杨达雅 中山一院心血管内科 郭晓刚 中山一院黄埔院区心血管内科 王月刚...
DESCRIPTION
杨达雅 中山一院心血管内科 郭晓刚 中山一院黄埔院区心血管内科 王月刚 南方医院心血管内科. 66yr/F HPI Exertional dyspnea and edema of lower extremities for one month PE BP 162/98 mmHg, HR 100 bpm. Moderately distended jugular vein Fine crackles over lower lung fields. Enlarged heart boarder - PowerPoint PPT PresentationTRANSCRIPT
杨达雅杨达雅中山一院心血管内科中山一院心血管内科
郭晓刚郭晓刚中山一院黄埔院区心血管内科中山一院黄埔院区心血管内科
王月刚王月刚南方医院心血管内科南方医院心血管内科

66yr/F66yr/F HPIHPI◦Exertional dyspnea and edema of lower extremities Exertional dyspnea and edema of lower extremities
for one monthfor one month PEPE◦BP 162/98 mmHg, HR 100 bpm. BP 162/98 mmHg, HR 100 bpm. ◦Moderately distended jugular vein Moderately distended jugular vein ◦Fine crackles over lower lung fields.Fine crackles over lower lung fields.◦Enlarged heart boarder Enlarged heart boarder ◦A III/VI diastolic murmur over LLSBA III/VI diastolic murmur over LLSB◦A symmetric pitting edema of legs and anklesA symmetric pitting edema of legs and ankles

PMHPMH◦ Hypertension Hypertension for 10+ yrs, inadequately controlled (150-for 10+ yrs, inadequately controlled (150-
160/80-90mmHg)160/80-90mmHg)◦ Type 2 DM Type 2 DM for 7 yrs, well controlled with Insulinfor 7 yrs, well controlled with Insulin◦ Ischemic stroke Ischemic stroke 5 yrs ago, well recovered, with minimal 5 yrs ago, well recovered, with minimal
neurological sequelaeneurological sequelae◦ GoutGout for 3 yrs, several acute attacks for 3 yrs, several acute attacks
Current medications:Current medications:◦ Nifedipine GITS 30 mg P.O., QDNifedipine GITS 30 mg P.O., QD◦ Aspirin 100 mg P.O., QDAspirin 100 mg P.O., QD◦Multiple-component Insulin RegimenMultiple-component Insulin Regimen
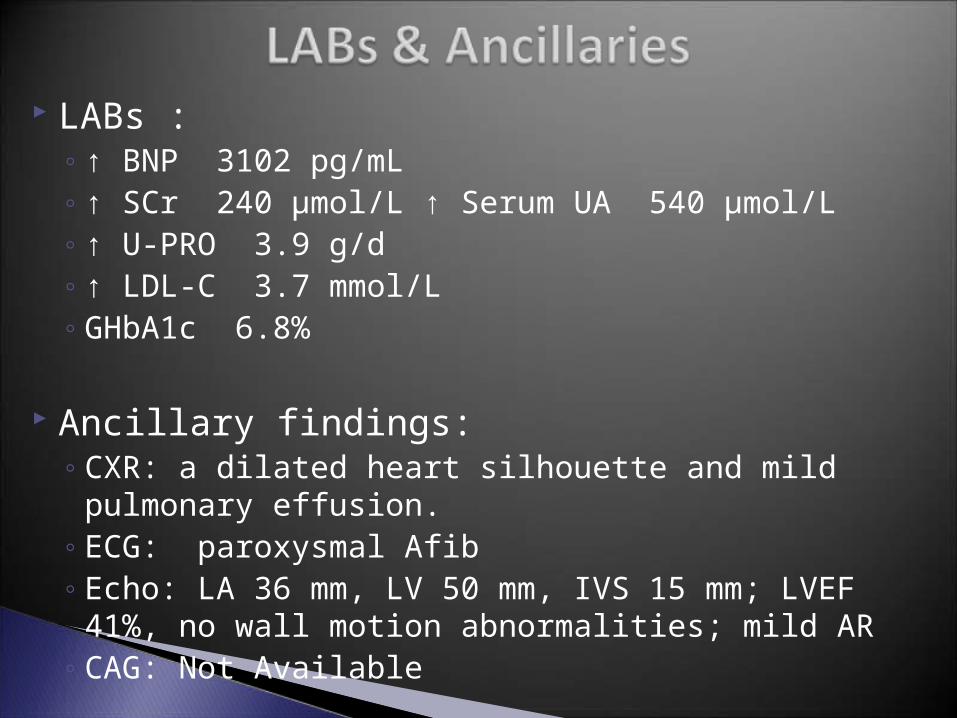
LABs : ◦↑ BNP 3102 pg/mL◦↑ SCr 240 µmol/L ↑ Serum UA 540 µmol/L◦↑ U-PRO 3.9 g/d◦↑ LDL-C 3.7 mmol/L◦GHbA1c 6.8%
Ancillary findings:◦ CXR: a dilated heart silhouette and mild pulmonary effusion.◦ ECG: paroxysmal Afib ◦ Echo: LA 36 mm, LV 50 mm, IVS 15 mm; LVEF 41%, no wall
motion abnormalities; mild AR◦ CAG: Not Available

Working Diagnoses:Working Diagnoses:◦ Acute LV FailureAcute LV Failure◦ HypertensionHypertension◦ Paroxysmal AfibParoxysmal Afib◦ Type 2 DM – Diabetic NephropathyType 2 DM – Diabetic Nephropathy◦ Prior StrokePrior Stroke◦ GoutGout
Treatments:Treatments:◦ Oxygen Rx, IV furosemide, digitalis, and IV nitroglycerine, Oxygen Rx, IV furosemide, digitalis, and IV nitroglycerine,
etc. all of which was well-responded.etc. all of which was well-responded.◦Metoprolol was added and titrated after stablizationMetoprolol was added and titrated after stablization

