jig's microbiology
DESCRIPTION
Jig's MicrobiologyTRANSCRIPT
Lecture 1: Virus properties1) Describe the nature of viruses: their small size, unique mode of replication and diversity. Viruses are small in size varying from 20 – 450 nm.(the largest virus is still smaller than the smallest bacteria) They are obligate intracellular parasites, composed of nucleic acid, protein and sometimes lipid and carbohydrates Virus replication is unique:
- binding to the host cell- can be a very specific interaction between virus surface proteins and cell receptors- penetration:
o enveloped: fusion of virus and cell membranes (HIV,, Measles, Influenza) o non-enveloped: disruption of host cell membrane integrity, genome or core crosses into cytosol
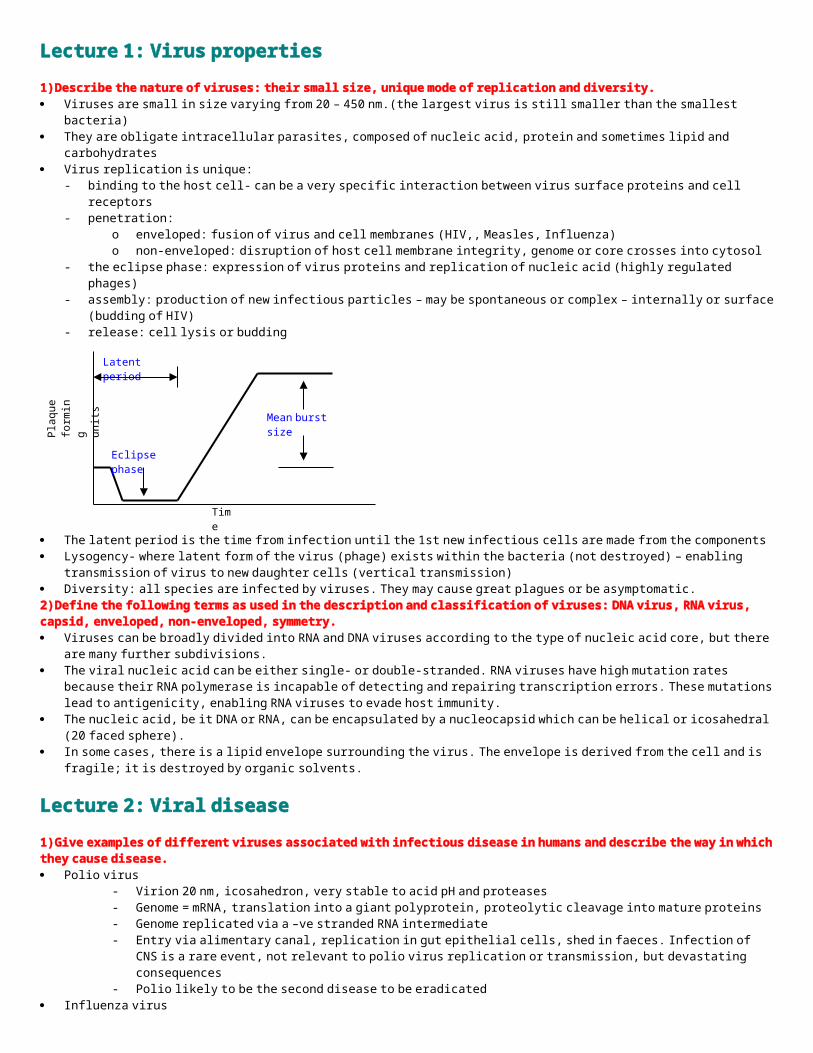
- the eclipse phase: expression of virus proteins and replication of nucleic acid (highly regulated phages)- assembly: production of new infectious particles – may be spontaneous or complex – internally or surface (budding of HIV)- release: cell lysis or budding
The latent period is the time from infection until the 1st new infectious cells are made from the components Lysogency- where latent form of the virus (phage) exists within the bacteria (not destroyed) – enabling transmission of virus to new
daughter cells (vertical transmission) Diversity: all species are infected by viruses. They may cause great plagues or be asymptomatic.2) Define the following terms as used in the description and classification of viruses: DNA virus, RNA virus, capsid, enveloped, non-enveloped, symmetry. Viruses can be broadly divided into RNA and DNA viruses according to the type of nucleic acid core, but there are many further
subdivisions. The viral nucleic acid can be either single- or double-stranded. RNA viruses have high mutation rates because their RNA polymerase
is incapable of detecting and repairing transcription errors. These mutations lead to antigenicity, enabling RNA viruses to evade host immunity.
The nucleic acid, be it DNA or RNA, can be encapsulated by a nucleocapsid which can be helical or icosahedral (20 faced sphere). In some cases, there is a lipid envelope surrounding the virus. The envelope is derived from the cell and is fragile; it is destroyed by
organic solvents.
