copy (2) of sepsis present เซกา revised
TRANSCRIPT

Khittisak Hankla, MD,FRCSTSeka Hospital
7th Oct 2014
Severe sepsis and Septic shock

SSC-Guidelines 2012.pdf

Content
What is Sepsis/Severe Sepsis and Septic shock?
Treatment Guideline
KPI
Pitfall/ Gap analysis


Pathophysiogyof
Severe sepsis and septic shock


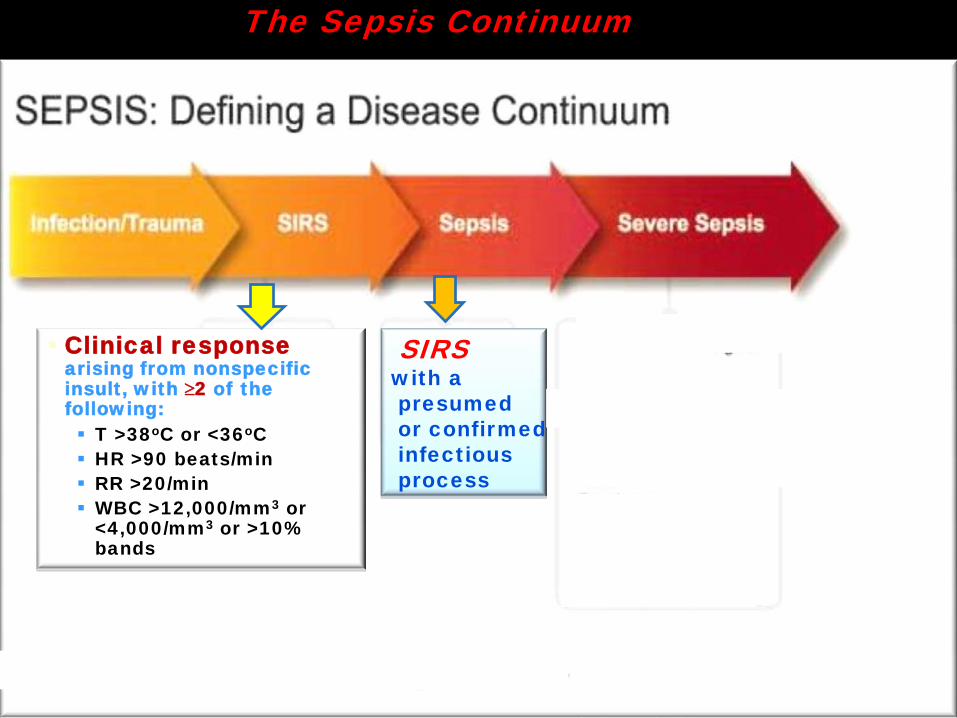
The Sepsis Continuum

The Sepsis Continuum
Clinical response arising from nonspecific insult, with ≥2 of the following: T >38oC or <36oC HR >90 beats/min RR >20/min or PaCO2< 32 WBC >12,000/mm3
<4,000/mm3 or >10% bands
The Sepsis Continuum
SIRSwith apresumedor confirmed infectiousprocess
Clinical response arising from nonspecific insult, with ≥2 of the following: T >38oC or <36oC HR >90 beats/min RR >20/min WBC >12,000/mm3 or
<4,000/mm3 or >10% bands

