수유 중 약물 복용의 상담 원칙 2016
TRANSCRIPT

단국대학교 의과대학 제일병원 한국마더세이프안현경
수유 중 약물 복용의 상담 원칙

젖의 장점

Mother
Reduced risk of fracture/
osteoporosis
Reduced risk of cancer
Emotional
Convenience
Cost
Baby
Reduced risk of infection
Reduced risk of SIDS
Reduced risk of many im-
mune mediated diseases
Emotional/Bonding
모유수유의 장점

수유아

1970 1982 1985 1988 1997 2000 2002 2005 2007 20090.0
20.0
40.0
60.0
80.0
100.0 99.7
68.9 59.0
36.4
14.1 10.2 6.5 12.7
37.4 46.0
모유수유율

90%
10%
모유수유계획분유수유계획
임신 중 모유수유 계획 율- 제일병원

• 의료인의 권유
• 젖이 모자라서
• 함몰 유두• 젖을 못 빨아서• 물 젖이어서• 유두가 아파서• 기타
37.1%18.8%
12.1%10.5%
7.0%6.1%8.4% 이승주 등 . 소아과 40: 1336
모유수유 중단요인
90% of women: medication in first week postpartum
Mothers worry about effect of medication on nursing infant Non compliance
Weaning
Aavoidance of breastfeeding
50% of mothers more reluctant to take a medication while
nursing than during pregnancy
수유 중 약물복용

Nearly all drugs pass into human milk
Almost all medication appears in small amounts, usu-
ally less than 1% of the maternal dose
Very few drugs are contraindicated for nursing moth-
ers
수유 중 약물복용

Mother HIV + (in USA)
Use of illegal drugs by mother
Certain medications
Active, untreated TB in mother
Galactosemia in baby
Mother HTLV +
Herpes on breast
모유수유금기 (AAP 2005)

Pharmacokinetic factors
Factors which govern drug transfer across membranes
into breast milk as well as the metabolism of the drug
in mother and infant
약물 선택시 고려사항

Passive diffusion
Molecular weight
Protein binding
Lipid solubility
Half life
Oral bioavailability
PHARMACOKINETIC FACTORS

PASSIVE DIFFUSION
Drugs move in and out of breast milk
High to low
With time direction may shift
Example: alcohol

High molecular weight limits movement into breast
milk
MW >500 daltons does not enter breast milk
MOLECULAR WEIGHT

Insulin: MW > 6,000 daltons
Heparin: MW 40,000 daltons
Ethanol: MW 200
MOLECULAR WEIGHT: EXAMPLES

Medications circulate in maternal circulation bound or
unbound to albumin
Only unbound drug gets into maternal milk
Definition of good protein binding > 90%
PROTEIN BINDING

High protein binding
Propranolol 90%
L2
Diazepam 99% L3
Low protein binding
Lithium 0% L3
PROTEIN BINDING

Drugs that are very lipid soluble penetrate into breast
milk in higher concentration
Drugs that are active in the CNS are drugs with high
lipid solubility
LIPID SOLUBILITY

Short half life drugs
Alcohol 24 min
Keflex 50 min
Ibuprofen 120 min
General anesthesia
Long half life drugsProzac 216 hours
HALF LIFE

Amount of drug that is absorbed from the gut into the blood stream
ORAL BIOAVAILABILITY

Drug
Maternal gut and liver
Maternal plasma
Infant gut
Infant plasma
Oral bioavailability variesHigh (>90%) Low (<50%)Acetaminopen Acyclovir Lo-razepam AzithromycinMetronidazole BudesonideMinoxidil Sulfasalazine
Dilution of all drugs leads to low concentrations in mother’s plasma
Only drugs are not protein-bound can pass into milkDrug protein bindingHigh LowBepridil >99% Bisoprolol 30%Diazepam 99% Cyclophosphamide 13%Diclofenac >99% Ranitidine 15%Propranolol 90% Primidone <20%Oral bioavailiability varies
Usually very low levels (often undetectable)
ROUTE OF DRUGS FROM MOTHER TO BABY VIA BREASTMILK

Low bioavailability may be due to
Reduced absorption in GI tract
Poor GI stability due to acidity
High first-pass uptake by liver
ORAL BIOAVAILABILITY

Gentamycin
<1% oral bioavailability
Insulin (destroyed in gut)
0% oral bioavailability
Heparin (destroyed in gut)
POOR ORAL BIOAVAILABILITY

Drugs transfer into human milk if they:
Attain high conc. in maternal plasma
Are small enough
Are non-protein bound
Are highly lipid soluble
Then once in breast milk:
Are affected by oral bioavailability in baby’s gut
SUMMARY
IN GENERAL, BABY GETS <1% OF MATERNAL DOSE OF DRUG

