Induced Hamster Buccal Pouch Model

A colony with holoclone characteristics of circular outline and tightly packed cobblestone’ cells (h) is surrounded by cells with a spaced and fusiform paraclone morphology (p). A small colony (m) perhaps corresponds to a meroclone.
Comparison of Morphology Between Our Isolated
Cells & Literature ResultsOur isolated cells from DMBA-induced cancer pouch tissue
Refs. 13, 17

Self-renewal, stem cell marker expression, aberrant differentiation, and tumor-initiating potential
OSCC-driven squamospheres demonstrated:(1)A number of stem cell markers, such as CK5, OCT4, SOX2, nestin, and CD44, Bmi-1, CD133, ALDH1(2) Single-dissociated squamosphere cells were able to form new squamospheres within 1 week of reseeding(3) Serum treatment led HNSCC-driven squamospheres to be non-tumorigenic differentiated cancer cells(4) Injection of as few as 100 undifferentiated squamosphere cells in nude mice gave rise to tumor formation
Hallmarks of CSCs (1)
CSCs is known to be significantly resistant to various chemotherapeutic agents (cisplatin, 5-fluorouracil (FU), paclitaxel, and doxetaxel)

Hallmarks of CSCs (2)
Ref. 18

Genticallyaltered cell
HyperlasiaDysplasia
Tumor developmentoccurs in stages
Geneticallyalteredcell (CSC) Hyperplasia
Dysplasia
Oral premalignant lesionsLeukoplakia, Erythroplakia, Oral submucous fibrosis, Verrucous hyperplasia, Erosive lichen planus
基底層完整
基底層完整
Initiated cell起始細胞
第二站 : Stages of Carcinogenesis
Ref. 1

In situ cancer
Invasive cancer
Blood vessel/lymphatic vessel
Ref. 1
How Cancer Spreads

Primary tumor
Normal epithelial cell
Basement membrane
Invasive tumor cellBlood vessel/lymphatic channel
How Cancer Spreads
Ref. 1

Endothelial/lymphaticlining
Basement membrane
Metastatic cellin circulation
Secondary tumor site
Tumor celladheringto capillary
Ref. 1
How Cancer Spreads

Initiation Phase (Early) 第二站 : Further look on stages of carcinogenesis
去毒
Ref. 9

Initiation Phase (Late) Ref. 9
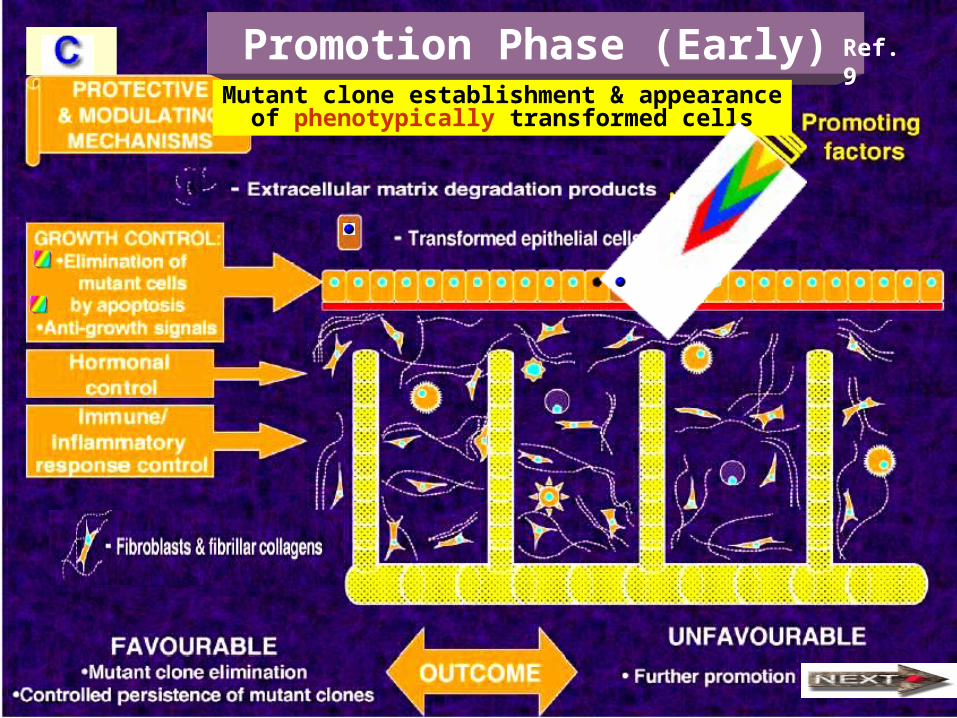
Promotion Phase (Early) Mutant clone establishment & appearance
of phenotypically transformed cells
Ref. 9