Lecture 2: Viral disease1) Give examples of different viruses associated with infectious disease in humans and describe the way in which they cause disease. Polio virus
- Virion 20 nm, icosahedron, very stable to acid pH and proteases- Genome = mRNA, translation into a giant polyprotein, proteolytic cleavage into mature proteins- Genome replicated via a –ve stranded RNA intermediate- Entry via alimentary canal, replication in gut epithelial cells, shed in faeces. Infection of CNS is a rare event, not relevant
to polio virus replication or transmission, but devastating consequences- Polio likely to be the second disease to be eradicated
Influenza virus- Virion enveloped, 100nm, contains helical nucleocapsid- ss –ve polarity genome, 8 segments, 13.6 kb- Genome transcribed into mRNAs by virus-encoded RNA-dependent RNA polymerase and replicated via +ve sense
cRNA intermediate- Influenza causes new epidemics because:- Virus undergoes antigenic variation (antigenic shift/drift)- Existing immunity is of limited value against the new strains- Antigenic shift – when a human and an avian virus co infect a cell and undergo reassortment resulting in a new strain of
virus.- Antigenic drift – this is as a result of the accumulation of point mutations but produces less dramatic epidemics that
antigenic shift. HIV
- AIDS caused by a retrovirus isolated in 1983 (human immunodeficiency virus)- No vaccine, no cure once infected, without drugs death is the outcome- Retrovirus, replicates via reverse transcription of the RNA genome to form a DNA intermediate.
Time
Pla
que
form
ing
units
Eclipse phase
Mean burst size
Latent period
- DNA integrates into host DNA (provirus), may remain dormant- Expressed by host RNA pol II, to make HIV mRNAs, regulated by splicing- Virus particles bud from cell surface- Transmission: sexual, intravenous drug use, vertical transmission, contaminated blood products- Entry: virus binds cells expressing CD4 and a co-receptor CCR5 (macrophage tropic strains) or CXCR4 (T-cell tropic
strains)- Outcome of infection: short acute illness, then patient may remain largely asymptomatic for 2-10 years, finally CD4 cells
decline and resulting immunodeficiency enables infection by opportunistic pathogens Herpes simplex virus
- Genome: linear ds DNA 152 kb, 80 genes- Replication: in nucleus, may replicate via lytic cycle (cascade of gene expression) or become latent - HSV-1, cold sores; HSV-2, genital herpes- Infection: via skin cuts and abrasions, HSV-2 is a STD- Local replication: entry of neurones, retrograde axonal transport to local ganglion- Latent infection: genome becomes circular, remains in nucleus, not integrated into host DNA- Only one area of the genome transcribed: latency associated transcript (LAT), no protein expression- Virus remains dormant for decades, then may reactivate, enter lytic cycle and pass down same nerve axon to cause