유아 고려사항
AgeBody weightHealth status
모성 고려사항
DoseRoute of administra-
tionHealth status
약물 선택 시 고려사항

Avoid unnecessary drug use and l imit use of OTC products Assess the benefit/risk ratio for both mother and infant Avoid use of drugs known to cause serious toxicity in adults or
children Choose drugs for the mother that have known and established in-
formation about their pharmacokinetics and toxicity and have low concentrations in breast milk and low relative infant dose
Avoid new drugs if possible Drugs licensed for use in infants do not generally pose a hazard Neonates (esp. premature infants) are at greater risk from expos -
ure to drugs via breast milk
약물 선택 시 일반적인 고려사항

Route of administration (minimum amount of drug to the infant)
Choose medications : shortest T 1/2 , highest protein binding ability, poorest oral absorption, lowest lipid solubility, well-studied in infants.
Avoid feeding the infant at the time of peak concentration of the drug in milk.
To minimize drug level in the milk administer the drug at / immediately after the infant feeds.
Avoid long-acting drug In case of no available alternative, medication is best
taken just prior to the longest sleep of the infant.
약물 선택 시 일반적인 고려사항

Monitor Infants exposed to drugs via breast milk for un-usual signs/symptomsfeeding, sedation, irritability, rash, etc
For some medications with potential harm, temporary suspension of breastfeeding may be necessary. Withhold breastfeeding temporarily if the drug is only
used for a short durationAdvice the mother about milk expression & cup feeding
instead of bottle feeding to avoid nipple confusion
약물 선택 시 일반적인 고려사항

L1 safest
L2 safer
L3 moderately safe
L4 possibly hazardous
L5 contraindicated
LACTATION RISK CATEGORY BY THOMAS W HALE

모유수유 중 약물 상담

( 서울 콜센터 2014. 12)
상담종류별 상담건수 분포

모유수유 상담 비율
모유수유 중 질병으로 인한 약물상담
89%
모유수유방법 관련상담11%
모유수유 상담 : 1,190 건
생식발생독성정보활용화 연구 식약처 2008

상담수유부의 질병 분류
생식발생독성정보활용화 연구 식약처 2008

모유수유지속81%
수유중단10%
중단후 재수유9%
약물 복용 후 모유수유 여부
생식발생독성정보활용화 연구 식약처 2008

한국마더세이프전문상담센터
모유 수유중 다빈도 질문

SUMMARY
CompatibleDrug?
Is a compatible Drug available?
D/C drug &breastfeed
Is therapyNecessary?
Monitor nursling
Monitor nursling
Is there a non-drug Alternative
That is compatible?
Can therapy bePostponed?
If acceptable pursue It & breast-
feed
Yes
YesYes
Yes
No
No
No
No

감사합니다 .


Reasons for using the telephone line in breastfeeding women
HemorrhoidCV diseaseGI diseaseContraceptionHepatitis BRespiratory disease
OthersPsychotic diseaseNutritionBreast problem
Dental diseasePain
Inflamation
Dermatologic diseaseThyroid disease
12.5%11%
9.6%
7.4%

AntihistamineRegional agents
Miscellaneous
CV agentsNutritional agentsNatural & Herbal proEndocrine agentsRespiratory agents Systemic antibiotics
CNS agents & Analges
GI drugs
Drugs prescribed for breastfeeding women

SUMMARY
Drugs transfer into human milk if they:Attain high conc in maternal plasmaAre small enoughAre non-protein boundAre highly lipid solubleThen once in breast milk:Are affected by oral bioavailability in baby’s gut

SUMMARY

DRUG CLASSIFICATION BY AAPCytotoxic drugs Drugs of abuse for which adverse effects on
the infantRadioactive compounds that require temporary
cessation of breastfeedingDrugs for which the effect on nursing infants in
unknown but may be concernDrugs that have been associated with signifi-
cant effects on some nursing infants and should be given to nursing mothers with cau-tion
Maternal medication usually compatible with breastfeeding

Maternal factor Dose and duration of therapy Route of administration Drug pharmacokinetics
Infant factor Infant’s ability to absorb, metabolize, and excrete the
drug Gestational age of infant and its postnatal age
DRUG TRANSFER INTO THE BREAST MILK

Infant age Premature and newborn infants are at somewhat
greater risk Infant stability
Unstable infants with poor GI stability may increase the risk of using medications
Pediatric approved drugs Generally are less hazardous if long-term history of
safety is recognizedDose
In a premature infant various doses may be more risky than in a 1 year old healthy infant
Drugs that alter milk production May be much more risky during neonatal period than
much later
EVALUATION OF THE INFANT

상담 시 주지 사항 및 상담내용약을 꼭 복용해야 하는지 평가한다 .젖을 빨리고 난 다음 약을 복용한다 .약물을 단기간 사용 할 경우에는 수유를 잠시 멈춘다 .정확한 정보가 있는 약으로 아이에게 영향이 적은 약을 선택하게 한다 .전신적으로 작용하는 약보다는 국소적으로 작용하는 약을 선택하게 한다 .