Promotion Phase (Late) Establishment of phenotypically
transformed cell population (dysplasia)
Ref. 9

Progression Phase (Early)
Malignisation
Ref. 9

Progression Phase (Middle)
Microinvasion
Ref. 9

Progression Phase (Late) Advanced invasion and metastasis
ChemotherapyRef. 9

NormalCell CycleCell enlargesand makesnew proteins
Beginningof cycleCell
divides(mitosis)
Cell preparesto divide
Cell replicatesas DNA
Cell rests
Restriction point:celldecides whetherto commit itself tothe complete cycle
崗 哨
第三站 : 癌化理論的標準教條
G1 arrest
Ref. 2

InhibitorypathwaysNormal Cell
Inhibitoryabnormality
Stimulatoryabnormality
Stimulatorypathways
標準教條
致癌基因 抑癌基因
Ref. 2

Activation ofoncogene
Inactivation of tumor suppressor gene
Cell Cycle
失 控失 控
下 坡
下 坡
下 坡 煞 車 失 靈
油 門 全 開
Aberrant cell cycle — accelerated cars without brake Ref. 2

Oncogene (1) Genes for growth factors or their receptors
PDGF Codes for platelet-derived growth factorInvolved in glioma (a brain cancer)
erb-B Codes for the receptor for epidermal growth factorInvolved in glioblastoma (a brain cancer) and breast cancer
erb-B2 Also called HER-2 or neu. Codes for a growth factor receptor Involved in breast, salivary gland and ovarian cancers
RET Codes for a growth factor receptorInvolved in thyroid cancer
Genes for growth factors or their receptors
Ki-ras Involved in lung, ovarian, colon and pancreatic cancers
N-ras Involved in leukemia
Ref. 2

