inhibidores de proteasa vs inhibidores de integrasasogaisida.org/files/congreso9/mesa2_008.pdf ·...
TRANSCRIPT

Inhibidores de proteasa vs inhibidores de integrasa
Raúl Rodríguez CHUOU. Lugo 19 Oct 2019
9º Congreso SOGAISIDA

Eficacia
Resistencias
TolerabilidadInteracciones
ComodidadTAR
SUPERIORIDAD: más allá de la eficacia virológica
Argumentos para el uso de INI vs Ips
• 1- Eficacia
• 2- Tolerabilidad
• 3- Perfil de interacciones
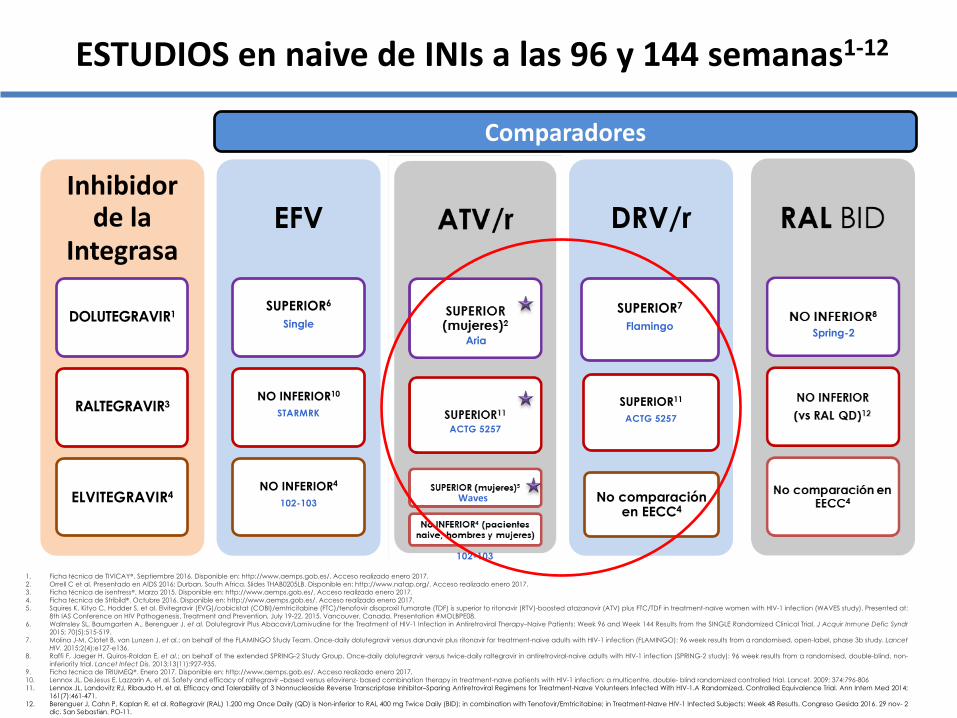
Inhibidor de la
Integrasa
DOLUTEGRAVIR1
RALTEGRAVIR3
ELVITEGRAVIR4
EFV
SUPERIOR6
Single
NO INFERIOR10
STARMRK
NO INFERIOR4
102-103
RAL BID
NO INFERIOR8
NO INFERIOR (vs RAL QD)12
No comparación en EECC4
DRV/r
SUPERIOR7
Flamingo
SUPERIOR11
ACTG 5257
No comparación en EECC4
ATV/r
SUPERIOR (mujeres)2
SUPERIOR11
SUPERIOR (mujeres)5
No INFERIOR4 (pacientes naive, hombres y mujeres)
1. Ficha técnica de TIVICAY®. Septiembre 2016. Disponible en: http://www.aemps.gob.es/. Acceso realizado enero 2017.2. Orrell C et al. Presentado en AIDS 2016; Durban, South Africa. Slides THAB0205LB. Disponible en: http://www.natap.org/. Acceso realizado enero 2017.3. Ficha técnica de isentress®. Marzo 2015. Disponible en: http://www.aemps.gob.es/. Acceso realizado enero 2017.4. Ficha técnica de Stribild®. Octubre 2016. Disponible en: http://www.aemps.gob.es/. Acceso realizado enero 2017.5. Squires K, Kityo C, Hodder S, et al. Elvitegravir (EVG)/cobicistat (COBI)/emtricitabine (FTC)/tenofovir disoproxil fumarate (TDF) is superior to ritonavir (RTV)-boosted atazanavir (ATV) plus FTC/TDF in treatment-naïve women with HIV-1 infection (WAVES study). Presented at:
8th IAS Conference on HIV Pathogenesis, Treatment and Prevention, July 19-22, 2015. Vancouver, Canada. Presentation #MOLBPE08.6. Walmsley SL, Baumgarten A., Berenguer J, et al. Dolutegravir Plus Abacavir/Lamivudine for the Treatment of HIV-1 Infection in Antiretroviral Therapy–Naive Patients: Week 96 and Week 144 Results from the SINGLE Randomized Clinical Trial. J Acquir Inmune Defic Syndr
2015; 70(5):515-519.7. Molina J-M, Clotet B, van Lunzen J, et al.; on behalf of the FLAMINGO Study Team. Once-daily dolutegravir versus darunavir plus ritonavir for treatment-naive adults with HIV-1 infection (FLAMINGO): 96 week results from a randomised, open-label, phase 3b study. Lancet
HIV. 2015;2(4):e127-e136.8. Raffi F, Jaeger H, Quiros-Roldan E, et al.; on behalf of the extended SPRING-2 Study Group. Once-daily dolutegravir versus twice-daily raltegravir in antiretroviral-naive adults with HIV-1 infection (SPRING-2 study): 96 week results from a randomised, double-blind, non-
inferiority trial. Lancet Infect Dis. 2013;13(11):927-935.9. Ficha técnica de TRIUMEQ®. Enero 2017. Disponible en: http://www.aemps.gob.es/. Acceso realizado enero 2017.10. Lennox JL, DeJesus E, Lazzarin A, et al. Safety and efficacy of raltegravir –based versus efavirenz- based combination therapy in treatment-naïve patients with HIV-1 infection: a multicentre, double- blind randomized controlled trial. Lancet. 2009; 374:796-80611. Lennox JL, Landovitz RJ, Ribaudo H, et al. Efficacy and Tolerability of 3 Nonnucleoside Reverse Transcriptase Inhibitor–Sparing Antiretroviral Regimens for Treatment-Naïve Volunteers Infected With HIV-1.A Randomized, Controlled Equivalence Trial. Ann Intern Med 2014;
161(7):461-471.12. Berenguer J, Cahn P, Kaplan R, et al. Raltegravir (RAL) 1.200 mg Once Daily (QD) is Non-inferior to RAL 400 mg Twice Daily (BID); in combination with Tenofovir/Emtricitabine; in Treatment-Naïve HIV-1 Infected Subjects: Week 48 Results. Congreso Gesida 2016. 29 nov- 2
dic. San Sebastián. PO-11.
