creation of a patient-centric patient lay summary in the...
TRANSCRIPT

42 | December 2017 Medical Writing | Volume 26 Number 4
Creation of a patient-centric patientlay summary in the local languageSatoru Mogami, Mikiko Noyes, Rika Morita,Atsuko Shiotsuki, Toshiaki Hagi, Hiroe Hasegawa, Chikara Iida, Mina Izuchi,Fumiharu Naganeo, Junko Tanabe, Kyoko Uno, Osamu Suga, andChikara KikuchiPfizer Japan Inc., Tokyo, Japan
Correspondence to:Satoru MogamiDevelopment Japan, Pfizer Japan Inc. 3-22-7 Yoyogi, Shibuya-ku, Tokyo, Japan 151-8589+81 90 6009 [email protected]
AbstractPrior to this project, no patient lay summary(PLS) had ever been developed locally inJapan. In order to create a PLS that is moretailored to local patients, we attempted todevelop one in and for Japanese. Such PLSwas drafted based on the disclosed summaryof the clinical study report. We took acomposite approach in refining the PLS byresearching on lay language and patient-friendly designs. At the same time, weensured scientific accuracy throughconsultation with experts such as physiciansand statisticians, practised diligence onregulatory and legal aspects, and incorporatedpatient’s voice by consulting a local patientadvocacy group. We successfully created aPLS in the Japanese language for the firsttime, which was more patient centric thanthose translated from another language.
While summary results of clinical trials havecommonly been posted on global websites suchas clinicaltrials.gov1 and EU Clinical TrialsRegister,2 the European Union Clinical TrialRegulation No. 536/20143 states that sharingclinical trial results to study participants in theform of a lay language summary is also animportant endeavour. In Japan so far, we havedistributed patient lay summaries (PLSs) for twoclinical trials,4 which were originally written in
English and translated into Japanese by anexternal organisation. In order to create PLSs thatare more tailored to local patients, we havepioneered creating a Japanese PLS starting fromscratch.
We formed two teams: One was responsiblefor researching on the characteristics of laylanguage, developing a template, communicatingwith a patient group, and considering legal andregulatory aspects; the other took charge ofdrafting a PLS. The two teams collaborated inrefining the PLS and developing a process of PLSpreparation. The team members voluntarilyparticipated in the project and were consisted ofmedical writers and members of the documentmanagement group.
Developing the templateTo develop a patient-friendly template, we firstgathered patient information materials at localhospitals and clinics and critically evaluated theirdesigns concerning legibility and readability. Wealso looked for relevant guidelines anddesign principles. We adopted theconcept of “universal design” foreffective communication5 and inparticular considered the fol -low ing aspects: � Font and style of text: We
chose to use a recommended Japanese fontMeiryo primarily, as it has a very cleartypeface that maintains high legibility even inbold style. Also to enhance legibility, we useda font size larger than what we wouldnormally use for regulatory documents (i.e.,12-point size was used for the main text of thePLS while 10.5-point size would normally beused for regulatory documents).
� Line spacing: Wider line spacing was used tooptimise legibility and readability. This alsoallowed us to place a Japanese reading aid (inform of syllabic scripts) above some Kanjicharacters, which are similar to Chinesecharacters, in order to show how this textshould be read. This was a part of the attemptto keep the language level equivalent to aJapanese junior high school graduate.