Oncogene (2) Genes for growth factors or their receptors
c-myc Involved in leukemia and breast, stomach and lung cancers
N-myc Involved in neuroblastoma (a nerve cell cancer) and glioblastoma
L-myc Involved in lung cancer
Genes for growth factors or their receptors
Bcl-2 Codes for a protein that normally blocks cell suicide.Involved in follicular B cell lymphoma
Bcl-1 Also called PRAD1. Codes for cyclin D1, a stimulatory component of the cell cycle clock.Involved in breast, head and neck cancers
MDM2 Codes for an antagonist of the p53 tumor suppressor protein. Involved in sarcomas and other cancers
Ref. 2
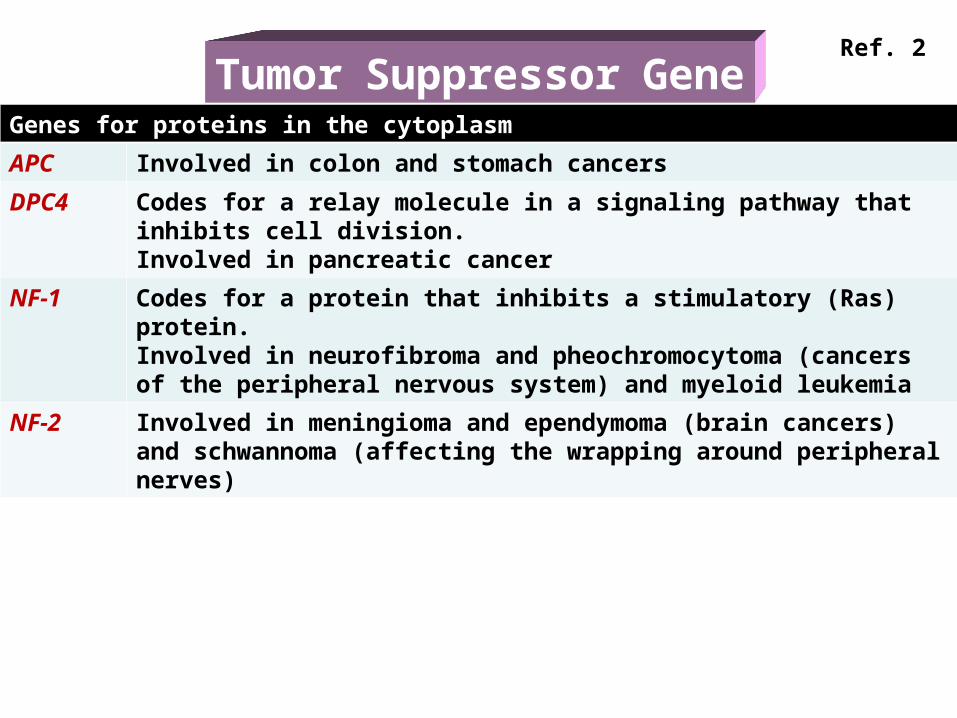
Tumor Suppressor GeneGenes for proteins in the cytoplasm
APC Involved in colon and stomach cancers
DPC4 Codes for a relay molecule in a signaling pathway that inhibits cell division.Involved in pancreatic cancer
NF-1 Codes for a protein that inhibits a stimulatory (Ras) protein.Involved in neurofibroma and pheochromocytoma (cancers of the peripheral nervous system) and myeloid leukemia
NF-2 Involved in meningioma and ependymoma (brain cancers) and schwannoma (affecting the wrapping around peripheral nerves)
Ref. 2

Tumor Suppressor Gene
Genes for proteins whose cellular locations is not yet clear
BRCA1 Involved in breast and ovarian cancers
BRCA2 Involved in breast cancer
VHL Involved in renal cell cancer
Genes for proteins in the nucleus
MTS1 Codes for the p16 protein, a braking component of the cell cycle clock. Involved in a wide range of cancers
RB Codes for the pRB protein, a master brake of the cell cycle. Involved in retinoblastoma and bone, bladder, small cell lung and breast cancer
p53 Codes for p53 protein, which can halt cell division and induce abnormal cells to kill themselves. Involved in a wide range of cancers
WT1 Involved in Wilms’ tumor of the kidney
Ref. 2
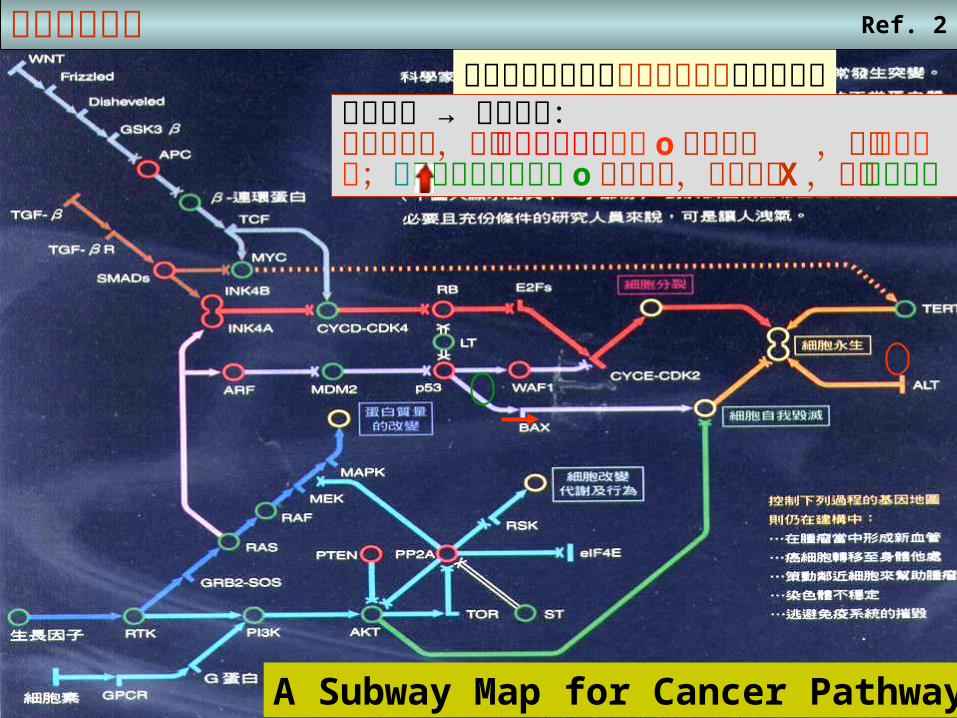
基因突變地圖在各種癌症中發現超過百種以上的突變基因癌化理論 → 標準教條:細胞循環中,正常促進細胞形成基因 o 過度活化 ,變成致癌基因;而抑制細胞形成基因 o 發生突變,失去功能 X ,成為抑癌基因
A Subway Map for Cancer Pathways
Ref. 2