Comparadores
ESTUDIOS en naive de INIs a las 96 y 144 semanas1-12
AriaSpring-2
ACTG 5257
Waves
102-103
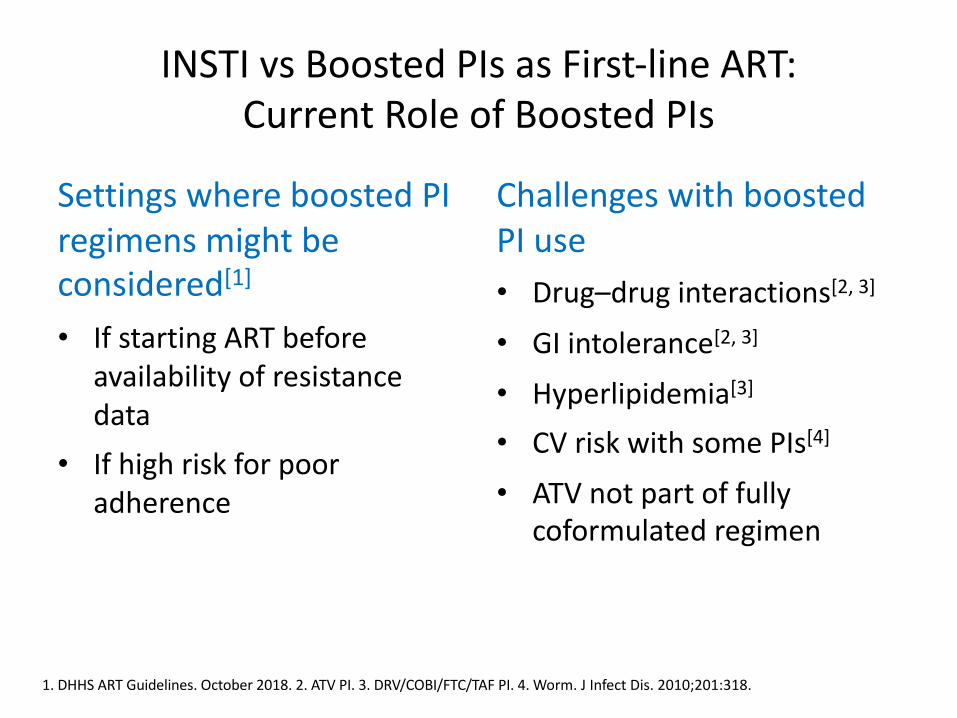
INSTI vs Boosted PIs as First-line ART:
Current Role of Boosted PIs
Settings where boosted PI
regimens might be considered[1]
• If starting ART before
availability of resistance
data
• If high risk for poor
adherence
Challenges with boosted
PI use
• Drug–drug interactions[2, 3]
• GI intolerance[2, 3]
• Hyperlipidemia[3]
• CV risk with some PIs[4]
• ATV not part of fully coformulated regimen
1. DHHS ART Guidelines. October 2018. 2. ATV PI. 3. DRV/COBI/FTC/TAF PI. 4. Worm. J Infect Dis. 2010;201:318.
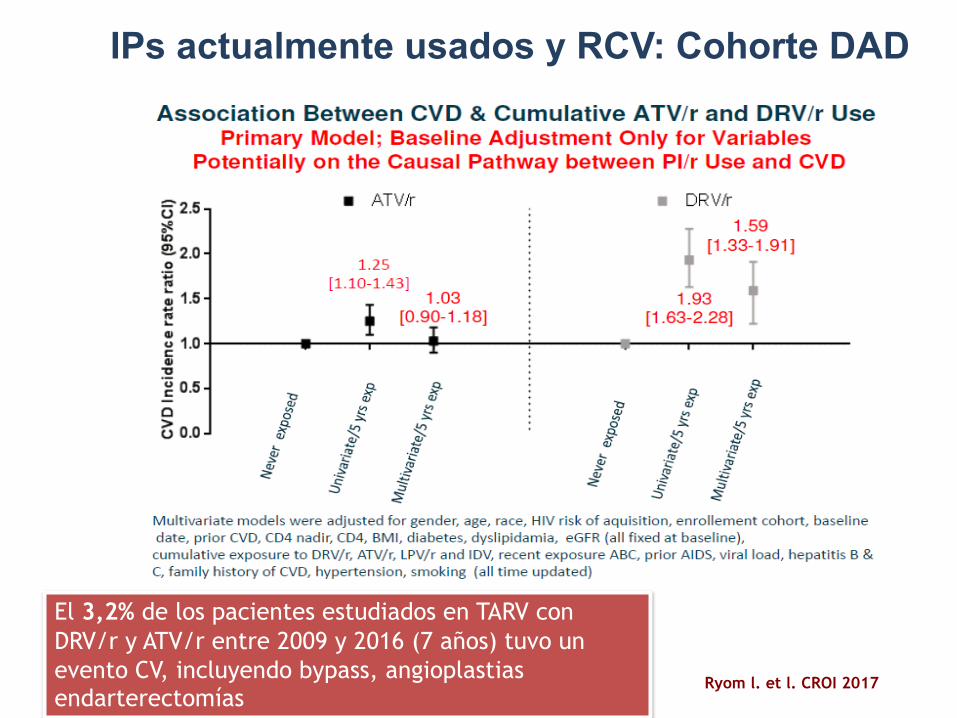
El 3,2% de los pacientes estudiados en TARV con DRV/r y ATV/r entre 2009 y 2016 (7 años) tuvo un evento CV, incluyendo bypass, angioplastias endarterectomías
Ryom l. et l. CROI 2017
IPs actualmente usados y RCV: Cohorte DAD
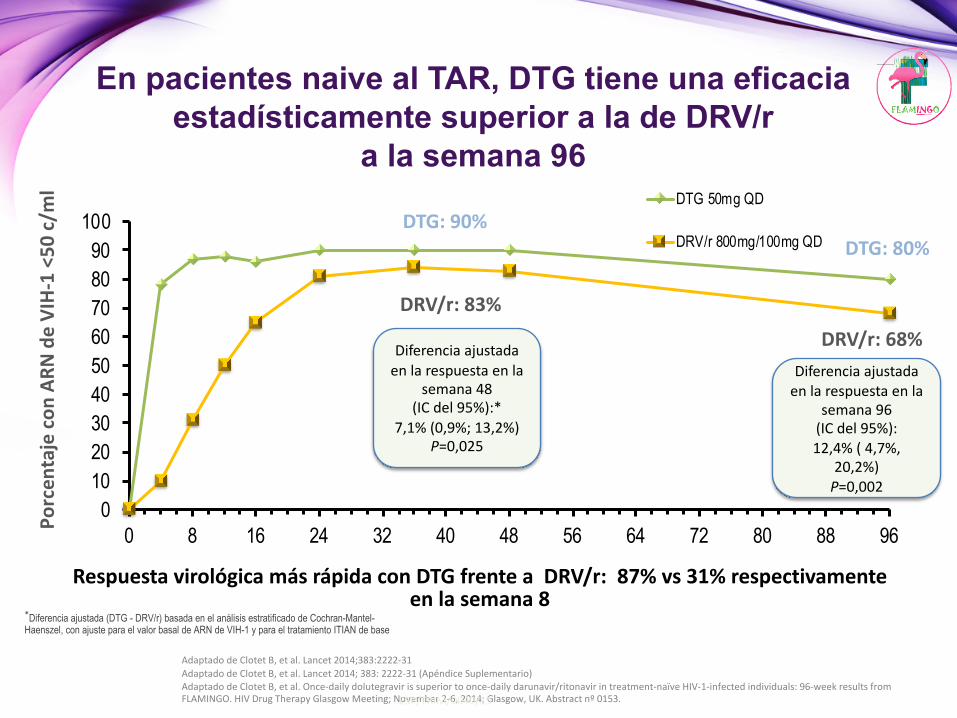
En pacientes naive al TAR, DTG tiene una eficacia estadísticamente superior a la de DRV/r
a la semana 96
Adaptado de Clotet B, et al. Lancet 2014;383:2222-31Adaptado de Clotet B, et al. Lancet 2014; 383: 2222-31 (Apéndice Suplementario)Adaptado de Clotet B, et al. Once-daily dolutegravir is superior to once-daily darunavir/ritonavir in treatment-naïve HIV-1-infected individuals: 96-week results fromFLAMINGO. HIV Drug Therapy Glasgow Meeting; November 2-6, 2014; Glasgow, UK. Abstract nº 0153.