The Sepsis Continuum
SIRSwith apresumedor confirmed infectiousprocess
Clinical response arising from nonspecific insult, with ≥2 of the following: T >38oC or <36oC HR >90 beats/min RR >20/min WBC >12,000/mm3 or
<4,000/mm3 or >10% bands
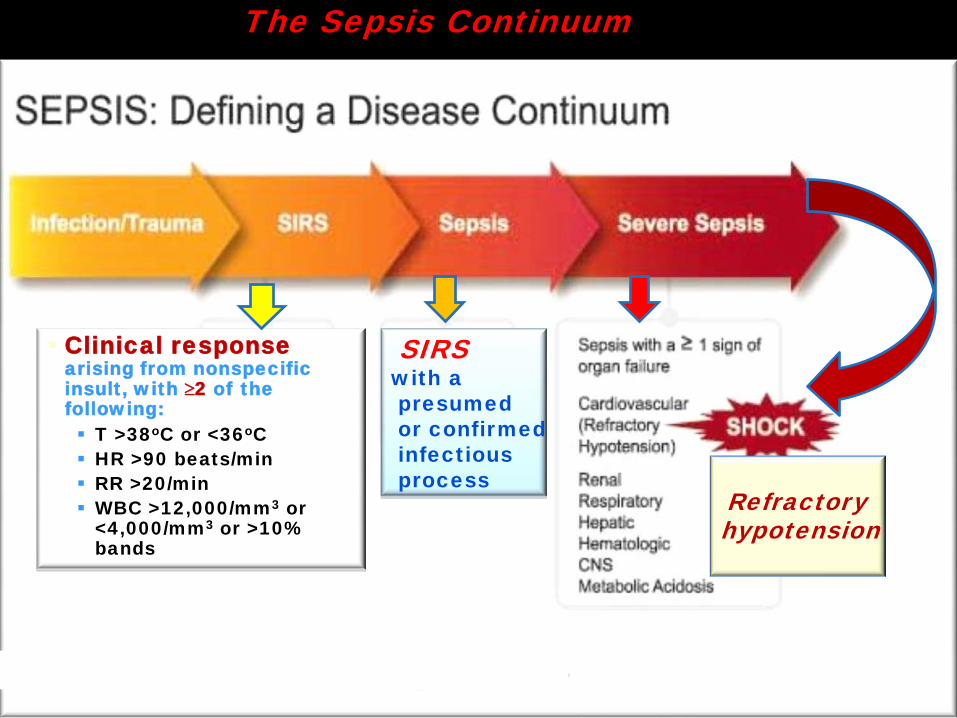
The Sepsis Continuum
SIRSwith apresumedor confirmed infectiousprocess
Clinical response arising from nonspecific insult, with ≥2 of the following: T >38oC or <36oC HR >90 beats/min RR >20/min WBC >12,000/mm3 or
<4,000/mm3 or >10% bands
Refractoryhypotension
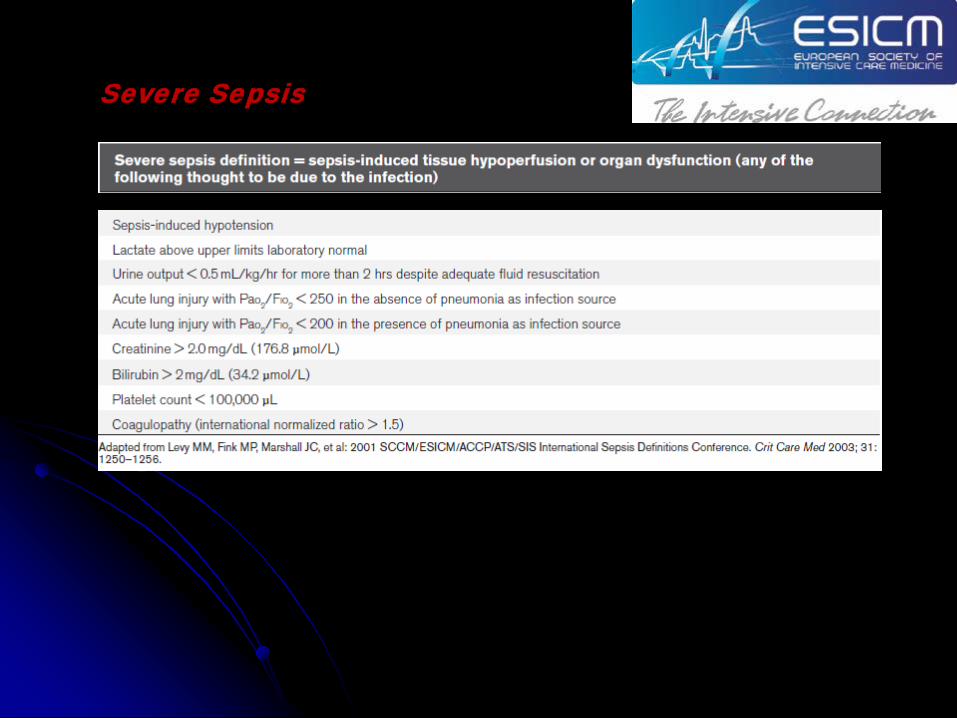
Severe Sepsis
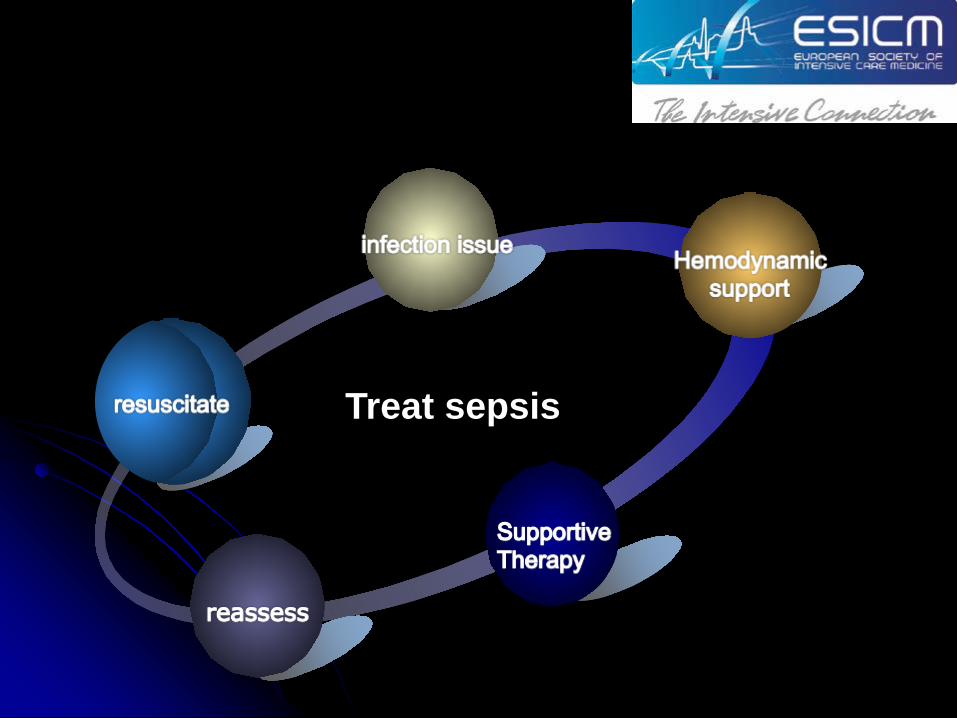
Treat sepsis