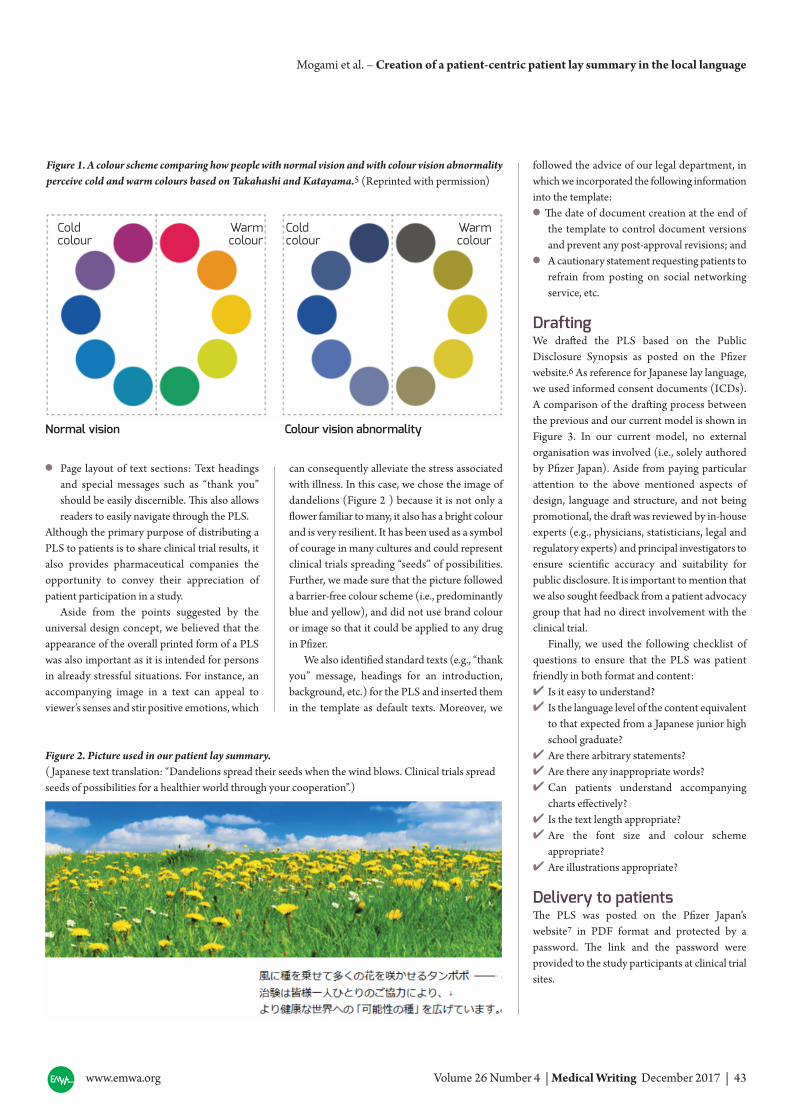
� Colours: In particular, a barrier-free colourscheme (see Figure 1) was studied to makesure that even patients with colour visionabnormality can appreciate the PLS without
difficulty. People with colour visionabnormality have difficulty differ -
en tiating among cold colours orwarm colours. For instance, it ishard for them to distinguishbet ween red and green, purpleand blue, or orange and yellow.
We adoptedthe concept of
“universal design” for effective
communication.
www.emwa.org Volume 26 Number 4 | Medical Writing December 2017 | 43
Mogami et al. – Creation of a patient-centric patient lay summary in the local language
� Page layout of text sections: Text headingsand special messages such as “thank you”should be easily discernible. This also allowsreaders to easily navigate through the PLS.
Although the primary purpose of distributing aPLS to patients is to share clinical trial results, italso provides pharmaceutical companies theopportunity to convey their appreciation ofpatient participation in a study.
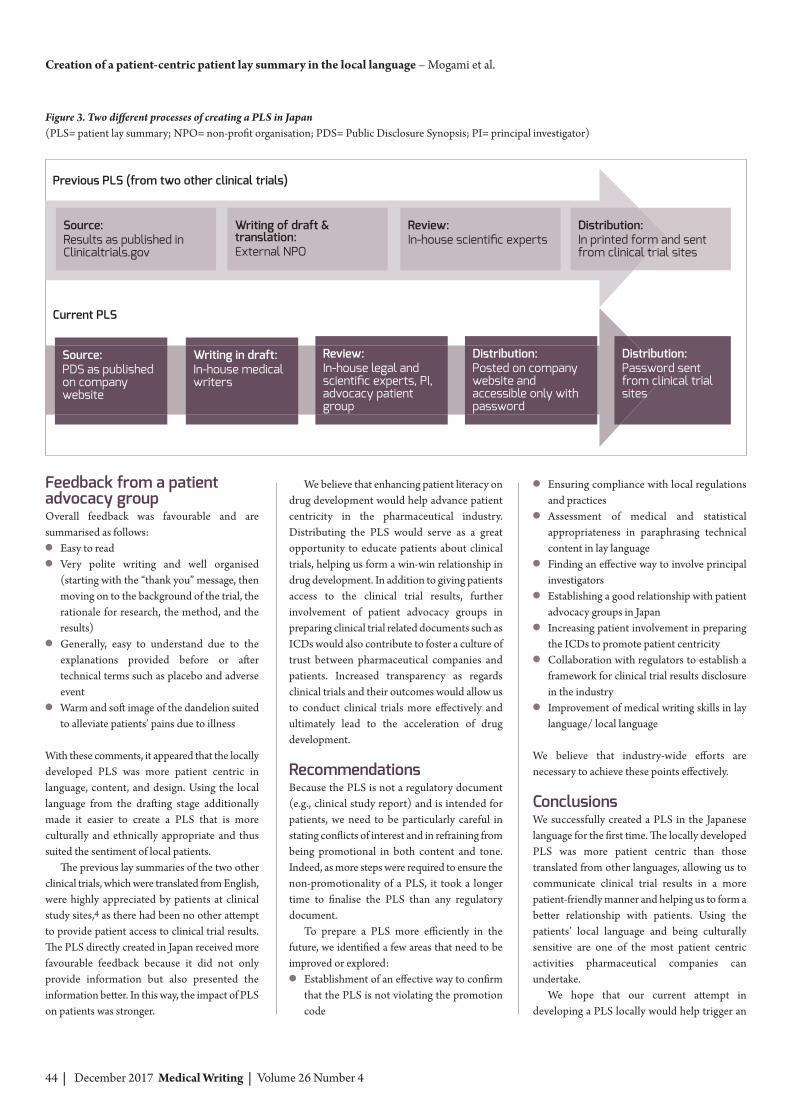
Aside from the points suggested by theuniversal design concept, we believed that theappearance of the overall printed form of a PLSwas also important as it is intended for personsin already stressful situations. For instance, anaccompanying image in a text can appeal toviewer’s senses and stir positive emotions, which
can consequently alleviate the stress associatedwith illness. In this case, we chose the image ofdandelions (Figure 2 ) because it is not only aflower familiar to many, it also has a bright colourand is very resilient. It has been used as a symbolof courage in many cultures and could representclinical trials spreading “seeds” of possibilities.Further, we made sure that the picture followeda barrier-free colour scheme (i.e., predominantlyblue and yellow), and did not use brand colouror image so that it could be applied to any drugin Pfizer.
We also identified standard texts (e.g., “thankyou” message, headings for an introduction,background, etc.) for the PLS and inserted themin the template as default texts. Moreover, we