DRV/r: 83%
DTG: 90%DTG: 80%
DRV/r: 68%Diferencia ajustada
en la respuesta en la semana 48
(IC del 95%):* 7,1% (0,9%; 13,2%)
P=0,025
Diferencia ajustadaen la respuesta en la
semana 96 (IC del 95%):12,4% ( 4,7%,
20,2%)P=0,002
Respuesta virológica más rápida con DTG frente a DRV/r: 87% vs 31% respectivamenteen la semana 8
Porc
enta
je c
on A
RN d
e VI
H-1
<50
c/m
l
*Diferencia ajustada (DTG - DRV/r) basada en el análisis estratificado de Cochran-Mantel-Haenszel, con ajuste para el valor basal de ARN de VIH-1 y para el tratamiento ITIAN de base
0102030405060708090
100
0 8 16 24 32 40 48 56 64 72 80 88 96
DTG 50mg QD
DRV/r 800mg/100mg QD
ESP/TRIM/0040/15
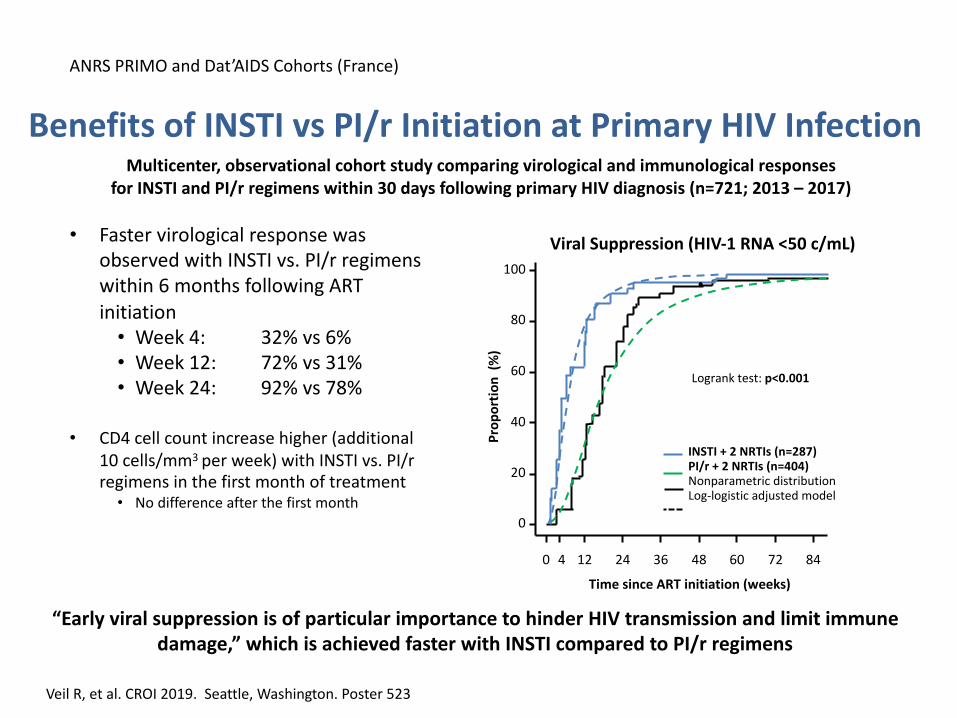
Benefits of INSTI vs PI/r Initiation at Primary HIV InfectionMulticenter, observational cohort study comparing virological and immunological responses
for INSTI and PI/r regimens within 30 days following primary HIV diagnosis (n=721; 2013 – 2017)
Veil R, et al. CROI 2019. Seattle, Washington. Poster 523
“Early viral suppression is of particular importance to hinder HIV transmission and limit immune
damage,” which is achieved faster with INSTI compared to PI/r regimens
Viral Suppression (HIV-1 RNA <50 c/mL)
Pro
po
rtio
n (
%)
Time since ART initiation (weeks)
0 12 24 36 48 60 72 84
0
20
40
60
80
100
Logrank test: p<0.001
INSTI + 2 NRTIs (n=287)PI/r + 2 NRTIs (n=404)Nonparametric distributionLog-logistic adjusted model
ANRS PRIMO and Dat’AIDS Cohorts (France)
• Faster virological response was observed with INSTI vs. PI/r regimens within 6 months following ART initiation• Week 4: 32% vs 6%• Week 12: 72% vs 31%• Week 24: 92% vs 78%
• CD4 cell count increase higher (additional 10 cells/mm3 per week) with INSTI vs. PI/r regimens in the first month of treatment• No difference after the first month
4
Argumentos para el uso de INI vs Ips
• 1- Eficacia
• 2- Tolerabilidad
• 3- Perfil de interacciones
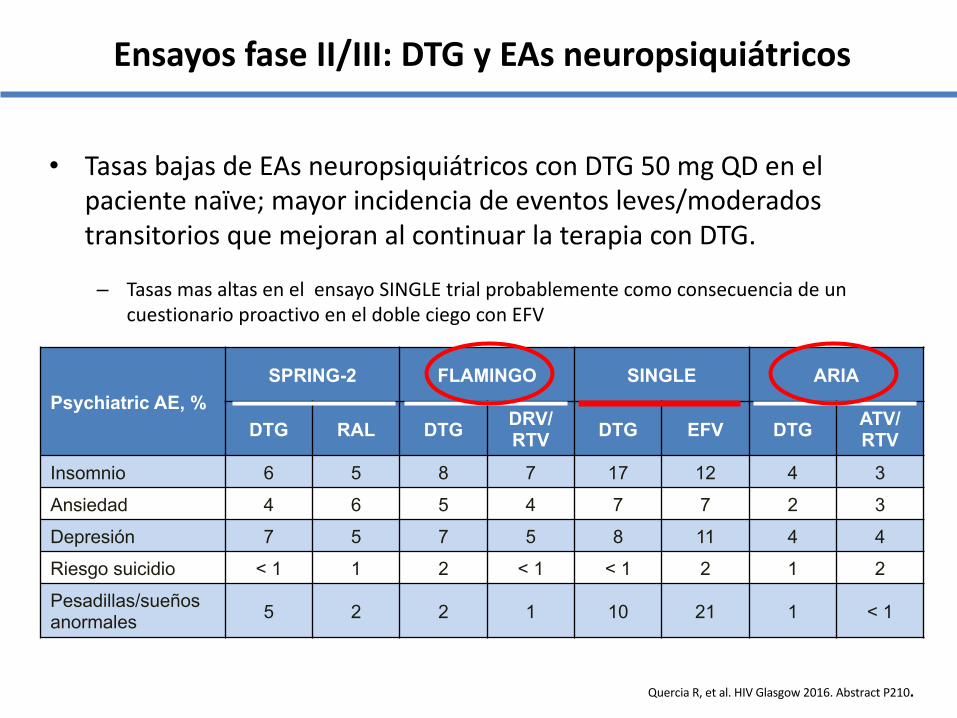
• Tasas bajas de EAs neuropsiquiátricos con DTG 50 mg QD en el paciente naïve; mayor incidencia de eventos leves/moderadostransitorios que mejoran al continuar la terapia con DTG.
– Tasas mas altas en el ensayo SINGLE trial probablemente como consecuencia de un cuestionario proactivo en el doble ciego con EFV
Quercia R, et al. HIV Glasgow 2016. Abstract P210.