Resuscitation

1: The goals of initial resuscitation of sepsis-induced hypoperfusion should include all of the following (grade 1C): within 6 hrs after diagnosis
1: CVP 8–12 mm Hg ( JVP 8-10cm H2O) 2: MAP ≥ 65 mm Hg3: Urine output ≥ 0.5 ml/kg/hr4: Scvo2 or Svo2 ≥70% or ≥ 65%, respectively
Initial resuscitationInitial Resuscitation
2: Suggest targeting resuscitation to normalize lactate inpatients with elevated lactate levels as a marker of tissuehypoperfusion (grade 2C).

1: The goals of initial resuscitation of sepsis-induced hypoperfusion should include all of the following (grade 1C): within 6 hrs after diagnosis
1: CVP 8–12 mm Hg ( JVP 8-10cm H2O)
2: MAP ≥ 65 mm Hg3: Urine output ≥ 0.5 ml/kg/hr4: Scvo2 or Svo2 ≥70% or ≥
65%, respectively

ResuscitationInfection Issue

2:Antimicrobial Therapy
Infection Issue
1: Diagnosis
3: Identification source and Control

2:Antimicrobial Therapy
Infection Issue
1: Diagnosis
Cultures as clinically appropriate before antimicrobial therapy if no significant delay (> 45 mins) in the start of antimicrobial(s)
At least 2 sets of blood cultures (both aerobic and anaerobic bottles) be obtained before antimicrobial therapy with at least 1 drawn percutaneously and 1 drawn through each vascular access device, unless the device was recently (<48 hrs) inserted
3: Identification source and Control

Infection Issue
Diagnosis Antimicrobial TherapyThe administration of effective intravenous antimicrobialswithin the first hour of recognition of septic shock (grad1B)and severe sepsis without septic shock (grade 1C)should be the goal of therapy.
Empiric combination therapy should not be administered for more than 3–5 days. De-escalation to the most appropriate single therapy should be performed as soon as the susceptibility profile is known
Duration of therapy typically 7–10 days; longer courses may be appropriate in patients who have
- a slow clinical response- Undrainable foci of infection- Bacteremia with S. aureus; some fungal and viral
infections - Immunologic deficiencies, including neutropenia
Antimicrobial agents should not be used in patients with severe inflammatory states determined to be of noninfectious cause