followed the advice of our legal department, inwhich we incorporated the following informationinto the template:� The date of document creation at the end of
the template to control document versionsand prevent any post-approval revisions; and
� A cautionary statement requesting patients torefrain from posting on social networkingservice, etc.
DraftingWe drafted the PLS based on the PublicDisclosure Synopsis as posted on the Pfizerwebsite.6 As reference for Japanese lay language,we used informed consent documents (ICDs). A comparison of the drafting process betweenthe previous and our current model is shown inFigure 3. In our current model, no externalorganisation was involved (i.e., solely authoredby Pfizer Japan). Aside from paying particularattention to the above mentioned aspects ofdesign, language and structure, and not beingpromotional, the draft was reviewed by in-houseexperts (e.g., physicians, statisticians, legal andregulatory experts) and principal investigators toensure scientific accuracy and suitability forpublic disclosure. It is important to mention thatwe also sought feedback from a patient advocacygroup that had no direct involvement with theclinical trial.
Finally, we used the following checklist ofquestions to ensure that the PLS was patientfriendly in both format and content:� Is it easy to understand? � Is the language level of the content equivalent
to that expected from a Japanese junior highschool graduate?
� Are there arbitrary statements?� Are there any inappropriate words?� Can patients understand accompanying
charts effectively?� Is the text length appropriate?� Are the font size and colour scheme
appropriate?� Are illustrations appropriate?
Delivery to patientsThe PLS was posted on the Pfizer Japan’swebsite7 in PDF format and protected by apassword. The link and the password wereprovided to the study participants at clinical trialsites.
Figure 2. Picture used in our patient lay summary. ( Japanese text translation: “Dandelions spread their seeds when the wind blows. Clinical trials spreadseeds of possibilities for a healthier world through your cooperation”.)