Psychiatric AE, %SPRING-2 FLAMINGO SINGLE ARIA
DTG RAL DTG DRV/ RTV DTG EFV DTG ATV/
RTVInsomnio 6 5 8 7 17 12 4 3
Ansiedad 4 6 5 4 7 7 2 3
Depresión 7 5 7 5 8 11 4 4
Riesgo suicidio < 1 1 2 < 1 < 1 2 1 2
Pesadillas/sueñosanormales 5 2 2 1 10 21 1 < 1
Ensayos fase II/III: DTG y EAs neuropsiquiátricos
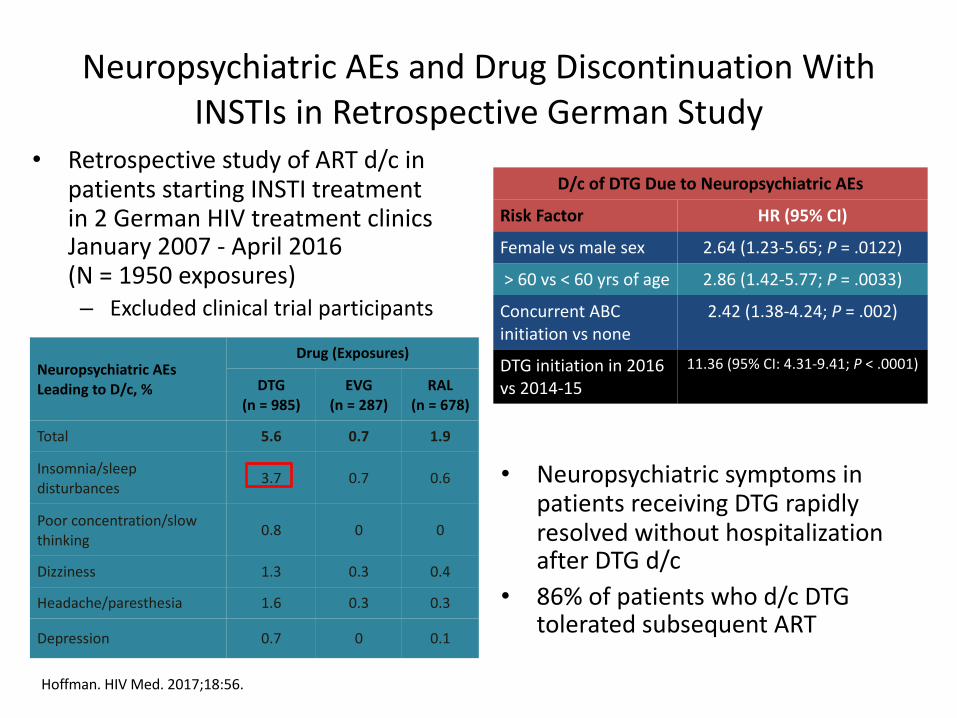
• Neuropsychiatric symptoms in patients receiving DTG rapidly resolved without hospitalization after DTG d/c
• 86% of patients who d/c DTG tolerated subsequent ART
Neuropsychiatric AEs and Drug Discontinuation With INSTIs in Retrospective German Study
• Retrospective study of ART d/c in patients starting INSTI treatment in 2 German HIV treatment clinics January 2007 - April 2016 (N = 1950 exposures)– Excluded clinical trial participants
Neuropsychiatric AEs Leading to D/c, %
Drug (Exposures)
DTG(n = 985)
EVG(n = 287)
RAL(n = 678)
Total 5.6 0.7 1.9
Insomnia/sleep disturbances 3.7 0.7 0.6
Poor concentration/slow thinking 0.8 0 0
Dizziness 1.3 0.3 0.4