recurrent infection at original site Varicella-zoster virus
- An alpha herpes virus closely related to HSV- Primary infection causes chicken pox- Immune system clears systemic infection but the virus becomes latent in nerve cells, as for HSV- On reactivation, the disease is different: shingles, very painful!- Both HSV and VZV are present in the majority of the population, successful parasites!
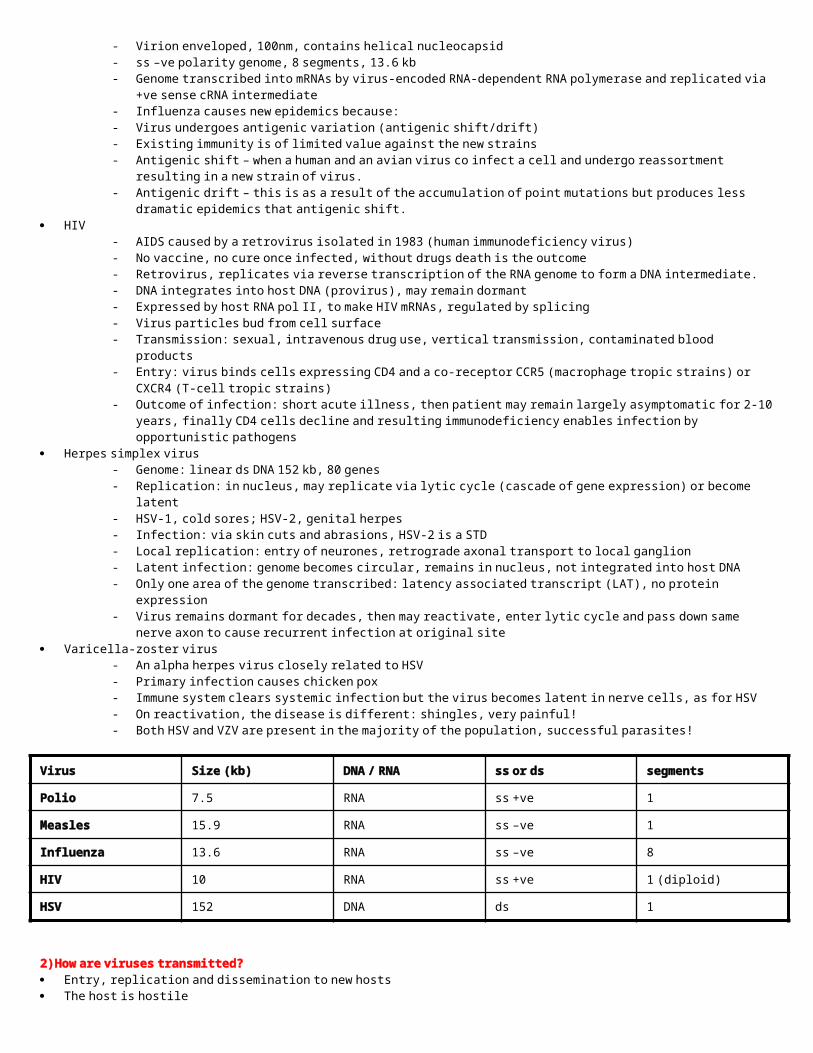
Virus Size (kb) DNA / RNA ss or ds segments
Polio 7.5 RNA ss +ve 1
Measles 15.9 RNA ss –ve 1
Influenza 13.6 RNA ss –ve 8
HIV 10 RNA ss +ve 1 (diploid)
HSV 152 DNA ds 1
2) How are viruses transmitted? Entry, replication and dissemination to new hosts The host is hostile
o Non-specific defenses skin, mucous membranes, acid pH, proteases
o Innate immunity Complement, NK cells, phagocytes, interferons, fever, inflammation
o Specific immune response Antibody, cytotoxic T cells
Factors affecting transmission Particle stability (enveloped less stable) Duration of virus shedding Virus concentration Availability of new hosts (population size, animal reservoirs)
There are many different entry routes associated with viral disease, these include:o Respiratory tract - Influenza, mumps, measles, variola, varicella-zoster virus (VZV), rhinoviruso Skin cuts and abrasions - Papilloma viruses (HPV), HSV-1 & 2, rabies (bites), yellow fever virus (mosquito)o Blood products - HIV, hepatitis B virus (HBV), hepatitis C virus (HCV)o Genital tract - HIV, HSV-2, HPV 16 & 18o Alimentary canal - Polio virus, hepatitis A virus, rotavirus
3) Outcome of the infection The outcome of the infection is influenced by several factors:
- Viral dose- Route of entry- Age and physiological state of host e.g. HBV – neonate, male > female
Consequences of infection may lead to cell death, persistant/latent infection or even cell transformation and cancer (HBV, Human Papilloma Viruses, Epstein-Barr Virus)
With local infections, replication occurs locally, there is also a shorter incubation period before symptoms With systemic infections, there are multiple phases of replication as virus spreads through body, therefore there are longer incubation
times. The infection may spread through blood stream or nerves. Systemic infection normally causes more severe infection and clearance of it depends more on cellular immunity.
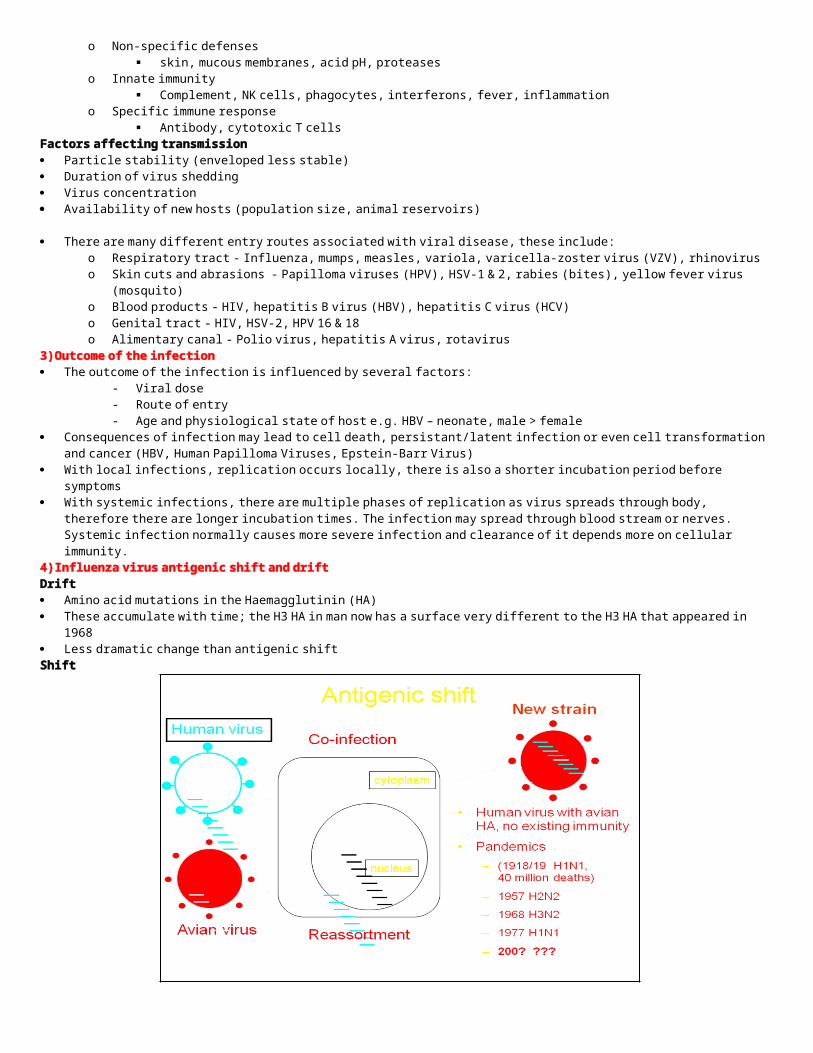
4) Influenza virus antigenic shift and driftDrift Amino acid mutations in the Haemagglutinin (HA) These accumulate with time; the H3 HA in man now has a surface very different to the H3 HA that appeared in 1968 Less dramatic change than antigenic shiftShift
5) HIV Life cycle and epidemic Transmission: sexual, intravenous drug abuse, mother to baby, contaminated blood products Entry: virus binds cells expressing CD4 and a co-receptor CCR5 (macrophage tropic strains) or CXCR4 (T-cell tropic strains) Mutant allele of CCR-5 with 32 nucleotide deletion. Causes termination of protein after transmembrane domain 4. Mutant protein does
