후기 기종성 급성 췌장염과 다른 경과를 보이는 초기 기종성 ... ·...
TRANSCRIPT

증 례 ISSN 2093-9272일산병원학술지 2019;18(1):81-84
Volume 18 Number 1 June 2019 81
INTRODUCTION
Emphysematous pancreatitis (EP) is a severe acute
pancreatitis characterized by air in the pancreatic pa-
renchyma and peripancreatic space caused by infection.
Open necrosectomy had traditionally been the principle
treatment, but there have been unsolved high mortality
and morbidity associated with surgical management.
Recently, several studies have reported favorable out-
come through conservative treatment.1-3 Further, conser-
vative treatment and delayed percutaneous or endo-
scopic interventional treatment have been increasing
since the American College of Gastroenterology (ACG)
published guidelines for managing acute pancreatitis in
2013.1,2
Here, we report on an EP patient who rapidly pro-
gressed into a fatal course. His imaging findings and
clinical features differed from previously reported pa-
tients who showed good outcomes following conserva-
tive treatment.
CASE
A 61-year-old male visited the emergency room due to abdominal pain that had begun two hours prior to
후기 기종성 급성 췌장염과 다른 경과를 보이는
초기 기종성 급성 췌장염
국민건강보험 일산병원 영상의학과1 소화기내과, 2
황신혜1 이천균, 2 박수미, 1
Early-Phase Emphysematous Acute Pancreatitis could Differ from Late-Phase Emphysematous Pancreatitis
Shin Hye Hwang1, Chun Kyon Lee2, Sumi Park1
Department of 1Radiology and 2Institute of GastroenterologyNational Health Insurance Service Ilsan Hospital, Goyang, Korea
Emphysematous pancreatitis, a rare and severe acute pancreatitis, is characterized by air trapped in the pancreatic parenchyma and peripancreatic space caused by infection. Although it is believed to have high mortality, successful cases of conservative treatment have been reported recently. However, we experienced a patient who exhibited extensive pancreatic and peripancreatic gas formation in the first few hours without pancreatic necrosis on contrast-enhanced computed tomography, which could be considered “early-phase emphysematous pancreatitis.” The patient was transferred to the intensive care unit and treated con-servatively for systemic inflammatory response syndrome and acute renal failure; however, he died within 16 hours after symptom onset. Early-phase emphysematous pancreatitis can result in a fulminant course that differs from that of pancreatitis, with emphy-sematous changes that develop in the late phase (emphysematous infected pancreatic necrosis) that may necessitate early sur-gery or other intervention.
Key Words: Pancreatitis; Necrosis, Systemic inflammatory response syndrome
책임저자 박수미: 경기도 고양시 일산동구 일산로 10444 100국민건강보험 일산병원 영상의학과
전화 팩스: (031)900-0067, : 0303-3448-7107E-mail : [email protected]

SH Hwang et al. Early-phase Emphysematous Acute Pancreatitis
82 Korean Journal of National Health Insurance Service Ilsan Hospital
his arrival; he was a chronic alcoholic and had drunk excessively in the past few days. Otherwise, he had no other specific medical history. At the time of his hos-pitalization, he showed signs of systemic inflammatory response syndrome (SIRS), tachycardia (pulse, 140/min), tachypnea (respiratory rate 24/min), and hypothermia (body temperature 35.3 ). His blood pressure was 94/64℃ mmHg. Blood test results indicated signs of acute pan-creatitis, diabetes, metabolic acidosis, and acute kid-ney injury and elevated levels of lipase (991 U/L), total bilirubin (3.80 mg/dL), CRP (6.20 mg/ml), BUN (18.4 mg/dL), Cr (2.17 mg/dL) and random glucose (512 mg/dL). His serum pH had decreased to 7.261, and his base excess was -18.2mmol/L. Non-enhanced CT showed acute pan-creatitis accompanied by extraluminal and intravascu-lar air at the superior mesenteric and portal veins (Fig. 1).
To differentiate between EP and peritonitis caused by bowel infarction and/or bowel perforation, follow- up contract-enhanced CT (CECT) was carried out two hours later. On the follow-up CT, there was intraductal air along the pancreatic duct, large amounts of air and fluid in the peripancreatic and retroperitoneal spaces,
and ascites. The pancreatic head was swollen, and its enhancement was slightly decreased without definite necrosis. There was no evidence of either bowel per-foration or infarction or intraperitoneal air on CECT (Fig. 2). Hence, EP was the most appropriate diagnosis for the patient considering the laboratory and imaging findings.
The patient was unable to undergo surgery because his vital signs were unstable. He was medicated with inotropic agents and antibiotics with hydration, and he was admitted to the intensive care unit (ICU). At the time of the ICU admission, his APACHE II score was 31 and his expected mortality was 73%.