Headache/paresthesia 1.6 0.3 0.3
Depression 0.7 0 0.1
Hoffman. HIV Med. 2017;18:56.
D/c of DTG Due to Neuropsychiatric AEs
Risk Factor HR (95% CI)
Female vs male sex 2.64 (1.23-5.65; P = .0122)
> 60 vs < 60 yrs of age 2.86 (1.42-5.77; P = .0033)
Concurrent ABC initiation vs none
2.42 (1.38-4.24; P = .002)
DTG initiation in 2016 vs 2014-15
11.36 (95% CI: 4.31-9.41; P < .0001)
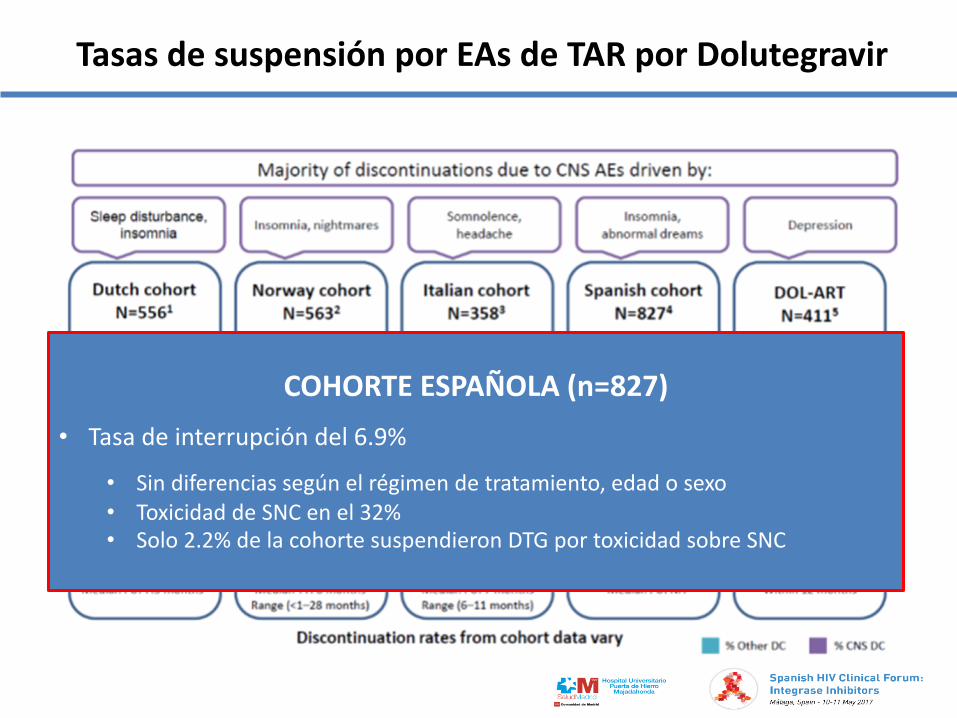
Tasas de suspensión por EAs de TAR por Dolutegravir
COHORTE ESPAÑOLA (n=827)• Tasa de interrupción del 6.9%
• Sin diferencias según el régimen de tratamiento, edad o sexo• Toxicidad de SNC en el 32%• Solo 2.2% de la cohorte suspendieron DTG por toxicidad sobre SNC
Argumentos para el uso de INI vs Ips
• 1- Eficacia
• 2- Tolerabilidad
• 3- Perfil de interacciones
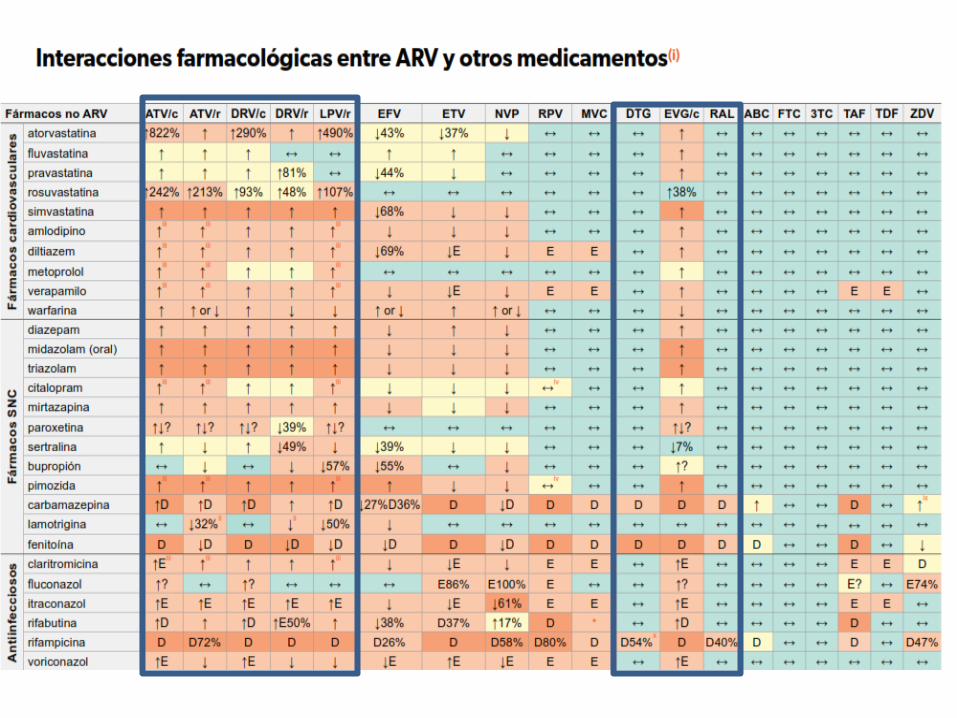
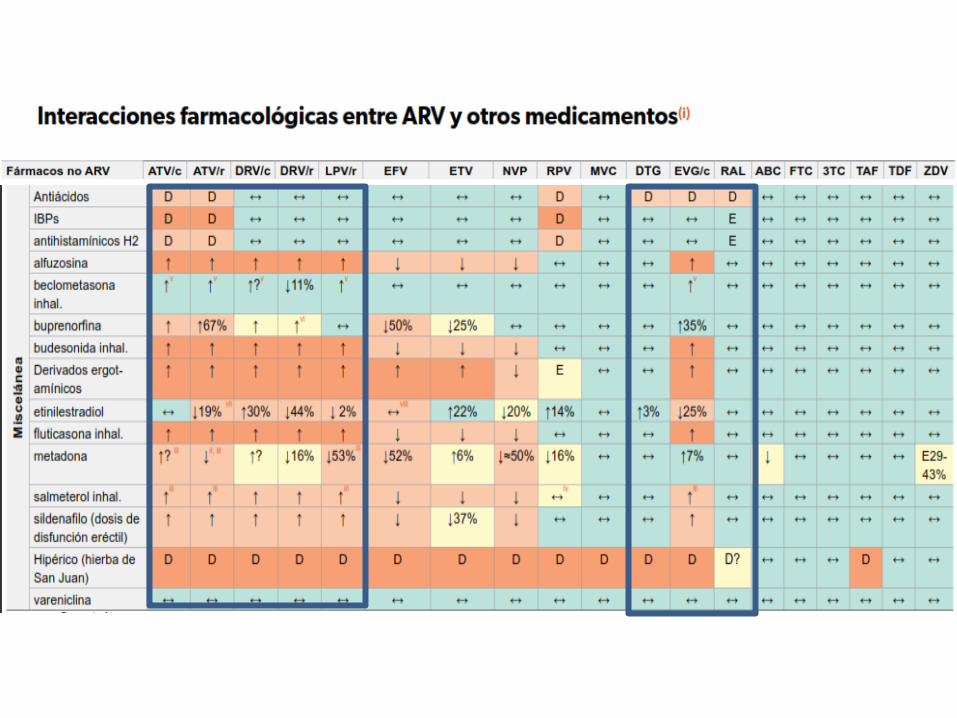
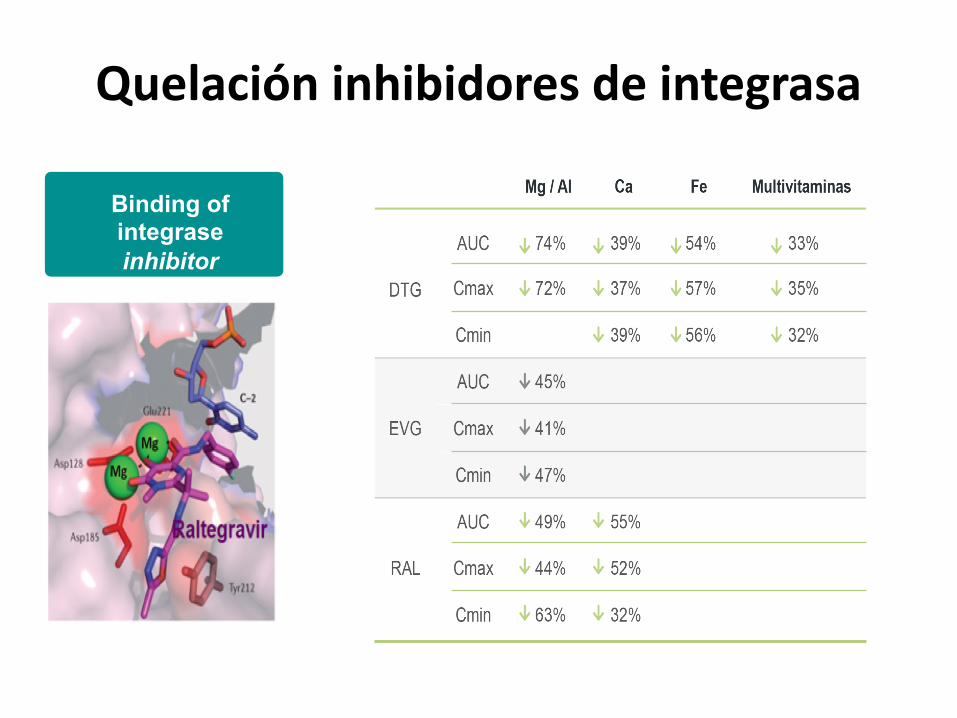
Quelación inhibidores de integrasa
Binding of integrase inhibitor
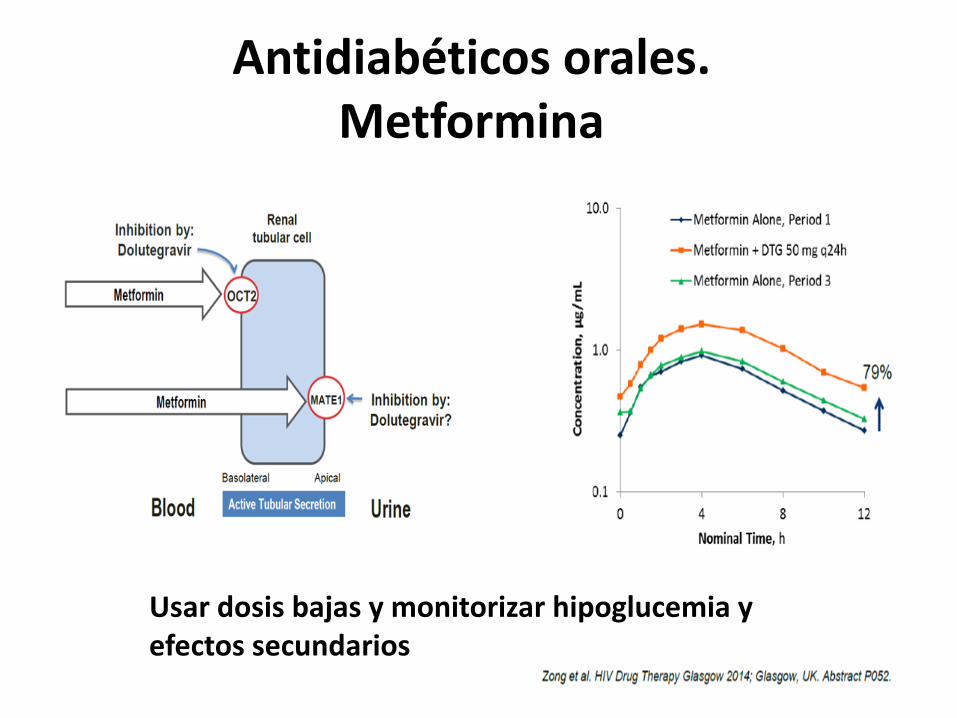