標準教條
第四站癌化的四個理論
Ref. 2

修 正 教 條
修 正 教 條 在癌化前期的細胞基因組當中,累積的隨機突變有顯著的增加,終於影響到癌症相關基因
Ref. 2
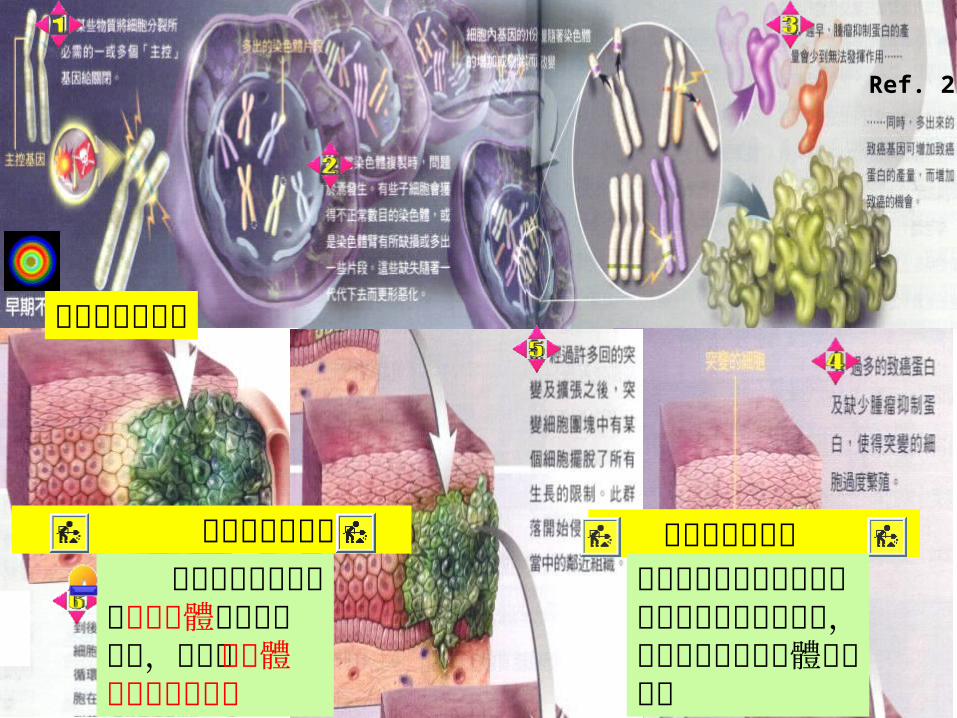
早期不穩定理論
早期不穩定理論 其餘兩個理論專注在非整倍體所扮演的角色,也就是染色體上大規模的變異
早期不穩定理論認為細胞分裂的主控基因受致癌物質影響而關閉,造成子代細胞染色體數目異常
Ref. 2