Adequate BP Control Antithrombotic Rx for Paroxysmal Afib
◦HF, Afib and probably stroke are more or less the direct results of, or at least precipitating factors of, inadequate BP control
◦Benefits of BP control concerning CV mortality are well-established and overwhelming
BP Target: <130/80mmHg
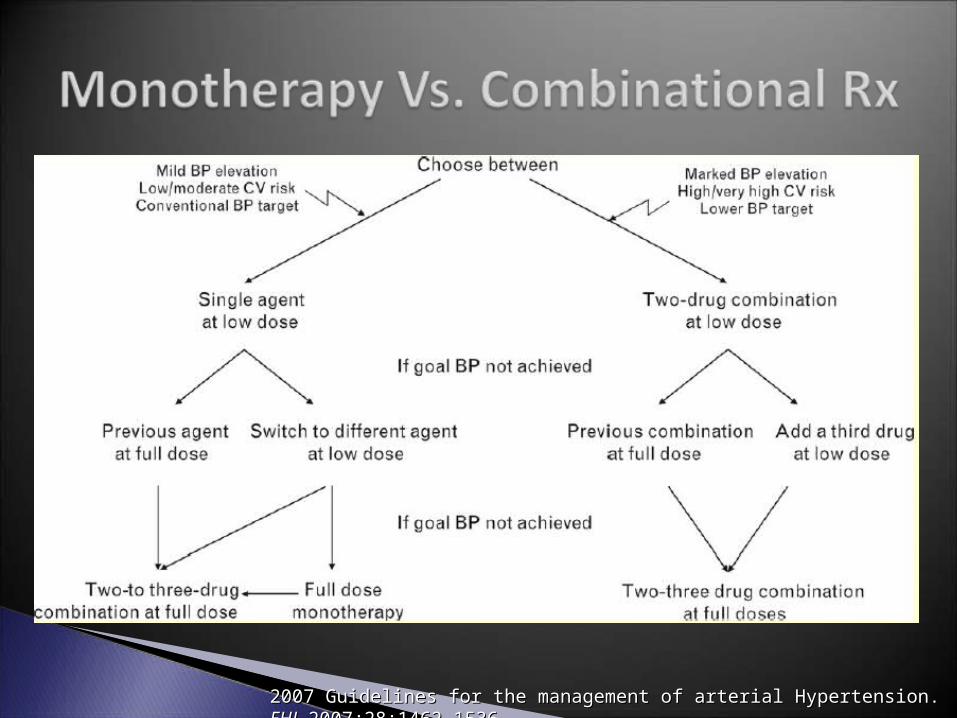
2007 Guidelines for the management of arterial Hypertension. 2007 Guidelines for the management of arterial Hypertension. EHJEHJ 2007;28:1462-1536 2007;28:1462-1536


2007 Guidelines for the management of arterial Hypertension. 2007 Guidelines for the management of arterial Hypertension. EHJEHJ 2007;28:1462-1536 2007;28:1462-1536

2007 Guidelines for the management of arterial Hypertension. 2007 Guidelines for the management of arterial Hypertension. EHJEHJ 2007;28:1462-1536 2007;28:1462-1536
Serum UA <357 μmol/L - ↓ risk of gouty attacks Losartan has uricosuric effects (7-8%), though evidence
on the clinical outcome of gout is less well established.
Perez-Ruiz F, Lioté F. Lowering serum uric acid levels: what is the optimal target for improving clinical outcomes in gout? Arthritis Rheum 2007;57:1324-8 Takahashi S, Moriwaki Y, Yamamoto T, Tsutsumi Z, Ka T, Fukuchi M. Effects of combination treatment using anti-hyperuricaemic agents with fenofibrate and/or losartan on uric acid metabolism. Ann Rheum Dis 2003;62:572-5

Compelling Indications: ◦HF, DM, proteinuria, Afib◦ACEI / ARB class
Hyperuricemia◦Losartan 50mg Qd
“Multi-tasking”

2010 Guidelines for the management of atrial fibrillation. 2010 Guidelines for the management of atrial fibrillation. EHJEHJ (31):2369-2429
The indication for Oral Anticoagulant (OAC) is independent of the types of Afib.

CHADS2:- Cardiac Failure- Hypertension- Age > 75yrs- Diabetes- Stroke / TIA (doubled)
- If >=2, VKA indicated (for an INR of 2.0-3.0)- If <2, Aspirin indicated

Lasix 20mg QdLasix 20mg Qd Spiranolactone 20mg QdSpiranolactone 20mg Qd Amlodipine 5mg QdAmlodipine 5mg Qd Losartan 50mg QdLosartan 50mg Qd Metoprolol 12.5mg QdMetoprolol 12.5mg Qd Digoxin 0.125mg QdDigoxin 0.125mg Qd Warfarin 3mg QdWarfarin 3mg Qd Rosuvastatin 10mg QNRosuvastatin 10mg QN Insulin RxInsulin Rx
If target BP control is not achieved by monotherapy, a If target BP control is not achieved by monotherapy, a combinational approach is warranted.combinational approach is warranted.
Choice of anti-hypertensive drugs should be dictated by Choice of anti-hypertensive drugs should be dictated by associated clinical co-morbidities.associated clinical co-morbidities.
Risk of stroke for pts with paroxysmal Afib is similar as in Risk of stroke for pts with paroxysmal Afib is similar as in other types of Afib.other types of Afib.
The CHADSThe CHADS22 Score is used clinically as an initial, rapid, Score is used clinically as an initial, rapid, easy-to-remember means of assessing stroke risk for Afib.easy-to-remember means of assessing stroke risk for Afib.