Antidiabéticos orales. Metformina
Usar dosis bajas y monitorizar hipoglucemia y efectos secundarios
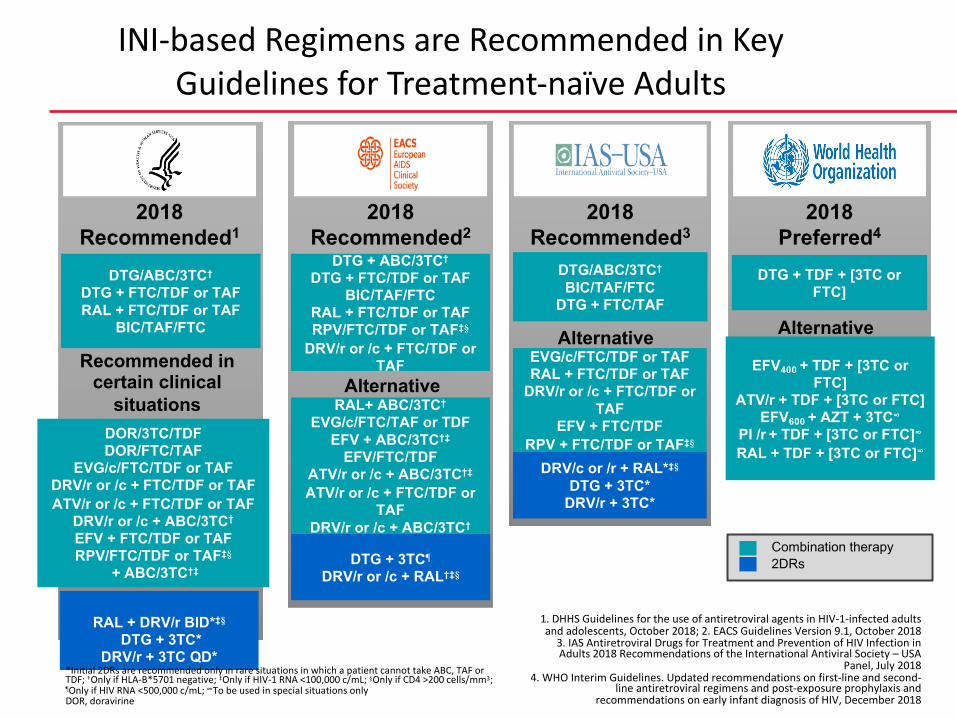
INIs recomendados en todas las guías como preferente
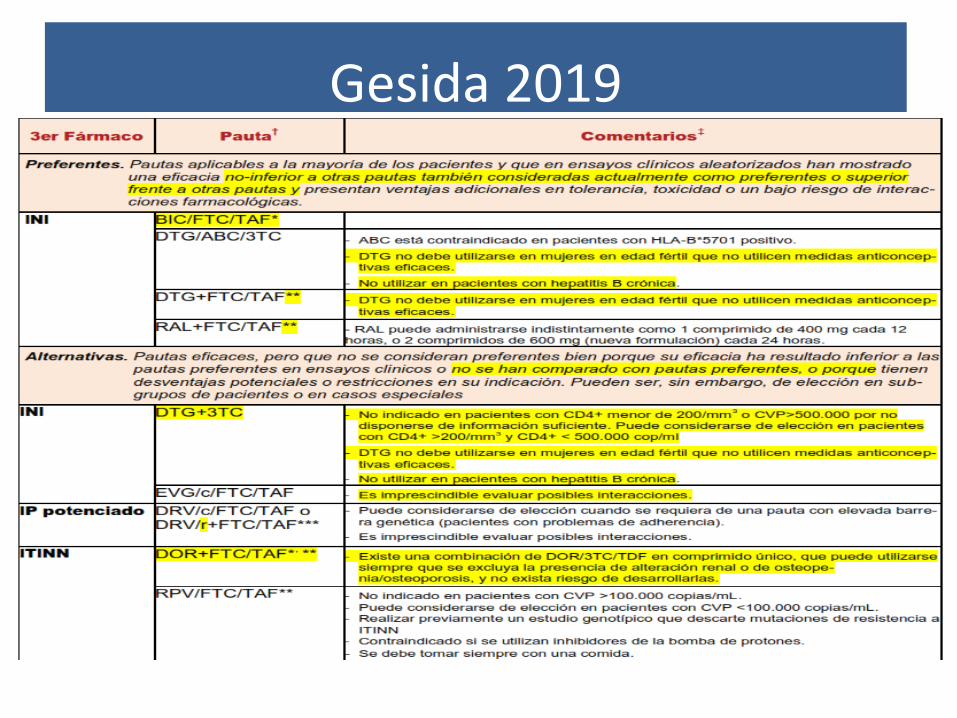
Gesida 2019
DTG + 3TC¶
DRV/r or /c + RAL†‡§
Recommended in certain clinical
situations
RAL + DRV/r BID*‡§
DTG + 3TC*DRV/r + 3TC QD*
DRV/c or /r + RAL*‡§
DTG + 3TC*DRV/r + 3TC*
Alternative
2018Recommended1
DTG/ABC/3TC†
DTG + FTC/TDF or TAFRAL + FTC/TDF or TAF
BIC/TAF/FTC
2018Recommended3
DTG/ABC/3TC†
BIC/TAF/FTCDTG + FTC/TAF
2018Recommended2
DTG + ABC/3TC†
DTG + FTC/TDF or TAFBIC/TAF/FTC
RAL + FTC/TDF or TAFRPV/FTC/TDF or TAF‡§
DRV/r or /c + FTC/TDF orTAF
Alternative
2018Preferred4
DTG + TDF + [3TC or FTC]
EFV400 + TDF + [3TC or FTC]
ATV/r + TDF + [3TC or FTC]EFV600 + AZT + 3TC∞
PI /r + TDF + [3TC or FTC]∞
RAL + TDF + [3TC or FTC]∞
Combination therapy2DRs
DOR/3TC/TDFDOR/FTC/TAF
EVG/c/FTC/TDF or TAFDRV/r or /c + FTC/TDF or TAFATV/r or /c + FTC/TDF or TAF
DRV/r or /c + ABC/3TC†