not function as HIV-1 co-receptor – homozygous (1%) resistant to infection – Heterozygote’s (16%) but only 10% HIV pop. Acute: 2 months, active virus replication, viraemia, temp loss of CD4+ PBL Asymptomatic: up to 15 years, active virus replication in lymph nodes, not in PBL, continuous virus variation, controlled by CTL AIDS: CD4 counts drop to low levels, unrestricted virus replication, opportunistic infections, death Different outcomes of infection: Slow progressors, Long term non-progressors, Rapid progressors
Lecture 3: Antiviral drug strategies1) Explain why it is difficult to develop drugs which selectively act against viral infections. Viruses are intracellular, obligate parasites which use host cell metabolism and processes. Difficult to target virus, without also
damaging host.2) Give examples of classes of drugs which have been used successfully in antiviral therapy. Stages of the viral replication cycle amenable to drug therapy:
Attachment No drugs yetPenetration/Uncoating Amantadine/Rimantadine Influenza AGenome replication Nucleoside analogues
Non-nucleoside inhibitorsRibavirin
Herpes viruses, HIVHIVRNA viruses
Genome expression Ribavirin RNA/DNA virusesAssembly/Maturation Protease inhibitors HIVRelease Relenza/Tamiflu Influenza A and B
3) Describe the strategies underlying the search for novel antiviral agents. Unlike antibiotics, there are few (if any) naturally occurring antivirals. Viral chemotherapy strategies:
- Identify viral enzymes and other proteins (e.g. receptors) which are essential for replication.- Screen for inhibitors of these viral proteins.- Knowledge of the viral protein function and structure aids in designing specific antivirals.- Ensure that the chemotherapeutic index (dose of the drug which inhibits virus replication/dose which is toxic for the host)
is acceptably small.4) Describe the roles of innate and adaptive immune responses in defence against viral infections Innate: this response is not a specific one and uses complement, NK cells, phagocytes, interferons and fever and inflammation Adaptive: This is a memory response and uses antibodies and cytotoxic T cells to mount a more specific and rapid response.5) Explain how some viruses evade natural immune responses Viruses will evade the natural defenses like skin, mucosa, membranes, acid and proteases by entering through cuts or adapting so
that these factors have no effect on them. Once in the body it will aim to replicate as efficiently as possible.
They may also secrete inhibitors to the immune response or be protected from them by a protein coat.6) Give examples of viral infections for which vaccination is a successful strategy. smallpox, diphtheria, tetanus, yellow fever, pertussis, measles, mumps, rubella and poliomyelitis are all diseases for which vaccination
is a successful stratergy.