Infection Issue
Diagnosis Antimicrobial Therapy

Infection Issue
3: Identification source and Control
DiagnosisAntimicrobial Therapy
ResuscitationInfection Issue
Hemodynamic support

Hemodynamic support And Adjunctive therapy
Adequate volume
Acceptable BPAdequate
tissue perfusion

Fluid Therapy of Severe Sepsis
Hemodynamic support And Adjunctive therapy
Adequate volume
Acceptable BPAdequate
tissue perfusion
Crystalloids as the initial fluid of choice in the resuscitation of severe sepsis and septic shock
Against the use of hydroxyethyl starches for fluid resuscitation of severe sepsis and septic shock
Albumin in the fluid resuscitation of severe sepsis and septic shock when patients require substantial amounts of crystalloids

Fluid Therapy of Severe Sepsis
Hemodynamic support And Adjunctive therapy
Adequate volume
Acceptable BPAdequate
tissue perfusion
การใหสารน้ํา
เลือก crystalloids เปนอันดับแรก ในการ resuscitationเร่ิม challenge โดยให crystalloid อยางนอย 30 มล/กก.

Hemodynamic support And Adjunctive therapy
Adequate volume
Acceptable BPAdequate
tissue perfusion
• Vasopressor and inotropic therapy
• Corticosteroid

Hemodynamic support And Adjunctive therapy
Adequate volume
Acceptable BPAdequate
tissue perfusion
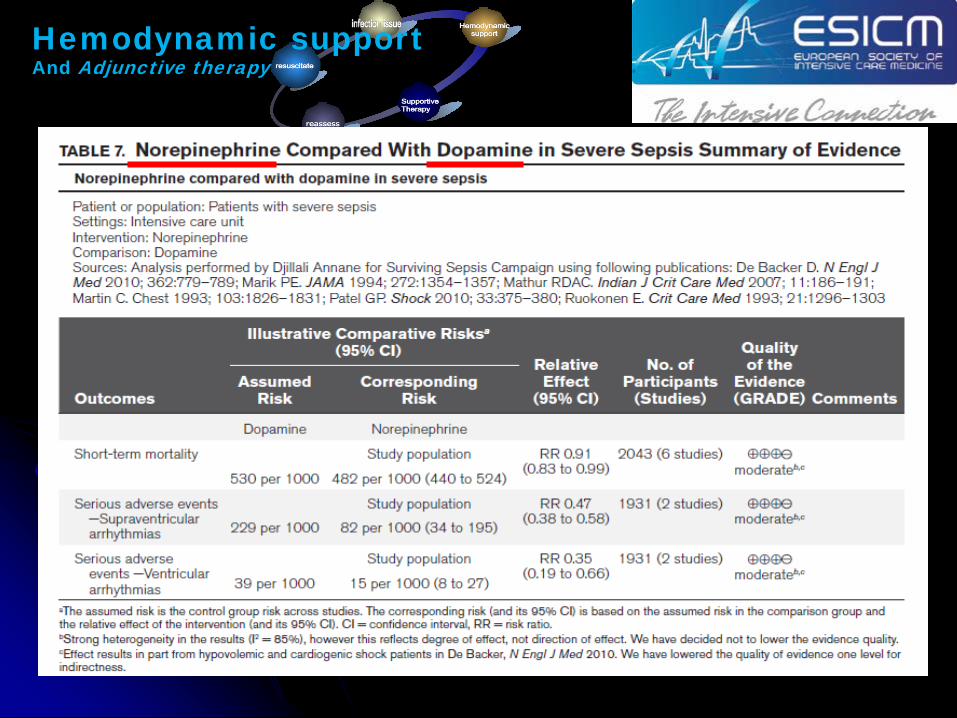
Vasopressor

Hemodynamic support And Adjunctive therapy
Adequate volume
Acceptable BPAdequate
tissue perfusion
Vasopressor
Hemodynamic support And Adjunctive therapy

Hemodynamic support And Adjunctive therapy
Adequate volume
Acceptable BPAdequate
tissue perfusion
Vasopressor and inotropic therapyA trial of Dobutamine infusion up to 20 micrograms/kg/min ( max) be administered or added to vasopressor (if in use) in the presence of
(A) Myocardial dysfunction as suggested by elevated cardiac filling pressures and low cardiac output, (grade 1C). or
(B) Ongoing signs of hypoperfusion, despite achieving adequate intravascular volume and adequate MAP (grade 1C).