EFV + FTC/TDF or TAFRPV/FTC/TDF or TAF‡§
+ ABC/3TC†‡
RAL+ ABC/3TC†
EVG/c/FTC/TAF or TDF EFV + ABC/3TC†‡
EFV/FTC/TDFATV/r or /c + ABC/3TC†‡
ATV/r or /c + FTC/TDF orTAF
DRV/r or /c + ABC/3TC†
Alternative
INI-based Regimens are Recommended in Key
Guidelines for Treatment-naïve Adults
1. DHHS Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents, October 2018; 2. EACS Guidelines Version 9.1, October 2018
3. IAS Antiretroviral Drugs for Treatment and Prevention of HIV Infection in Adults 2018 Recommendations of the International Antiviral Society – USA
Panel, July 20184. WHO Interim Guidelines. Updated recommendations on first-line and second-
line antiretroviral regimens and post-exposure prophylaxis and recommendations on early infant diagnosis of HIV, December 2018
*Initial 2DRs are recommended only in rare situations in which a patient cannot take ABC, TAF or TDF; †Only if HLA-B*5701 negative; ‡Only if HIV-1 RNA <100,000 c/mL; §Only if CD4 >200 cells/mm3; ¶Only if HIV RNA <500,000 c/mL; ∞To be used in special situations onlyDOR, doravirine