Lecture 4: Parasite Infections
1) Define the relationships – parasitic, symbiotic, commensal. Parasite - organism living in or on the host and dependent on it for nutrition- causing damage (many infections – not just protozoa and
helminths) Symbiotic - mutual benefit Commensal - neutral2) Describe the major differences between protozoa (single cell organisms) and metazoa (helminths).Protozoa single celled organisms Eukaryote (genome within a nucleus, complex organelles in cytoplasm) Pathogenesis (mechanism of disease) varied Some have insect vectors (eg malaria) No eosinophilia Metazoa Multicellular organisms (Helminths/worms) Free living, intermediate hosts and vectors Some just inhabit gut - others invade Eosinophilia – if invade blood3) Describe how, as eukaryotes, protozoa (amoeba, coccida, flagellates, ciliates) differ from prokaryotes. Have a cell membrane rather than cell wall DNA material linear (chromosomes) plus circular elements, bounded by a membrane Cytoplasmic inclusions such as mitochondria, golgi apparatus etc Cell division generally slow Amoeba - Amoebiasis – dysentery (bloody diarrhoea), liver abscess Coccida –
o Plasmodium species Malariao Toxoplasma Toxoplasmosiso Cryptosporidium Diarrhoea
Flagellates –o Giardiasis – diarrhoea, lethargy o Leishmaniasis (from sand fly) – visceral and cutaneous
Ciliates – Balantidiasis (pigs and cattle) – diarrhoea 4) Malaria – an example of a protozoal disease. Give a brief life cycle relevant to clinical disease.
Fever, shivering, vomiting, severe anaemia, convulsions
Brian damage, encephalopathy, unrousable coma Hepatomegaly, splenomegaly, hypoglycaemia 5) Metazoa – roundworms, flatworms, flukes cause much morbidity rather than mortality. Explain using an example.

Complex muticellular parasites Cycles may involve insect vectors and intermediate hosts For most, humans are the definitive host - few are zoonoses (acquired from animals) Adult worms cannot multiply in man - number of adults related to infection Lay eggs, microfilaria, larvae True parasites for the most part (morbidity > mortality). Tapeworm: Any of a group of worms that have a long thin ribbon-like body and live as parasites in the intestines. Body consists of a
head (scolex), a short neck, and a strobila made up of a chain of separate segments (proglottides). Cause infection in the gut e.g. Ascaris and also in the tissues e.g. Trichinella infection typically associated with the ingestion of undercooked pork.
Fluke: Often have suckers for attachment to their host, occurring in the liver, lungs, gut, and blood vessels. Usually have a snail intermediate host; sometimes also a second host such as a fish or crab; distribution reflects the snail “availability” e.g. Shistosomiasis – the most important fluke infection affecting millions worldwide.; live in pelvic or mesenteric veins; causes calcification in bladder, inflammatory changes in the liver etc.
Roundworm: Unsegmented cylindrical body, tapering at both ends. Tapeworm infection is acquired by ingestion of meat containing the encysted larval forms; develop and attach to wall of small intestine; adult can be 10m long; segments detach and pass out in faeces; more animals get infected. Difficult to treat.
Lecture 5: Bacterial Properties1) Define the terms commensal and pathogen used in association with bacteria. Commensal bacteria – normally present bacteria (e.g. the gut) that are beneficial to the host. If the body’s resistance is impaired,
these commensal bacteria can enter the tissue, causing disease. Pathogen – environmental cause of disease, though this term is used commonly only when referring to bacteria. Pathogenicity refers
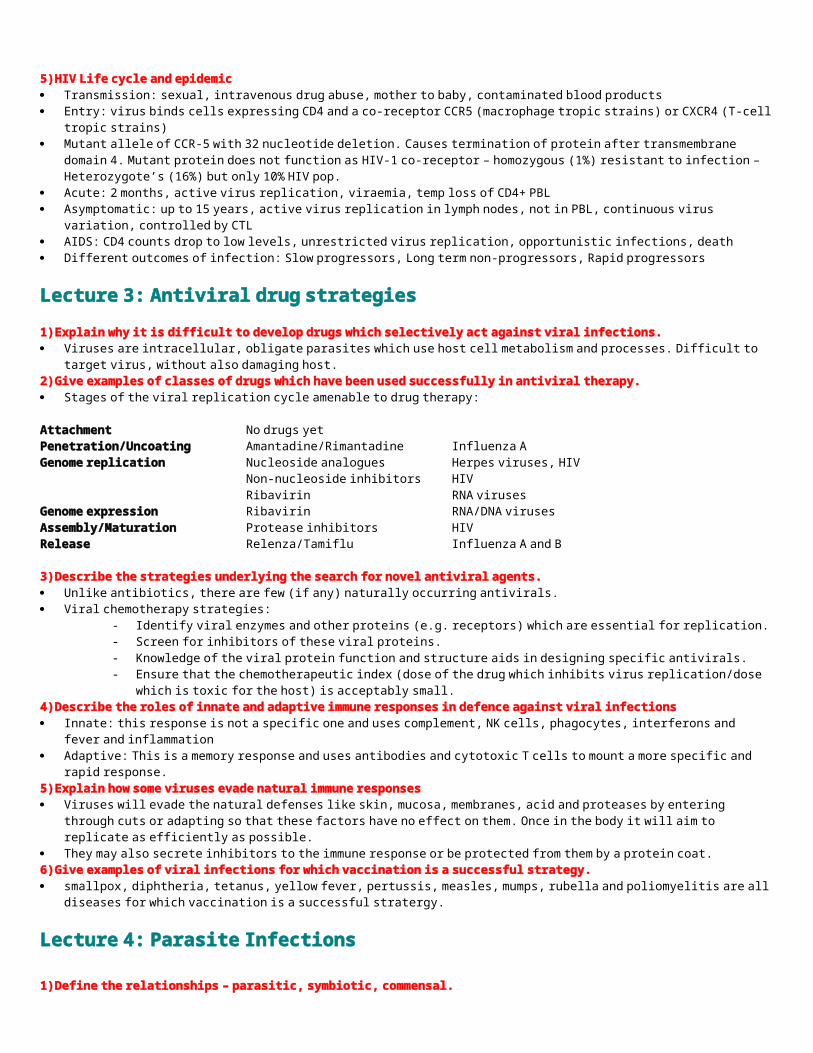
to the capacity of an infectious agent to cause disease.2) Describe the structure and means of replication of bacteria Bacteria – prokaryotic. Contain a chromosome of DNA but no nucleus. Divide by binary fission. They also do not have any membrane