Under the supportive management, he developed disseminated intravascular coagulation through septic shock. He died from respiratory and renal failure with-in 14 hours of his admission. After his death, the pa-tient’s blood culture results revealed gram-negative an-aerobes and aerobes. However, we did not identify any specific organisms because he had died.
DISCUSSION
EP is very rare acute pancreatitis that can be diag-nosed when pancreatic and/or peripancreatic air re-sulting from infection is found. Common causative or-ganisms are gram-negative anaerobes, such as E. coli, Pseudomonas aeruginosa, and K. pneumonia, as well as gram-positive pathogens, such as C. perfringens. The potential infection routes are hematogenous or lym-phatic spread, reflux of the enteric organism through the ampulla of Vater, and fistula with the adjacent bowel. Since the ACG published guidelines for manag-ing acute pancreatitis in 2013, conservative treatment has become more prevalent than traditional surgical treatment.1,2
The revised Atlanta classification of acute pancre-atitis in 2012 clarified the diagnostic criteria and de-fined two subtypes, interstitial edematous pancreatitis and necrotizing pancreatitis, with associated radiologic findings; acute pancreatitis was also divided into three
Fig. 1. Initial nonenhanced CT showed peripancreatic
fat haziness (arrow), multifocal extraluminal (open arrow),
intraductal, and intravascular air (asterisk) within superior
mesenteric vein
황신혜 외 초기 기종성 급성 췌장염.
Volume 18 Number 1 June 2019 83
categories according to disease severity also into early or late based on weeks from the time of onset.3
About 5-10% of acute pancreatitis patients have pancreatic and/or peripancreatic necrosis, and the ne-crosis can remain sterile or become infected. Infected necrosis rarely occurs within the first week, the early phase, of acute pancreatitis. Infected pancreatic ne-crosis (IPN) can be diagnosed when gas appears in pancreatic and/or peripancreatic tissue on an imaging study or when the patient is positive for bacteria on Gram stain and culture in a fine-needle aspiration.3
According to the revised Atlanta classification, pre-viously reported successful cases of conservative and/ or percutaneous interventional treatment of EP were among patients in whom emphysema developed in late acute pancreatitis as a local complication and that was the emphysematous form of IPN. These patients were
stable during their treatment. Furthermore, it has been reported that there is no difference in clinical course and prognosis between emphysematous and non-em-physematous IPN.4
On the contrary, within a few hours of acute pan-creatitis onset (early phase), our patient showed large amounts of air and fluid in his pancreatic and peri-pancreatic tissue on CECT, although the presence of necrosis was unclear. The patient’s condition rapidly deteriorated through SIRS and multi-organ failure, leading to his death through a fulminant course. There have been a few similar reported cases in which pa-tients showed gas formation in the early phase of acute pancreatitis and either died through clinically grave courses or had their lives saved through early surgical treatment.5-8 Of them, two patients had history of dia-betics mellitus and a patient had a history of chronic