Beta-blocking agents Acebutolol Atenolol Labetalol Propranolol Sotalol
SalicylatesLithiumAntineoplastic agentsDrugs of abuse
DRUGS TO AVOID IN THE NEWBORN AND IN INFANTS < 6MONTHS OF AGE
CYTOTOXIC DRUGS THAT MAY IN-TERFERE
WITH CELLULAR METABOLISM OF THE NURSING INFANT
Cyclophosphamide Cycloserine Doxorubicin Methotrexate

DRUGS OF ABUSE FOR WHICH ADVERSE EFFECTS ON THE INFANT
DURING BREASTFEEDING HAVE BEEN REPORTED
Drug Reported effect or reasons for concernAmphetamine Irritability, poor sleeping patternCocain Cocaine intoxication: irritability, vomiting, di-
arrhea, tremulousness. seizureHeroin Tremous, restlessness, vomiting, poor feedingMarijuana Only 1 report in literature; no effect men-
tioned; very long half-life for some compo-nents
Phencyclidine Potent hallucinogen

AAP Clssification
RADIOACTIVE COMPOUNDS THAT REQUIRE TEMPORARY CESSATION
OF BREASTFEEDING
Copper 64 Gallium 67 Indium 111 Iodine 123 Iodine 125 Iodine 131 Technetium 99 Radioactive sodium

Anti-anxiety antidepressants antipsychotic Others
AlprazolamDiazepamLorazepamMidazolamPerphenazinePrazepamQuazepamTemazepam
AmitryptilineAmoxapineBupropionClomipramineDesipramineDothepineDoxepineFluoxetineFluvoxamineImipramineNortriptylineParoxetineSertralineTrazodone
ChloropromazineChlorprothixeneClozapineHaloperidolMesoridazineTrifluoperazine
AmiodaroneChloramphenicol ClofazimineLamotriginemetronidazoleMetoclopramideTinidazole
Drugs for which the effect on nursing infants is un-known but may be of concern
AAP Clssification

AAP Clssification
Drug Reported effectAcebutolol Hypotension; bradycardia; tachycardia5-aminosalicylic acid DiarrheaAtenolol Cyanosis; bradycardiaBromocriptin Suppresses lactation; may be hazardous to the motherAspirin Metabolic acidosisClemastine Drowsiness irritability, refusal to feed, high-pitched cry, neck stiffnessErgotamine Vomiting, diarrhea, convulsionsLithium One-third to one-half therapeutic blood concentration in infantsPhenindione Anticoagulant; increased prothrombin and partial thromboplastin time
in 1 infant; not used in united statesPhenobarbital Sedation; infantile spasm after weaning from milk containing pheno-
barbitalPrimidone Sedation feeding problemsSlfasalazine Bloody diarrhea
Drugs that have been association with significant ef -fects on some nursing infants and should be given to nursing mothers with caution

AcetaminophenAcetazolamideAcitretinAcyclovirAlcohol (Ethanol)AllopurinolAmoxicillineAntimonyAtropineAzapropazoneAztreonam
B1(Thiamin)B6(Pyridoxine)B12BaclofenBarbiturateBendroflumethiazideDicumarolBromideButorphanol
CaffeineCaptoprilCarbamazepineCarbetocinCarbimazoleCascaraCefadrxilCefazolinCefotaxime
AAP Clssification
Maternal medication usually compatible with breast-feeding

CefoxetineCefprozilCeftazidimeCeftriaxoneChloral hydrateChloroformChloroquineChlorothiazideChlorothalidoneCimetidineCiprofloxacinCisapride
CisplatinClindamycinClogestoneCodeineColchicineOral contraceptive pill with estr/progesCycloserineD (vitamin)DanthronDapsonDexbrompheniramine
DiatrizoateDigoxinDiltiazemDipyroneDisopyramideDomperidoneDyphyllineEnalprilErythromycinEstradiolEthambutolEthosuximide
AAP Clssification
Maternal medication usually compatible with breast-feeding

FentanylFexofenadineFlecainideFleroxacinFluconazoleFlufenamic acidFluoresceinFolic acidGadopentaticGentamicinGold saltsHalothane
HydralazineHydrochlorothiazideHydroxychloroquineIbuprofenIndomethacinIodidesIodineIodine(Povidone-iodine)IohexolIopanoic acidIsoniazid
InterferonIvermectineK1(vitamin)KanamycinKetoconazoleLabetalolLevonorgesterolLidocaineLoperamideLoratadine Magnesium- sulfate
AAP Clssification
Maternal medication usually compatible with reastfeed-ing