Cold Warmcolour colour
Cold Warmcolour colour
Normal vision Colour vision abnormality
Figure 1. A colour scheme comparing how people with normal vision and with colour vision abnormalityperceive cold and warm colours based on Takahashi and Katayama.5 (Reprinted with permission)
44 | December 2017 Medical Writing | Volume 26 Number 4
Feedback from a patientadvocacy groupOverall feedback was favourable and aresummarised as follows: � Easy to read� Very polite writing and well organised
(starting with the “thank you” message, thenmoving on to the background of the trial, therationale for research, the method, and theresults)
� Generally, easy to understand due to theexplanations provided before or aftertechnical terms such as placebo and adverseevent
� Warm and soft image of the dandelion suitedto alleviate patients’ pains due to illness
With these comments, it appeared that the locallydeveloped PLS was more patient centric inlanguage, content, and design. Using the locallanguage from the drafting stage additionallymade it easier to create a PLS that is moreculturally and ethnically appropriate and thussuited the sentiment of local patients.
The previous lay summaries of the two otherclinical trials, which were translated from English,were highly appreciated by patients at clinicalstudy sites,4 as there had been no other attemptto provide patient access to clinical trial results.The PLS directly created in Japan received morefavourable feedback because it did not onlyprovide information but also presented theinformation better. In this way, the impact of PLSon patients was stronger.
We believe that enhancing patient literacy ondrug development would help advance patientcentricity in the pharmaceutical industry.Distributing the PLS would serve as a greatopportunity to educate patients about clinicaltrials, helping us form a win-win relationship indrug development. In addition to giving patientsaccess to the clinical trial results, furtherinvolvement of patient advocacy groups inpreparing clinical trial related documents such asICDs would also contribute to foster a culture oftrust between pharmaceutical companies andpatients. Increased transparency as regardsclinical trials and their outcomes would allow usto conduct clinical trials more effectively andultimately lead to the acceleration of drugdevelopment.
RecommendationsBecause the PLS is not a regulatory document(e.g., clinical study report) and is intended forpatients, we need to be particularly careful instating conflicts of interest and in refraining frombeing promotional in both content and tone.Indeed, as more steps were required to ensure thenon-promotionality of a PLS, it took a longertime to finalise the PLS than any regulatorydocument.
To prepare a PLS more efficiently in thefuture, we identified a few areas that need to beimproved or explored: � Establishment of an effective way to confirm
that the PLS is not violating the promotioncode
� Ensuring compliance with local regulationsand practices
� Assessment of medical and statisticalappropriateness in paraphrasing technicalcontent in lay language
� Finding an effective way to involve principalinvestigators
� Establishing a good relationship with patientadvocacy groups in Japan
� Increasing patient involvement in preparingthe ICDs to promote patient centricity
� Collaboration with regulators to establish aframework for clinical trial results disclosurein the industry
� Improvement of medical writing skills in laylanguage/ local language
We believe that industry-wide efforts arenecessary to achieve these points effectively.
ConclusionsWe successfully created a PLS in the Japaneselanguage for the first time. The locally developedPLS was more patient centric than thosetranslated from other languages, allowing us tocommunicate clinical trial results in a morepatient-friendly manner and helping us to form abetter relationship with patients. Using thepatients’ local language and being culturallysensitive are one of the most patient centricactivities pharmaceutical companies canundertake.
We hope that our current attempt indeveloping a PLS locally would help trigger an
Creation of a patient-centric patient lay summary in the local language – Mogami et al.
Figure 3. Two different processes of creating a PLS in Japan(PLS= patient lay summary; NPO= non-profit organisation; PDS= Public Disclosure Synopsis; PI= principal investigator)
Previous PLS (from two other clinical trials)
Current PLS
Source:Results as published inClinicaltrials.gov
Writing of draft &translation:External NPO
Review:In-house scientific experts
Distribution:In printed form and sentfrom clinical trial sites
Source:PDS as publishedon companywebsite
Writing in draft:In-house medicalwriters
Review:In-house legal andscientific experts, PI,advocacy patientgroup
Distribution:Posted on companywebsite andaccessible only withpassword
Distribution:Password sentfrom clinical trialsites

www.emwa.org Volume 26 Number 4 | Medical Writing December 2017 | 45
increase in the distribution of such summaries inJapan. We believe that locally developedsummaries would bring more benefits to bothpatients and the pharma ceutical industry,especially in more culturally and linguisticallydiverse regions such as the EU.
Conflicts of interest anddisclaimersThe authors are employed by Pfizer Japan Inc.
References1. ClinicalTrials.gov. Clinical TrialsRegistry
and Results Posting Database. 2017 [cited2016 September 1]. Available from:https://clinicaltrials.gov.