全盤非整倍體理論:非整倍體細胞的基因組非常不穩定,使得癌症基因極易發生突變而形成腫瘤
Ref. 2

癌症是一種基因的疾病然而癌症的複雜情況,卻不能用簡單的「基因突變」來描述。最近理論認為,染色體的異常可能才是細胞邁向癌症之路的第一步。
隨染色體起舞Ref. 2

正常 癌 症
Ref. 2Normal & Cancer Chromosomes

Field Cancerization (1)
Patch phase
Precursor lesionsdevelop within field
Carcinoma excised,field and precursorlesion remains
Expandingfield phase
Field
Second field tumordevelops fromprecursor lesion
Precursor lesionsbecomes carcinomaand new precursorbecomes develop
Epithelium
Connective tissue Basal layer withstem cells
第五站 :
Genetic altered
Ref. 7

Carcinoma
11q
Field Cancerization (2)
FieldPatch
Histological Proof
Chromosomal Proof
p armq arm
centromere
Normal
17p 3p, 9p, 8p, 18q
Ref. 8

癌細胞的第一種魔鬼能力第六站 : 癌細胞的六種魔鬼能力 Ref. 2

癌細胞的第二種魔鬼能力第六站 : 癌細胞的六種魔鬼能力 Ref. 2

癌細胞的第三種魔鬼能力第六站 : 癌細胞的六種魔鬼能力 Ref. 2

癌細胞的第四種魔鬼能力第六站 : 癌細胞的六種魔鬼能力 Ref. 2

Angiogenesis Factors (1)
Tumor island
Ref. 3

Angiogenesis Factors (2)
Newly-formedvessels
Tumor cellsNormal vessels
Ref. 4

Angiogenesis Factors (3)
Normal epithelium Dysplasia
Early localizedtumor
Advanced invasive
tumor
Normal vesselNewly-formed vesselTumor-lined vessel
Ref. 4

癌細胞的第五種魔鬼能力第六站 : 癌細胞的六種魔鬼能力
藍
p armq arm
centromere
Ref. 2

Consequences of teleomere lossin tumor cells
Teleomere( 末端粒腺體 )Normal
Mutant
Chromosomeinstability Chromosome
imbalances
Geneamplification
Tel
eom
ere
Fusions breakages
Duplicationof 16q: iso16qTrisomy 16qMonosomy 16q
Ref. 10