bound organelle, no complex internal membrane (e.g. Golgi), and it has a single circular chromosome The components of the bacterial structure include: capsule/glycocalyx, pili/fimbrae and flagellum The capsule /glycocalyx is usually made of polysaccharide, and is antiphagocytic. It is used I attachment and colonisation to form
plaques. Pili/fimbrae are attached to the surface and are used in genetic exchange (conjugation) Flagellum is used for motility The bacteria also contains a cell wall to maintain shape Other structures not mentioned include:
3) Explain the meaning of the following terms used when describing bacteria: coccus, bacillus, rod; Gram-negative, Gram-positive, acid-fast; aerobic, anaerobic, in terms of bacterial structure and function. The major classification of bacteria is according to shape: coccus is a spherical bacteria, bacillus is a rod shaped bacteria.
Another classification is staining characteristics; Gram-positive bacteria, when stained with crystal/iodine complex, the complex penetrates the thicker exposed cell wall and thus is not easily washed away so the stain remains purple. In Gram-negative bacteria the outer membrane protects the cell wall so the stain is easily washed away. (gram positive cell walls are thick, whereas the gram negative cell walls are thin. The are between the thin cell wall and the outer membrane of the gram negative bacteria is called the periplasm
Acid-fast bacteria have fatty cell walls which prevent the cells from being decolourised by acid solutions after staining during diagnostic tests.
Cultural characteristics such as aerobic (able to survive only in oxygen-rich conditions) and anaerobic (able to survive in oxygen-deprived conditions) can also be used to classify bacteria.
4) Outline the three main ways bacteria use to exchange genetic material. Conjugation: Movement of DNA requiring cell-to-cell contact and pili. A copy of the genetic material is transferred from donor cell to
recipient cell. Transduction: Movement of DNA by bacteriophage and does not require cell-to-cell contact.
cytoplasm
plasma membranechromoso
meplasmid
Transformation: Transfer of naked DNA between bacteria. Does not require cell-to-cell contact. Some bacterial species are naturally competent for transformation.
Lecture 6: Bacterial Diseases1) List the potential sources and possible routes of infection by bacteria. Sources of infection
- other human beings with active disease, subclinical infection of who are carriers- animals or their products (zoonotic infection)- food- water- soil, dust, air
Routes of infection- inhalation (risk activity – breathing)- ingestion (risk activity – eating or drinking)- contact ( risk activity – sport, touch-feely activities, cuddling babies…)- sexual transmission (risk activity – sex)- through wounds (risk factors – natural wounds, bites, surgery…)- vector borne (risk activity – exposure, lack of cleanliness)- mother to foetus – vertical transmission
2) Explain the concepts of infectivity and virulence and define the term infective dose. Infectivity – the ability to colonise and invade. Virulence – used to denote variations in the degree of pathogenicity/damage caused within the host. Virulence is based on:
- Tropism: host and tissue specificity (adherence via pili and host cell surface receptors)- Multiplication: evasion, nutrient acquisition- Cytotoxicity: damage to host tissues (toxins)
Infective dose = the amount of microorganism required to cause disease3) Give examples of bacterial pathogens transmitted by different routes and outline the ways in which they cause disease. Cholera is a local infection at the epithelium. The bacteria are usually present in the water supply and colonise the gut epithelium.
They replicate and further transmission is faecal. The cholera toxin causes fluid imbalance which leads to diarrhoea. The disease is mediated by the release of a soluble toxin composed of A and B subunits. The A subunit enters the host cell via a ganglioside and causes ADP ribosylation of adenylate cyclase producing more cAMP which causes diarrhoea.