Hemodynamic support And Adjunctive therapy
Adequate volume
Acceptable BPAdequate
tissue perfusion
• Vasopressor and inotropic therapy
•Corticosteroid

Hemodynamic support And Adjunctive therapy
Adequate volume
Acceptable BPAdequate
tissue perfusion
Corticosteroid
1:Not using IV hydrocortisone to treat adult septic shock patients if adequate fluid resuscitation and vasopressor therapy are able to restore hemodynamic stabilityIn case this is not achievable, we suggest IV Hydrocortisone at a dose of 200 mg per day (grade 2C).2. Not using the ACTH stimulation test to identify adults with septic shock who should receive hydrocortisone (grade 2B).3. In treated patients hydrocortisone tapered when vasopressors are no longer required (grade 2D)4. Corticosteroids not be administered for the treatment of sepsis in the absence of shock (grade 1D).5. When hydrocortisone is given, use continuous flow (grade 2D).

Hemodynamic support And Adjunctive therapy
Adequate volume
Acceptable BPAdequate
tissue perfusion
Corticosteroid
Hemodynamic not achieved goal :MAP < 65 mmHg despiteAdequate volumeAdequate or near adequate Vasopressor : IV Hydrocortisone 50 mg IV q 6 hr or 100 mg IV q 8 hr and tailor off within 7 days

Hemodynamic support And Adjunctive therapy
Adequate volume
Acceptable BPAdequate
tissue perfusion 1 : CVP 8–12 mm
Hg2: MAP ≥ 65 mm Hg3: Urine output ≥ 0.5 ml/kg/hr4: Scvo2 or Svo2 ≥70% or ≥ 65%, respective
?
No Yes
Achieve goal ท่ีเวลา......

Hemodynamic support And Adjunctive therapy
Adequate volume
Acceptable BPAdequate
tissue perfusion 1 : CVP 8–12 mm
Hg2: MAP ≥ 65 mm Hg3: Urine output ≥ 0.5 ml/kg/hr4: Scvo2 or Svo2 ≥70% or ≥ 65%, respective
?
No

Hemodynamic support And Adjunctive therapy
Adequate volume
Acceptable BPAdequate
tissue perfusion
1: Urine output < 0.5 ml/kg/hr2: Scvo2 or Svo2 <70% or < 65%, respective3: serum lactate > 4 mmol/l or capillary lactate > 5 mmol/l
Check 1 If MAP > 90 mmHg ::::: Vasopressor ; Keep MAP 60-90 mmHg2 If Hct < 30 % ; PRC3 If Hct ≥ 30 % ; Dobutamine 2.5 µg/kg/min titrate ครั้งละ 2.5 µg/kg/min Until
SVC O2 sat ≥ 70Max= 20 µg/kg/min
3 Checks

Hemodynamic support And Adjunctive therapy
Adequate volume
Acceptable BPAdequate
tissue perfusion 1: CVP 8–12 mm Hg
2: MAP ≥ 65 mm Hg3: Urine output ≥ 0.5 ml/kg/hr4: Scvo2 or Svo2 ≥70% or ≥ 65%, respective1st choice :Crystalloid
Colloid :alternative e.g Albumin

Hemodynamic support And Adjunctive therapy
Adequate volume
Acceptable BPAdequate
tissue perfusion
Vasopressor and InotropictherapyCorticosteroid
1: CVP 8–12 mm Hg2: MAP ≥ 65 mm Hg3: Urine output ≥ 0.5 ml/kg/hr4: Scvo2 or Svo2 ≥70% or ≥ 65%, respective1st choice :Crystalloid
Colloid :alternative e.g Albumin