Regulation of Teleomeres –Alterative Length of Teleomere
(ALT), Teleomerase or BothGrowth Massive Apoptosis Immortalization
Teleomeresshorten
Teleomeresare critically short
Repeated cell divisions
Gen
om
ic I
nst
abil
ity
3. Teleomerase & ALT ?
2. Telomerase
Teleomeresare regulated
by1. ALT
Ref. 10
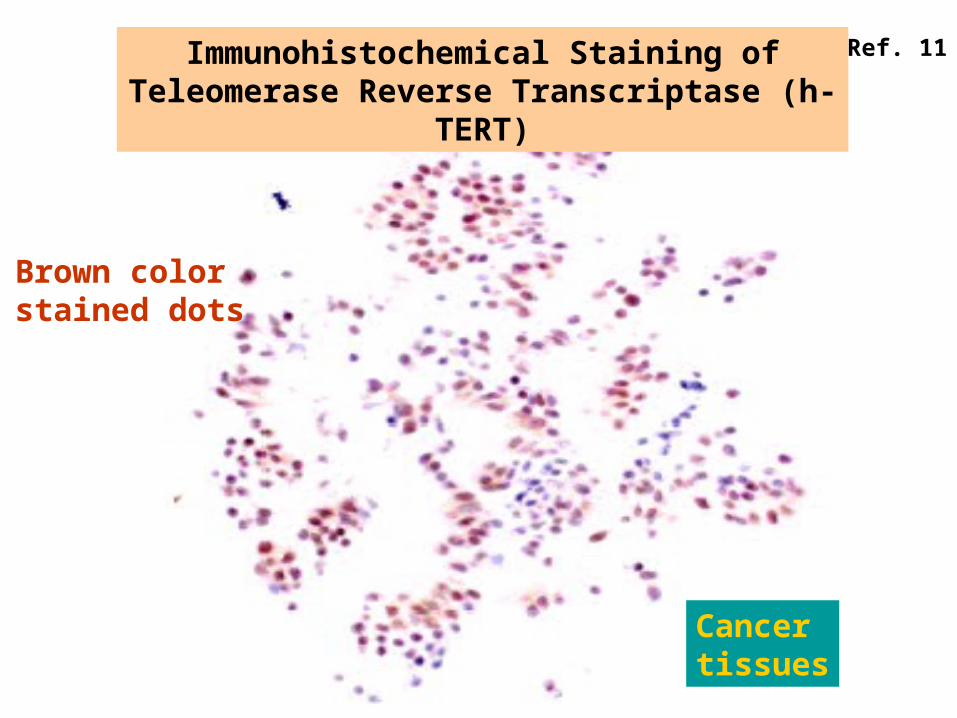
Immunohistochemical Staining of Teleomerase Reverse Transcriptase (h-TERT)
Brown colorstained dots
Cancertissues
Ref. 11

癌細胞的第六種魔鬼能力第六站 : 癌細胞的六種魔鬼能力
Ref. 2

Causesand Prevention
第七站
What Causes Cancer?
Chemical-environment
Virus
The top two causes - tobacco and diet-account for almost two thirds of all cancerdeaths and are amongst most correctable
PAPILLOMA VIRUS is asignificant cause of cancer
Ref. 1

Most Oral Carcinoma in Taiwan is Associated with Betel Quid
Ref. 12

Lancet Oncology 2001; August
印度檳榔包裝
Ref. 6

Lancet Oncology 2003; October
印度的檳榔攤
Ref. 5

Carcinogens in Work Place (1)
砷
石棉
Ref. 1

Carcinogens in Work Place (2) Ref. 1

Genes and Cancer Risk
基因警察
DNA修補基因
Ref. 1

Food
Strategiesfor MinimizingCancer Risk
Causes of currentcancer mortalityRealistic population goals for reduced cancer mortality
Risk factors
Estimated number of deaths in US (thousands per year)
100,000 to 125,000 current deaths
Simple, realistic preventive measurescould save hundreds of thousands of livesevery year in developed countries alone
Realistic Goals for Reducing Cancer Mortality Ref. 1

Chemopreventionof CancerSomeday people should be able toavoid cancer or delay its onset by takingspecially formulated pills or foods
Ref. 1

Chemoprevention 的原理
Healthy cell
Differentiation cell
Genetic mutationsthat can lead
to cancer
Processes that leadto excessive proliferation genetically damaged cells
Cancer cellDamaged cell(precancer
cell)
Programmed deathof altered cells(Apoptosis)
Ref. 1

BRCA1
Chromosome 17
A family search for BRCA1 mutation
Earlier Detection Earlier DetectionAdvances inCancer DetectionTests to look for the presence of a tumor before any symptoms appear may save more lives than new drug therapies do
Ref. 1