Meningitis is commonly caused by the spread of the microorganism (commonly Neisseria meningitidis from a carrier to a non-carrier. In the carrier state there is colonisation of the nasopharyngeal epithelium but it can spread into the bloodstream causing septicaemia and meningitis. The bacterial lipopolysaccharide causes the release of host cell cytokines which can cause septic shock.
Tuberculosis is a bacterial infection (Mycobacterium tuberculosis) of a respiratory nature. In primary TB, there can be granuloma formation in which tissue destruction results in caseous necrosis where the centre of the granuloma appears dry and ‘cheese-like’. Secondary TB is usually due to reactivation of latent mycobacteria when the immune system is suppressed.
Lecture 7: Defence and vaccination against bacteria1) Explain the following non-immune mechanisms of host defence against infection: natural barriers, secretions, commensal organisms. Skin is a natural barrier to microorganisms Respiratory tract
o hairs in the nostrils filter large particleso ciliated and mucus-secreting cells (mucociliary clearance)o alveoli lined with macrophages
Digestive tracto mouth is bathed in saliva (lysozyme)o microorganisms have to resist acid, proteolytic enzymes and bile
Urinogenital tracto flushing action of urineo lactobacilli in the vagina inhibits the growth of most other microbes
Conjunctivao tears (lysozyme) and blinking
2) List the major components of the innate immune response and the major antimicrobial mechanisms Recruiting immune cells to sites of infection and inflammation, through the production of chemical factors, including specialized
chemical mediators, called cytokines. Activation of the complement cascade to identify bacteria, activate cells and to promote clearance of dead cells or antibody complexes
(opsonisation) The identification and removal of foreign substances present in organs, tissues, the blood and lymph, by specialized white blood cells
(phagocytic cells) Activation of the adaptive immune system through a process known as antigen presentation.3) Explain how an adaptive immune response is involved in defence mechanisms operative against major bacterial pathogens.Humoral Immunity directly mediated by antibodies antibodies are produced by B lymphocytes Plasma cells (terminally differentiated B lymphocytes) are the primary source of secreted immunoglobulins
Cell Mediate Immunity not primarily mediated by antibody mediated by T lymphocytes and NK cells indirectly other cell types may play a role e.g. macrophages
Antibodies:- neutralise bacterial toxins- prevent bacterial adhesion (e.g. IgA at mucosal surfaces)- promote phagocytosis (opsonisation) - promote complement fixation and activation ‘classical pathway
T cells: T cells play a pivotal role in determining the outcome of the immune response Cytokines
- soluble mediators produced by a wide variety of cells- modulate and focus cellular immune response- potentiate humoral immune response- aid in cell mediated response (macrophage activation, TC cell)
CD4 positive -T helper cells CD8 positive -cytotoxic T cellsAntigen
Antigen Presentation Antigens are presented to lymphocytes by antigen presenting cells
- macrophages, B cells, dendritic cells- involves MHC class I or II molecules
Antigen presenting cells process protein antigens (proteolytic cleavage) to produce peptides Peptides presented to:
- TH cells in conjunction with MHC class II- TC cells in conjunction with MHC class I
4) Describe how infectious agents avoid host defences. Resist phagocytosis: polysaccharide capsule; actively inhibit phagocytosis, hide inside other cells Inhibit intracellular killing: escape from phagosome; inhibit phagosome maturation Resist complement: thick cell wall; polysaccharide capsule Resist antibodies: IgA protease; antigenic variation5) Explain the difference between active and passive immunization. Passive immunization – neutralisation of the toxin by preformed antibodies being injected into the patient or across the placenta to a
developing foetus. Active immunization - raise antibodies by injecting toxin preparation to elicit protective immunity and immunological memory.6) Give examples of the different types of vaccine presently available and how they are used. Live vaccines (where virulence has diminished)
- polio, MMR, BCG Subunit vaccines (parts of the original microbe used, containing the antigen)
- toxin: tetanus, diphtheria- capsule: Hib, MenC
K illed (intact organism containing antigen)- polio
Toxoids (bacterial toxin(inactivated))- DT
Conjugates (polysaccharide antigen attached to protein carrier)- neisseria meningitis
Limitations: - costs of vaccines and delivery systems- safety concerns and vaccine scares- some vaccines are less effective than others- some pathogens change their surface structures- surviving initial infection doesn’t always guarantee resistance
Novel approaches: - recombinant vaccinia virus- DNA vaccination- live attenuated enteric pathogens (oral delivery)
Lecture 8: Fungal Infections1) Outline the main differences between fungi (eukaryotes) and bacteria (prokaryotes) Eukaryotic organisms have complex cells Genetic material is organised into a membrane-bound nucleus2) Summarise briefly the ecology and epidemiology of infectious fungiTypes of fungal infection: Allergy – airborne spores – asthma, rhinitis, dermatitis Mycotoxicosis – toxic reaction caused by ingestion or inhalation of a mycotoxin Mycoses - infection3) List the major groups of disease causing fungi and specify their growth forms. Mycelial fungi have a filamentous structure and reproduce by means of spores.