(A) (B)
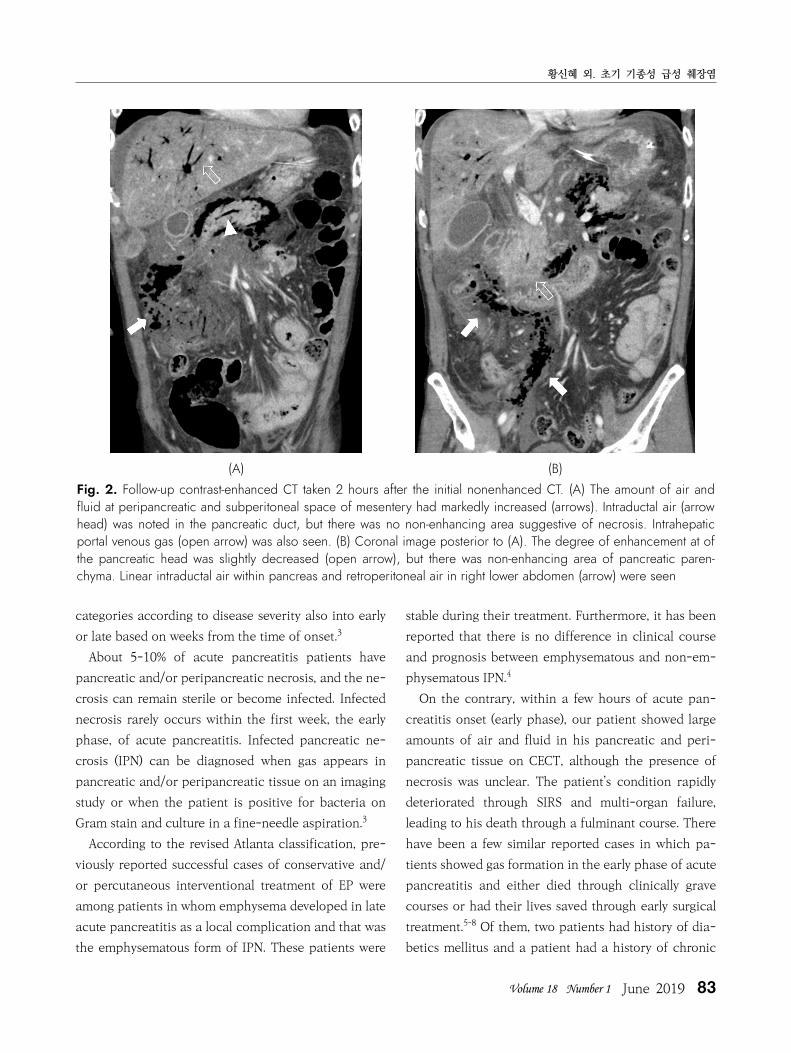
Fig. 2. Follow-up contrast-enhanced CT taken 2 hours after the initial nonenhanced CT. (A) The amount of air and
fluid at peripancreatic and subperitoneal space of mesentery had markedly increased (arrows). Intraductal air (arrow
head) was noted in the pancreatic duct, but there was no non-enhancing area suggestive of necrosis. Intrahepatic
portal venous gas (open arrow) was also seen. (B) Coronal image posterior to (A). The degree of enhancement at of
the pancreatic head was slightly decreased (open arrow), but there was non-enhancing area of pancreatic paren-
chyma. Linear intraductal air within pancreas and retroperitoneal air in right lower abdomen (arrow) were seen

SH Hwang et al. Early-phase Emphysematous Acute Pancreatitis
84 Korean Journal of National Health Insurance Service Ilsan Hospital
renal disease. However, others including our patient did not have any medical history. Therefore, there is still a question regarding whether intensive medical care or conservative treatment is more appropriate for such cases if the patient can withstand surgery, which was not the case with our patient.
Early phase EP, which shows pancreatic and/or peri-pancreatic gas formation within few hours or days from the onset of acute pancreatitis while necrotic change is little or absent, is severe pancreatitis accom-panied by organ failure, and it often leads to a fatal course. Thus, it seems to be differentiated from late phase EP (emphysematous IPN), which shows air and well-demarcated necrosis in the late phase and a grad-ual and stable clinical course, as well as good out-comes with conservative treatment. Early-phase EP ne-cessitates more proactive treatments such as early nonsurgical drainage and/or necrosectomy. Further re-search on treatment strategies for early-phase EP is required.
REFERENCES
1. Bul V, Yazici C, Staudacher JJ, Jung B, Boulay BR.
Multiorgan Failure Predicts Mortality in Emphysem-atous Pancreatitis: A Case Report and Systematic Analysis of the Literature. Pancreas 2017;46:825-30.
2. Tenner S, Baillie J, DeWitt J, Vege SS. American College of Gastroenterology guideline: management of acute pancreatitis. Am J Gastroenterol 2013;108: 1400-15; 16.
3. Banks PA, Bollen TL, Dervenis C, Gooszen HG, Johnson CD, Sarr MG, Tsiotos GG, Vege SS. Classification of acute pancreatitis--2012: revision of the Atlanta clas-sification and definitions by international consensus. Gut 2013;62:102-11.
4. Wig JD, Kochhar R, Bharathy KG, Kudari AK, Doley RP, Yadav TD, Kalra N. Emphysematous pancreatitis. Radiological curiosity or a cause for concern? Jop 2008;9:160-6.
5. De Silva NM, Windsor JA. Clostridium perfringens in-fection of pancreatic necrosis: absolute indication for early surgical intervention. ANZ J Surg 2006;76:757-9.
6. Komatsu H, Yoshida H, Hayashi H, Sakata N, Morikawa T, Onogawa T, Motoi F, Rikiyama T, Katayose Y, Egawa S, Hirota M, Shimosegawa T, Unno M. Fulminant type of emphysematous pancreatitis has risk of massive hemorrhage. Clin J Gastroenterol 2011;4:249-54.
7. Porter NA, Lapsia SK. Emphysematous pancreatitis: a severe complication of acute pancreatitis. Qjm 2011; 104:897.
8. Balani A, Dey AK, Sarjare S, Chatur C. Emphysematous pancreatitis: classic findings. BMJ Case Reports. 2016; Dec 15.