Medroxypro- gesteroneMefenamic acidMeperidineMethadoneMethimazoleMethohexitalMethyldopaMethyprylonMetoprololMetrizamideMetrizoate
MexiletineMinoxidilMorphineMoxalactamNadololNalidixic acidNaproxenNefopamNifedipineNitrofurantoinNorethynodrelNorsteroids
NoscapineOfloxacinOxprenololPhenylbutazonePhenytoinPiroxicamPrednisolonePrednisoneProcainamideProgesteronePropoxyphenePropranolol
AAP Clssification
Maternal medication usually compatible with breast-feeding
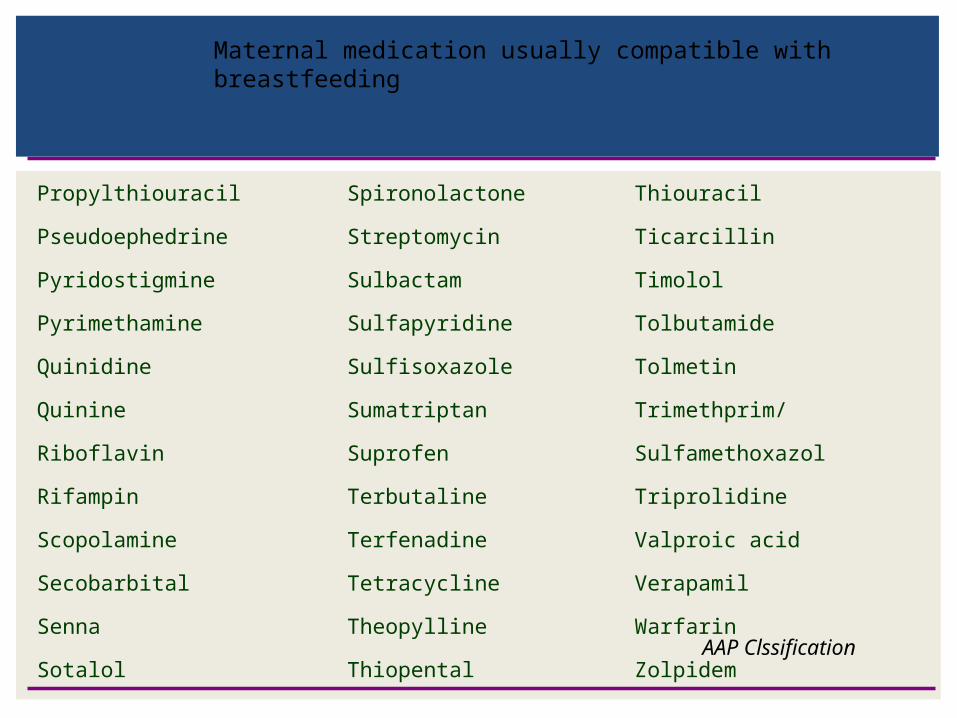
PropylthiouracilPseudoephedrinePyridostigminePyrimethamineQuinidineQuinineRiboflavinRifampinScopolamineSecobarbitalSennaSotalol
SpironolactoneStreptomycinSulbactamSulfapyridineSulfisoxazoleSumatriptanSuprofenTerbutalineTerfenadineTetracyclineTheopyllineThiopental
ThiouracilTicarcillinTimololTolbutamideTolmetinTrimethprim/SulfamethoxazolTriprolidineValproic acidVerapamilWarfarinZolpidem
AAP Clssification
Maternal medication usually compatible with breastfeeding

condition Recommended agents Use with caution
Allegic rhinitis BeclomethasoneFluticasone, cromolyn
Depression Sertraline, Paroxetine Fluoxetine,
Diabets Insulin, GlyburideTolbutamide
MetforminThiazolinediones
Asthma Cromolyn, Nedocromil
Pain Ibuprofen, Morphinacetaminophen
Naproxenmeperidine
Contraception Barrier method Estrogen-containing contraceptives
Epilepsy Phenytoin, Carbamazepine Phenobarbital
Chaves RG 2004
Medications commonly prescribed for maternal ailments during breastfeeding

Passive diffusionActive transport against a concentration gradientTranscellular diffusion
METHODS OF DRUG TRANSFER INTO MILK

1. Passive diffusion
2. Molecular weight
3. Protein binding
4. Lipid solubility
5. Half life
6. Oral bioavailability
약물 역동학적 인자

Short acting
Highly protein bound
Low lipid solubility
High molecular weight
No active metabolites
Low oral bioavailability
Route of administration
CHOICE OF DRUG