Yeasts are typically unicellular, round or oval in shape. Dimorphic fungi may be either mycelial or yeast form depending on growth conditions. Most disease causing species are moulds but there are also some yeasts and dimorphics. Dimorphic fungi are often mould-like in
nature but yeast-like when causing an infection.4) Define the terms superficial mycoses and deep mycoses, giving appropriate examples of each type of infection. Mycoses are the diseases caused by yeasts and fungi of which there are two types: superficial and systemic (deep) mycoses. Superficial infections of the skin, hair, nails and mucous membranes are the most common e.g. ringworm caused by moulds and
yeast infections caused by Candida. No living tissue is infected so no cellular response from the host. Black Piedra Cutaneous - Dermatophytes, or keratinophilic fungi. Produce extracellular enzymes (keratinases) which are capable of hydrolyzing
keratin. Inflammation is caused by host response to metabolic by-products. Tinea (latin: worm) pedis (atheletes foot) Subcutaneous – rare. Chronic, localized infections of the skin and subcutaneous tissue following traumatic implantation of the
aetilogic agent. Sporotrichosis. Systemic mycoses are unusual, but opportunistic mycoses can cause disease in immunocompromised patients e.g. those caused by
Aspergillus and Cryptococcus.5) Describe briefly the main classes of antifungal agents
Lecture 9 – Hospital acquired infection and antibiotic resistance 1) The important bacterial pathogens that are multi-drug resistant Gram negatives Pseudomonas aeruginosa – hospital acquired pneumonia, UTI. Immunocompromised hosts especially. Survices on abiotic surfaces. Acinetobacter baumanii - ITU infection ESBL Enterobactaeciae Gram positives Enterococcus faecium – Line and UTI MRSA – colonises skin and nasopharynx . Line associated sepsis, UTI, bloodstream infections, disseminated spread
2) Reasons for the high rate of hospital acquired infectionsIntervention Lines Intravenous Central Arterial CVP/Pulmonary artery Chemotherapy Catheterisation Prophylactic antibiotics Inappropriate prescribing Intubation Prosthetic materialDissemination Health care professionals, visitors, clothing worn Concentration 3) Describe the mode of action of the major groups of antibiotics and list the mechanisms of resistance to them. Selective toxicity can be achieved relatively easily because bacterial structure is distinct from mammalian cells, which are eukaryotic.
Bacteria lack intracellular membrane-bound organelles such as a nucleus and mitochondria, have a complex cell wall containing protein, lipids and peptidoglycan, use a smaller 70S ribosome and have unique metabolic pathways.
Basteriostatic activity = level of antibiotic needed to inhibit growth Bacterioidal activity = level of antibiotic needed to cause death Bacterial target sites
- Cell envelope synthesis: beta-lactams (penicillin, cephalosporins), vancomycin, isoniazid, ethambutol, cycloserine, ethonamide
- Protein synthesis: aminoglycosides, tetracycline, macrolides and clinamycin- Nucleic acid synthesis: quinolones, rifampicin and metronidazole- Antimetabolites: sulphonamides, dapsone, and trimethoprim
Resistance to antibacterial agents- Produce enzymes that inactive the antibiotic by attaching or cleaving a key bond,- change their permeability to the antibiotic either by alterations in the cell wall or by pumping the antibiotic out of the cell
and hence decreasing the amount of antibiotic that reaches the target- develop an altered structural target such that the target has a lowered affinity for the antibiotic but can still function- develop an altered metabolic pathway that bypasses the reaction inhibited by the antibiotic
4) Some of the approaches to prevent the emergence of drug resistant bacteria and nosocomial infections Hygiene Single rooms Change lines/monitor regularly Screen those at high risk Discharge patients Avoid unnecessary antibiotics Drug combination Narrow vs. Broad spectrum Develop new drugs Examples of antibiotic resistance. Resistance to penicillin: Penicillin discovered in 1928.
- First bacterium to become resistance was Staphylococcus aureus, often harmless but can cause pneumonia or toxic shock syndrome.
- Streptococcus pneumoniae, another cause of pneumonia, began to demonstrate resistance in 1967.- 1976, penicillin resistant gonorrhoea- 1983, resistant strains of Enterococcus faecium causing intestinal infection
Tuberculosis: Leading cause of death among infectious diseases. Mycobacterium tuberculosis is usually treated by a combination of antibiotics. However, organisms which are resistant to several antibiotics have arisen, probably because of non-compliance of the long treatment regimen, and so it is no longer possible to guarantee a cure by antibiotic treatment.