Some Family Causing Syndromes
Syndrome Cancers GeneDNA Testing cost
Ref. 1
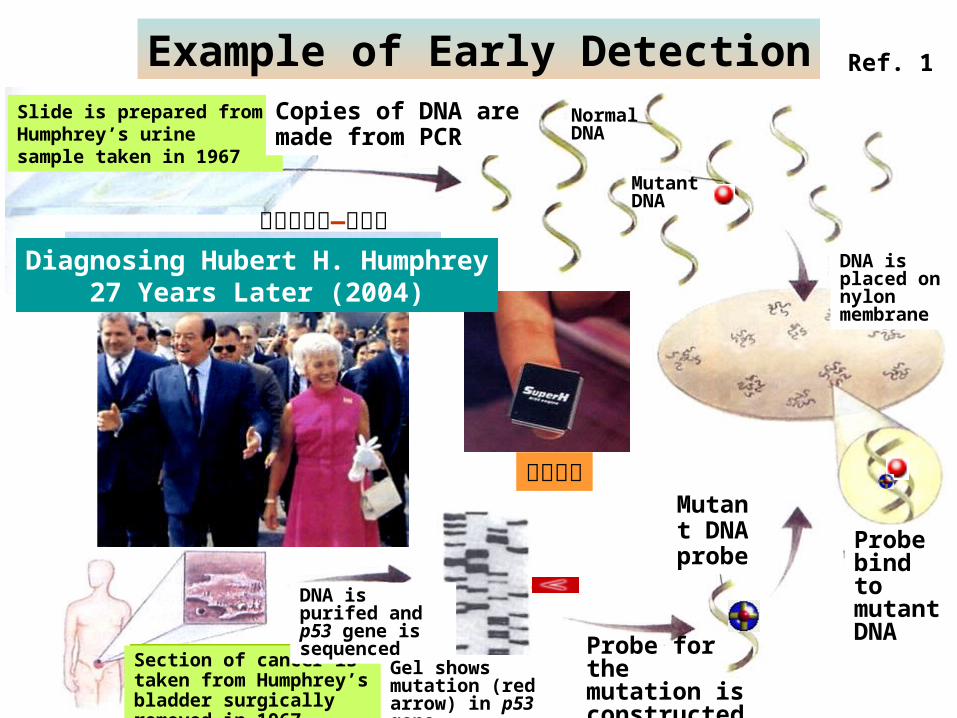
Slide is prepared from Humphrey’s urine sample taken in 1967
Section of cancer is taken from Humphrey’s bladder surgically removed in 1967
Copies of DNA aremade from PCR
Mutant DNAprobe
Probe bind to mutant DNA
Probe for the mutation is constructed
DNA is purifed and p53 gene is sequenced
Gel showsmutation (red arrow) in p53 gene
Normal DNA
Mutant DNA
DNA is placed on nylon membrane
生物晶片
美國副總統—韓福瑞Diagnosing Hubert H. Humphrey
27 Years Later (2004)
Ref. 1Example of Early Detection

Mammograms CT scan
Liver
Hepatoma
Breast
Advances inTumor Imaging
Advances inTumor Imaging
New tools yield a three-dimensional viewinside the body and automated adviceon interpreting the anatomical landscape
Ref. 1

Advances inTumor Imaging
Advances inTumor Imaging
Positron Emission Tomography
Ref. 1

Immunotherapy/Stem Cell Therapyfor Cancer
Immunotherapy/Stem Cell Therapyfor Cancer
Orange: Stroma Green: Colon cancer cell
Antibodies recognizes specific cells and can be used to find and selectively destroy tumor cells
Ref. 1

Fighting Cancer by Attacking Its Blood Supply
Inhibition of NOS enzymes by NOS inhibitor
Relatively lower level of NO produced by SCC facilitates angiogenesis & tumor dissemination
NO
NOS inhibitor
NO
Before therapyBefore therapy After therapyAfter therapy
NOS inhibitor
NOS inhibitor
NO: nitric oxide NOS: nitric oxide synthase
Ref. 1

Summaries瞭解以下各點:1. How cancer arise2. Stages of carcinogenesis3. 癌化的標準教條4. 四種癌化理論5. Field cancerization6. 癌細胞的六種超能力7. 癌症的預防