2. European Medicines Agency. EuropeanClinical Trials Database (EudraCT) V10.2017 [cited 2016 August 10]. Availablefrom: https://eudract.ema.europa.eu/index.html.
3. Official Journal of the European Union.Regulation (EU) No 536/2014 of theEuropean Parliament and of the Council of16 April 2014 on Clinical Trials on MedicinalProducts for Human Use, and RepealingDirective 2001/20/EC. 2014 [cited 2016August 5]. Available from: http://ec.europa.eu/health/files/eudralex/vol-1/reg_2014_
536/reg_2014_536_ en.pdf.4. Suga O, Take Y, Ishiguro T, Izuchi M, Udo
K, Shibata A, et al. Communicating trialresults to study volunteers in Japan [inJapanese]. Regulatory Science of MedicalProducts. 2016;6 Suppl:54.
5. Takahashi Y, Katayama N. Design tocomunicate: universal design for researchpresentation. 2012 [cited 2016 September1] Available from: http://tsutawarudesign.web.fc2.com/.
6. Pfizer Inc. Clinical study report synopses[cited 2016 September 1] Available from:http://www.pfizer.com/science/research_
clinical_trials/trial_results.7. Pfizer Japan Inc. Patient lay summary [cited
2016 December 1] Available from:http://www.pfizer.co.jp/development/patient_lay/index2.html.
Author informationSatoru Mogami is the Director of MedicalWriting at Pfizer Japan. He has over 20 yearsof experience in medical writing. He is astrong advocate for patient-centricity and apromoter of clinical trial results disclosures inthe Japanese pharmaceutical industry.
Mikiko Noyes worked as a Japanese-Englishpharmaceutical translator before joiningPfizer. She now has over 10 years ofexperience in regulatory writing. Her interestsinclude medical writing for lay audiences aswell as the patient-centric document designfor effective communication.
Rika Morita is a member of the MedicalWriting Group at Pfizer Japan. She has over10 years of experience in regulatory writing,with keen interest in advancing patientcentricity in the pharmaceutical industry bysharing clinical trial results with participants.
Atsuko Shiotsuki is a member of theRegulatory Editing Group at Pfizer Japan. Shehas over 10 years of experience in regulatoryediting and is a specialist in editing andpublishing of investigator brochures. Herinterests include delivering accurateinformation to patients in a timely manner.
Toshiaki Hagi has more than 20 years ofexperience in regulatory documentation andhas been working on medical writing andediting activities for the last 18 years.
Hiroe Hasegawa has over 20 years ofexperience in clinical development and hasbeen a medical writer for the past two years.She is a subject matter expert on clinical trialdisclosure in Pfizer Japan and has a stronginterest in increasing transparency in drugdevelopment.
Chikara Iida has over 10 years of experiencein clinical development and has been with theMedical Writing Group for the past 2 years.Having worked in the development operationfor many years, he is knowledgeable aboutinteracting with patient groups and is an advo -cate for patient-centred drug development.
Mina Izuchi is a member of the MedicalWriting Group at Pfizer Japan. She has over10 years of experience as a regulatory writermainly in the area of vaccines. She led theconstruction of the website for posting thepatient lay summary.
Fumiharu Naganeo is a member of theDocument Management Group at PfizerJapan. After 4 years of medical writingexperience, he now collaborates with medicalwriters as a regulatory dossier coordinator. Heis an expert on eCTD submission and thesubsequent disclosure.
Junko Tanabe has over 10 years ofexperience in regulatory editing anddocument management. Being an expert on“submission-ready” documents, she has astrong interest in “universal” documentdesign for providing information in a patient-friendly manner.
Kyoko Uno started her career in thepharmaceutical industry in developmentoperations. She now has over 10 years ofexperience in medical writing. She hasextensive knowledge of submission require -ments in Japan, particularly Common Tech -nical Document (CTD) Module 1 and thepublic disclosure of regulatory documents.
Osamu Suga is the head of the DocumentManagement Group at Pfizer Japan. He was amedical writer for about 16 years and was theformer head of the Medical Writing Group.He led the pilot to create a patient laysummary for the first time in Japan.
Chikara Kikuchi has more than 20 years ofexperience in regulatory affairs and iscurrently the Senior Director, RegulatoryAffairs, at Pfizer Japan and Vice-Chair of theDrug Evaluation Committee in the JapanPharmaceutical Manufacturers Association.
Mogami et al. – Creation of a patient-centric patient lay summary in the local language