EVG/c/FTC/TDF or TAF RAL + FTC/TDF or TAF
DRV/r or /c + FTC/TDF orTAF
EFV + FTC/TDFRPV + FTC/TDF or TAF‡§
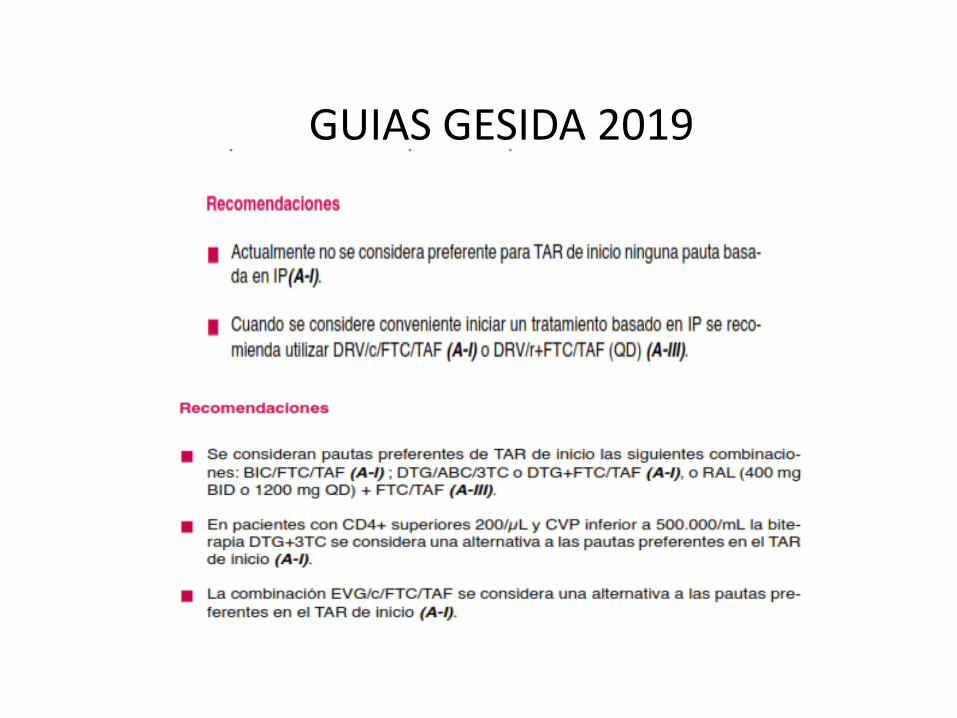
GUIAS GESIDA 2019
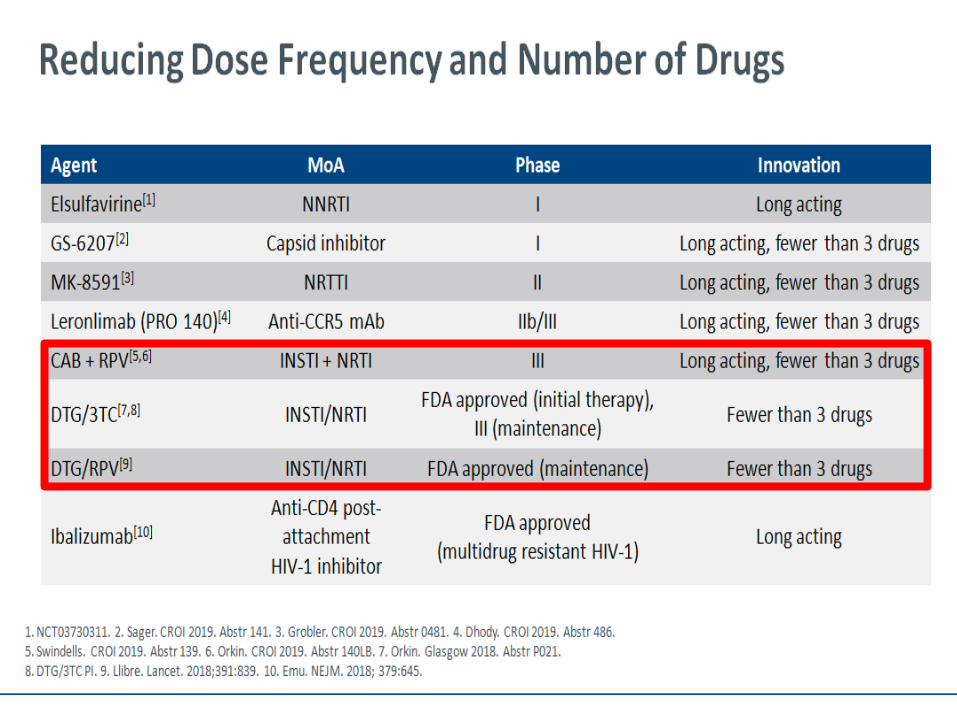
Posibilidad de terapia dual / LA en FT en naive
Conclusiones• Los INI son fármacos que alcanzan superioridad frente a Ips
en naives, en todos los estudios• Son los preferidos en las guias nacionales e internacionales de
tratamiento de la infección por vih• Tienen un excelente perfil de interacciones y buena
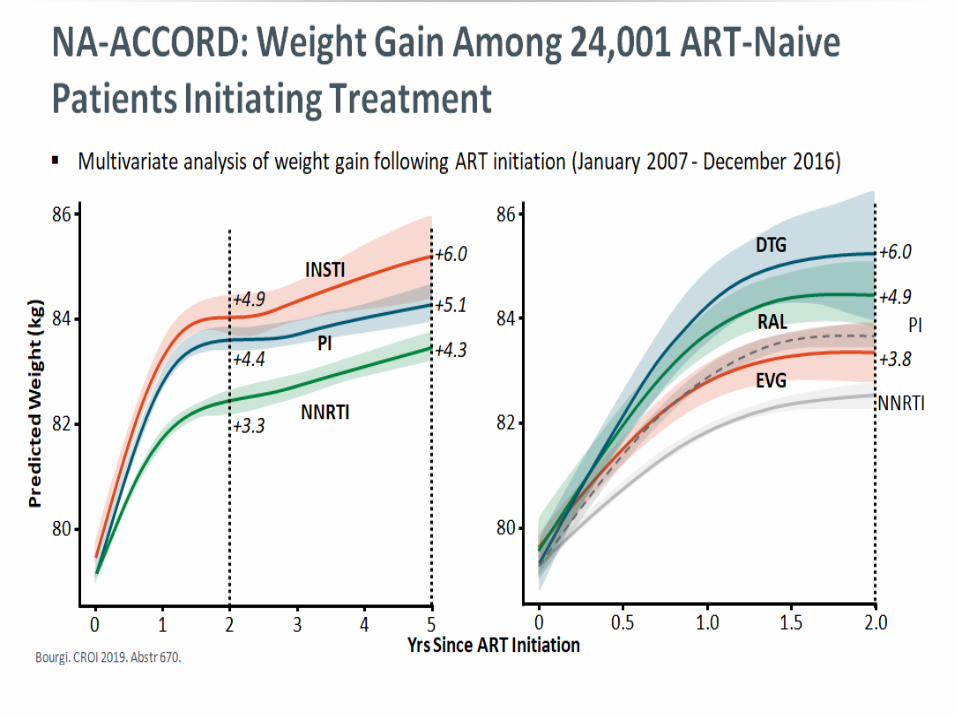
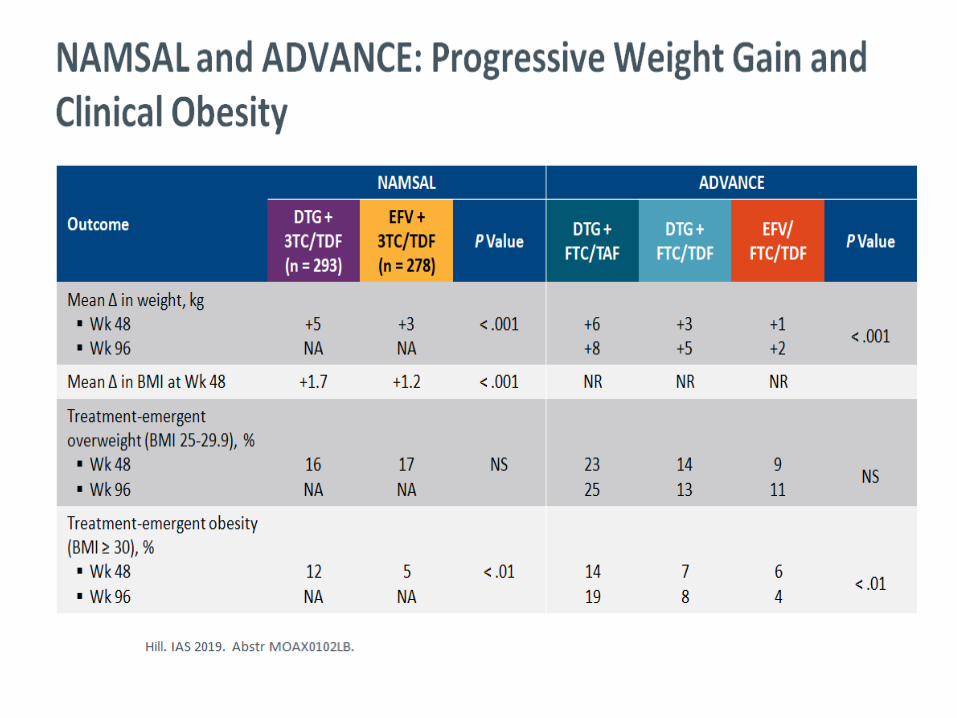
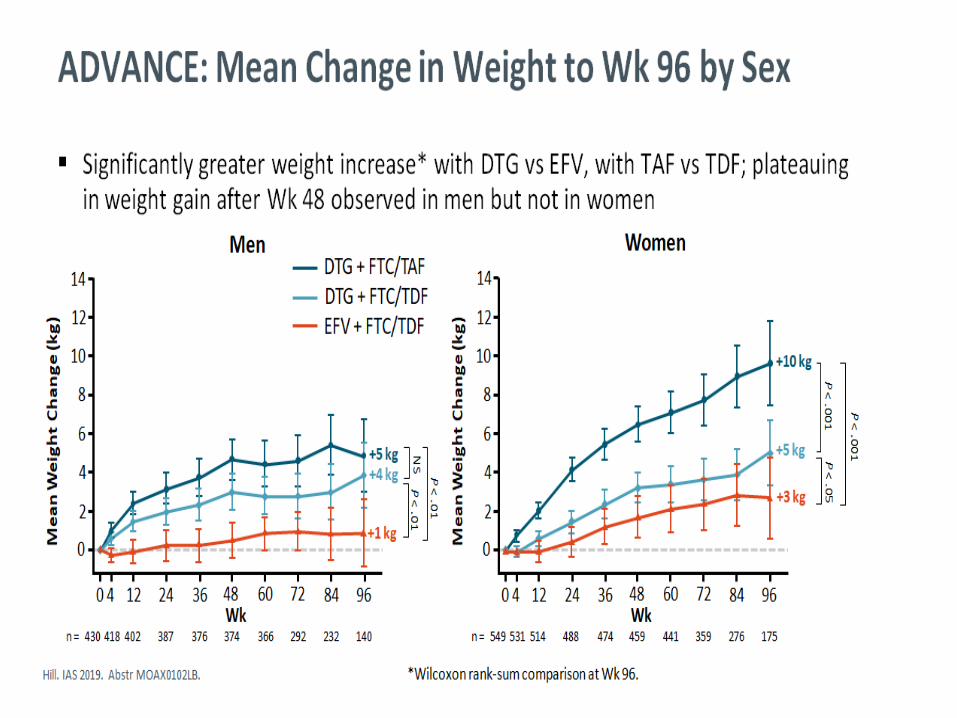
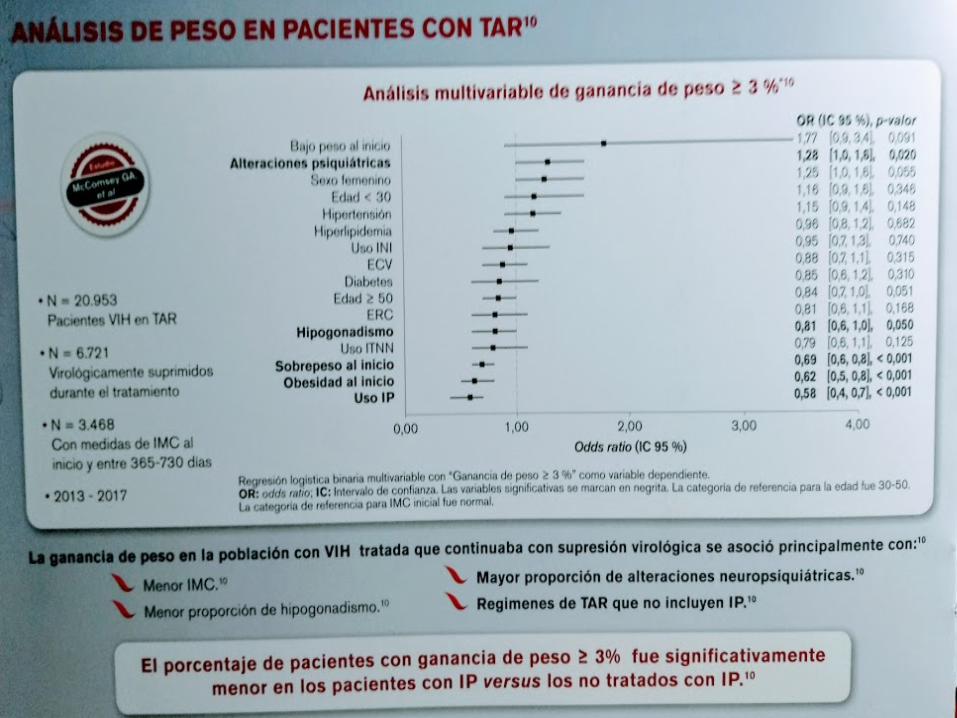
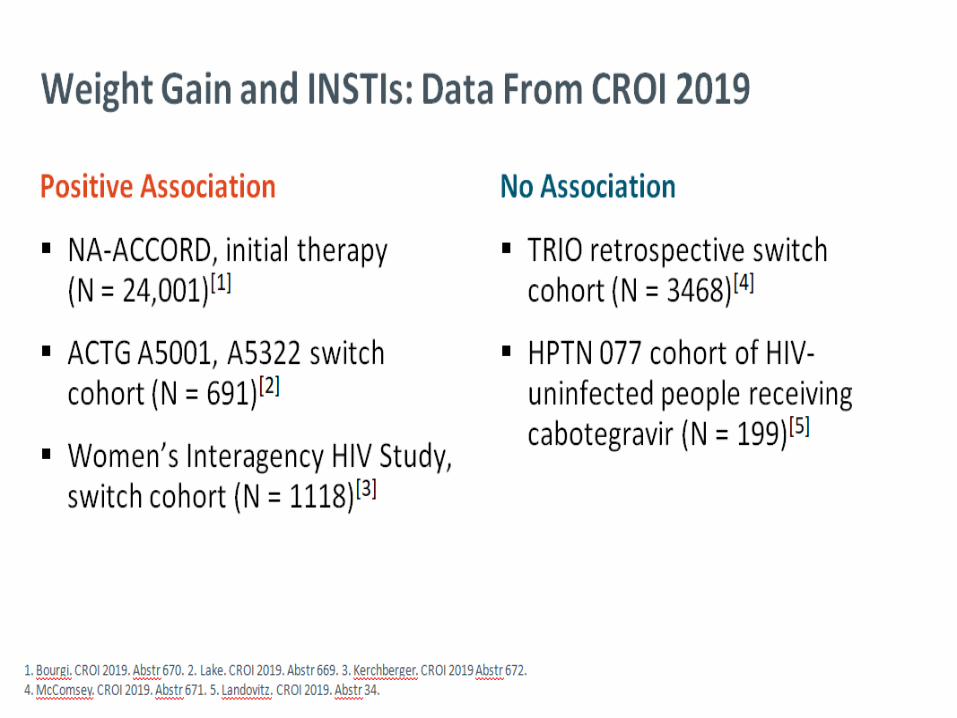
tolerancia con escasas retiradas por EA, a valorar en el futuro la ganancia ponderal y el papel de TAF
• Son fármacos que forman y formarán parte de las nuevas estrategias de tratamiento de futuro, como terapia dual y terapia LA

GRACIAS !!