Hemodynamic support And Adjunctive therapy
Adequate volume
Acceptable BPAdequate
tissue perfusion
Vasopressor and InotropictherapyCorticosteroid
1: CVP 8–12 mm Hg2: MAP ≥ 65 mm Hg3: Urine output ≥ 0.5 ml/kg/hr4: Scvo2 or Svo2 ≥70% or ≥ 65%, respective1st choice :Crystalloid
Colloid :alternative e.g Albumin Adjust MAPPRCDobutamine administration

ResuscitationInfection Issue
Hemodynamic support
Supportive therapy
Supportive Therapy: Metabolic and organs support

Supportive Therapy: Metabolic and organs support
Blood Product Administration ImmunoglobulinsSeleniumHistory of Recommendations Regarding Use of Recombinant Activated Protein C (rhAPC) Mechanical Ventilation of Sepsis-Induced Acute Respiratory Distress Syndrome (ARDS)Sedation, Analgesia, and Neuromuscular Blockade in SepsisGlucose Control Renal Replacement Therapy Bicarbonate Therapy Stress ulcer prophylaxisDeep Vein Thrombosis Prophylaxis Nutrition
Issue

Supportive Therapy: Metabolic and organs support
Blood Product Administration Issue

Supportive Therapy: Metabolic and organs support
Blood Product Administration• PRC transfusion occur only whenHb decreases to <7.0 g/dL to target a Hb of 7.0 –9.0 g/dL in adults (grade 1B).
•Platelets prophylactically when - Platelet counts are <10,000/mm3 (10 x 109/L) in the absence of apparent bleeding. - < 20,000/mm3 (20 x 109/L) if the patient has a significant risk of bleeding. - ≥50,000/mm3 [50 x 109/L] are advised for active bleeding, surgery, or invasive
procedures (grade 2D).
Issue

Supportive Therapy: Metabolic and organs support
Issue
This protocolized approach should target an upper blood glucose ≤180 mg/dL rather than an upper target blood glucose ≤ 110 mg/dL (grade 1A).
Glucose Control

Supportive Therapy: Metabolic and organs support
IssueStress Ulcer Prophylaxis
Coagulopathy :- Platelet <50,000 per/mm3,- INR >1.5, or PTT >2 times the control value
Mechanical ventilation for >48 hoursHistory of GI ulceration or bleeding within the past yearTraumatic brain injury, traumatic spinal cord injury, or burn injury≥ 2 of the following:
SepsisICU stay >1 weekOccult GI bleeding for ≥6 daysGlucocorticoid therapy (more than 250 mg hydrocortisone or the equivalent)

Supportive Therapy: Metabolic and organs support
IssueStress Ulcer Prophylaxis
Nutrition

Take home message

Take home message

Take home message
BP drop Load NSS อยางนอย 30 ml/kg กอนพิจารณา vasopressorLevophed is preferedตอง H/C x 2 spp. กอน start Antibiotic
-H/C เลือดใชอยางนอย 10 ml ตอขวด -แนะนําเจาะเลือด peripheral x 2 site ตางตําแหนงกันSevere sepsis or septic shock
antibiotic within 1 hr after diagnosis

ตัวชี้วัด เปาหมาย 2555 2556 2557 2558
ผูปวยไดรับยาปฏิชีวนะภายใน 1
ชั่งโมงหลงั วินิจฉัยSepsis≥ 80%
Septic Culture กอนใหยา
ปฏิชีวนะ≥ 80%
อัตราเสียชีวิตจาก Sepsis < 30%
อัตราการเกิดภาวะแทรกซอน < 50 %
Respiratory Failure
Acute Kidney Injury
Septic shock
อัตราการปฏิบัตติาม CPG ≥ 80%


เคร่ืองชี้วัด เปาหมาย 2555 2556 2557
อัตราท่ีผูปวยไดยาปฏิชีวนะภายใน 1 ชั่วโมงหลัง
วินิจฉัย Severe sepsis or septic shock≥80 %
อัตราผูปวยมีAdequate tissue perfusionภายใน 6 ชั่วโมง
≥80 %
อัตราการเสียชีวิตดวยภาวะ Sepsis ≤ 30%อัตราการเกิดภาวะแทรกซอน ≤ 50%
Septic shock
Respiratory failure
Acute kidney injury
ระยะวันนอนโรงพยาบาล
อัตราการปฏิบัติตาม CPG


Question ?

Thank you